ARTÍCULOS ORIGINALES
Do resin cements influence the cuspal deflection of teeth restored with composite resin inlays?
Helen C.V. da Rosa1, Maurem L. Marcondes1, Niélli C. de Souza1, João B. B. Weber2, Ana M. Spohr3
1 Department of Restorative Dentistry, School of Dentistry, Pontifical Catholic University of Rio Grande do Sul, Brazil.
2 Department of Preventive Dentistry, Pontifical Catholic University of Rio Grande do Sul, Porto Alegre, Brazil.
3 Department of Dental Materials, School of Dentistry, Pontifical Catholic University of Rio Grande do Sul, Brazil.
CORRESPONDENCE Dr. Ana Maria Spohr PUCRS – School of Dentistry, Block 6 Avenida Ipiranga, 6681, 90619-900 Porto Alegre, RS, Brazil. E-mail: ana.spohr@pucrs.br
ABSTRACT
The aim of this study was to evaluate the influence of different resin cements on the cuspal deflection of endodontically treated teeth restored with composite resin inlays. Sixty upper premolars were randomly divided into five groups (n=12): 1 – sound teeth; 2 – cavity; 3 - Rely X ARC; 4 – RelyX Unicem; 5 – SeT. The teeth from groups 2, 3, 4 and 5 received a MOD preparation and endodontic treatment. Impressions were made with vinyl polysiloxane and poured using type IV die stone in groups 3, 4 and 5. Inlays with composite resin were built over each cast and luted with the resin cements. A 200 N load was applied on the occlusal surface, and cuspal deflection was measured using a micrometer. After 24 h, cuspal deflection was measured again using a 300 N load. The Student t-test showed that there was no statistically significant difference between the 200 N and 300 N occlusal loads only for the sound teeth group (p = 0.389) and the RelyX ARC group (p = 0.188). ANOVA and Tukey'test showed that the sound teeth had the lowest mean cuspal deflection, differing statistically from the other groups (p<0.05). The highest cuspal deflections were obtained in the SeT group and the cavity group, with no statistical difference between them. Intermediate values were obtained in RelyX ARC group and RelyX Unicem group, which differed statistically. The self-adhesive resin cements RelyX Unicem and SeT showed less capacity to maintain the stiffness of the tooth/restoration complex than the conventional resin cement RelyX ARC.
Key words: Endodontics; Resin cements.
RESUMO
Os cimentos resinosos influenciam a deflexão de cúspides de dentes restaurados com inlays em resina composta?
O objetivo deste estudo foi avaliar a influencia de diferentes cimentos resinosos na deflexao de cuspides de dentes tratados endodonticamente e restaurados com inlays em resina composta. Sessenta pre-molares foram divididos aleatoriamente em cinco grupos (n=12): grupo 1 – dentes higidos; 2 – cavidade; 3 - Rely X ARC; 4 – RelyX Unicem; 5 – SeT. Os dentes dos grupos 2, 3, 4 e 5 receberam preparos cavitarios MOD e tratamento endodontico. Foram realizadas moldagens com silicone por adicao nos grupos 3, 4 e 5, seguido de vazamento de gesso tipo IV. Inlays em resina composta foram construidas sobre os modelos de gesso, sendo as inlays cimentadas com os cimentos resinosos. Uma carga de 200 N foi aplicada na face oclusal, e a deflexao de cuspide foi medida usando um micrometro. Apos 24 h, a deflexao de cuspide foi medida novamente sob carga de 300 N. De acordo com o teste t-Student, nao houve diferenca estatistica na deflexao de cuspides apenas para o grupo dos dentes higidos (p = 0.389) e o grupo do RelyX ARC (p = 0.188) quando comparada as duas cargas. De acordo com ANOVA e o tese de Tukey, os dentes higidos tiveram a menor media de deflexao de cuspides, diferindo estatisticamente dos outros grupos (p<0.05). A maior deflexao de cuspides foi obtida com o grupo SeT e o grupo cavidades, nao diferindo estatisticamente entre si. Valores intermediarios foram obtidos para os grupos RelyX ARC e RelyX Unicem, diferindo estatisticamente entre si. Os cimentos resinosos autoadesivos RelyX Unicem e SeT mostraram menor capacidade de manter a rigidez do complexo dente/restauracao em comparacao com o cimento resinoso RelyX ARC.
Palavras-chave: Tratamento endodontico; Cimento resinoso.
INTRODUCTION
As a result of their structural design, posterior teeth
naturally suffer cuspal deflection under load. When
endodontic treatment and mesio–occlusal–distal
(MOD) preparations are performed, this trend
towards cuspal deflection under masticatory loads
is increased 1,2 due to the decrease in the stiffness of
the tooth 3. It is a consequence of the removal of
dental tissues, which leads to greater fragility of the
dental structure 4,5.
Numerous techniques and restorative materials have
been indicated to recover the stiffness of endodontically
treated teeth 6,7. The most frequently used materials
are composite resins and ceramics, due to esthetic
demands. In the case of composite resin restorations,
the indirect technique is considered the best treatment
option to restore teeth with large cavities and to overcome
polymerization shrinkage 8. These indirect
restorations are luted with adhesive materials, such as
adhesive systems associated with resin cements,
which favor reinforcement of the weakened tooth 9-11.
The conventional adhesive luting procedure consists
of applying an adhesive system followed by a resin
cement. However, self-adhesive resin cements have
gained popularity with clinicians because they are easy
to use, and the luting procedure takes less time than
resin cements, which require the application of an
adhesive system. Without the adhesive system, part of
the sensitivity of the technique is eliminated 12,13.
Self-adhesive resin cements interact superficially
with tooth hard tissues, and the formation of a
hybrid layer or resin tags was not observed 14-16.
Self-adhesive resin cements have lower bond
strength with enamel than do resin cements requiring
an adhesive system 12, 17. In relation to dentin,
studies have shown that self-adhesive resin cements
perform comparably to multistep systems on coronal
dentin 12, 14, 17- 19. In contrast, other studies have
shown significantly lower bond strengths of these
materials to dentin 20- 22.
In an inlay restoration, the luting material occupies
the space between the restoration and the tooth, and
is responsible for connecting these different substrates.
Regardless of the luting technique, the
tooth/restoration complex must be capable of restoring
the stiffness of the original tooth to a certain
degree, in order to decrease mechanical fatigue of
the cusps 23, which increases with higher occlusal
loads 1. However, there is no study showing the influence
of resin cements on cuspal deflection under different
occlusal loads.
The aim of this study was to evaluate the influence
of three resin cements on cuspal deflection, under
two different occlusal loads, of endodontically
treated maxillary premolars restored with composite
resin inlays. This study was conducted under the
hypotheses that there are differences in the amount
of cuspal deflection between inlays luted with the
different resin cements.
MATERIALS AND METHODS
MOD preparation
Sixty sound maxillary first premolars, extracted for
therapeutic reasons, were obtained from a tooth bank
after the approval of the Ethics Committee of the Pontifical
Catholic University of Rio Grande do Sul. The
teeth were cleaned and disinfected in 10% thymol for
24 h and stored in 4° C distilled water. The water was
changed every week, and the teeth were used within
6 months. The buccal–palatal and mesio–distal
dimensions of each tooth were measured with a digital
caliper (Mitutoyo, Suzano, SP, Brazil). A variation
of 0.5 mm was allowed for each measurement to standardize
the dimensions of the teeth.
Each tooth was mounted vertically in a plastic cylinder
with self-cured acrylic resin (Jet Classico, Sao Paulo,
SP, Brazil), up to 2 mm below the cement–enamel junction
(CEJ). The teeth were randomly divided into 5
groups (n=12): Group 1, sound teeth (control); Groups
2, 3, 4, and 5, teeth with MOD preparation and
endodontic treatment. Group 2 was not restored, and
the other groups were restored with composite resin
inlays, which were luted with RelyX ARC (Group 3),
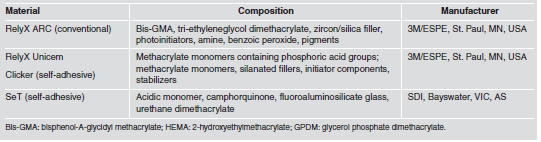
RelyX Unicem (Group 4), and SeT (Group 5). Table 1 shows the composition and manufacturer details of the
materials used.
Table 1: Resin cements used in the study.
A single operator performed the MOD preparations
using a standardized preparation machine. This device
consisted of a high-speed handpiece (Kavo, Joinville,
SC, Brazil) attached to a mobile base. The mobile base
moves vertically and horizontally, in 3 mm increments,
with the aid of a micrometer (Mitutoyo, Tokyo,
Japan). The long axis of the tooth was positioned vertically
on the preparation machine, and the tooth was
cut using a #4159 diamond bur (KG Sorensen,
Barueri, SP, Brazil) attached to the high-speed handpiece
under constant water and air cooling. The preparations
presented rounded internal angles, divergent
walls, and an occlusal box width of two-thirds of the
intercuspal distance. The depth of the proximal boxes
was located 1 mm above the CEJ. The preparations
had only buccal and palatal walls, and a common floor
from mesial to distal, so that the pulp floor of the
occlusal box and the gingival floor of the proximal
boxes were unified on the same level. The diamond
bur was replaced after every five preparations.
After the preparations were completed, endodontic
access was prepared with a #8 spherical carbide burr
(SS White, Lakewood, NJ, USA). The preparation of
the chamber was round and expulsive. Flexo-File files
(Kerr, Orange, CA, USA) from number 15 to 40 were
manually placed in the root canals to standardize the
preparation.
A 2.5% sodium hypochlorite solution was
used to irrigate and clean the root canal. After the root
canal preparation, all teeth were filled with gutta-percha
cones (Dentsply Maillefer, Ballaigues, Switzerland)
and N-Rickert endodontic sealer (Inodon, Porto
Alegre, RS, Brazil) using the lateral condensation
technique. Excess sealer was removed from the cavity
using a cotton pellet soaked in 70% ethanol. The
access to root canals was covered with gutta-percha.
Restorative procedures
Impressions of the preparations were taken with
Express XT polyvinyl siloxane (3M Espe, Saint
Paul, MN, USA) using individual trays made from
self-cured acrylic resin (Jet Classico, Sao Paulo, SP,
Brazil) with the putty/wash one-step technique. The
impression material was allowed to set for 10 min
before removal from the preparation. After 1 h, the
impressions were poured using Durone Type IV
stone (Dentsply, York, PA, USA). After 1 h, the
casts were removed from the impression, numbered
according to their group, and placed in dry storage.
Cavity surfaces were lined with two coats of a die
spacer, maintaining a distance of 1.0 mm to the marginal
areas. Four horizontal layers of Filtek
Z250XT composite resin (3M Espe, Saint Paul,
MN, USA) were inserted in the casts, with Thompson
spatulas no. 2 and 12, which resulted in a 90°
inclination between the internal slopes and cusps.
Each resin layer was light cured for 40 s. Restorations
were then light cured for 60 s on each free surface,
followed by finishing with flexible disks
(TDV, Pomerode, SC, Brazil) and 8093F and 8093
FF silicone tips (KG Sorensen, Cotia, SP, Brazil).
Throughout the experiment, a quartz-tungsten-halogen
curing unit (Optilux Plus, Ribeirao Preto, SP,
Brazil) was used for photopolymerization. The light
intensity was controlled by a radiometer (model
100, Demetron/Kerr, Danbury, CT, USA) in the
interval between 450 and 500 mW/cm2.
Luting procedures
The internal surfaces of the inlays were sandblasted
with 50 μm aluminum oxide for 5 s, followed by
silane application (Ceramic Primer, 3M Espe, Saint
Paul, MN, USA). In Group 3, Scotchbond Multi-
Purpose adhesive system (3M Espe, Saint Paul, MN,
USA) was applied. The tooth preparations were
etched with 37% phosphoric acid for 15 s, followed
by rinsing with air and water spray for 15 s. Excess
water was removed with absorbent paper. A layer of
primer was applied, followed by gentle air drying
for 5 s. Then the bond was applied with a microbrush
and light cured for 10 s. Equal lengths of base and
catalyst pastes of RelyX ARC resin cement were
mixed for 15 s and put on the inlay and preparation.
In Group 4, equal quantities of base and catalyst
pastes of RelyX Unicem were mixed and applied
on the inlay and preparation. In Group 5, the internal
content of a capsule of SeT was activated for 10
s and applied on the inlay and preparation. In
Groups 3, 4, and 5, the inlay was placed on the
preparation and a 10 N load was applied by means
of a metallic tool. After 2 min, excess cement was
removed with a microbrush, followed by light curing
for 60 s on each free surface. The specimens
were stored in distilled water at 37° C for 72 h and
then submitted to the cuspal deflection test.
Cuspal deflection testing
Resin spheres (approximately 1.5 mm in diameter)
were fixed with adhesive on both cusps. Following
the methodology described by Gonzales-Lopez et al.2
the spheres were positioned on the cuspal apexes and
served as reference points for measuring the intercuspal
distance, using a precision micrometer (Mitutoyo,
Suzano, SP, Brazil) to the nearest 1 μm. A device was
used to fix the micrometer in the same position for
every measurement. Each specimen was attached to
the lower platen of a universal testing machine (Emic
DL-2000, EMIC, Sao Jose dos Campos, PR, Brazil),
and a steel sphere with an 8 mm diameter was used
to apply a 200 N occlusal load at a cross-head speed
of 0.5 mm/min. The load was applied parallel to the
long axis of the tooth, simultaneously contacting the
buccal and palatal cuspal inclines (Fig. 1). When the
200 N load was achieved, the machine was locked
and three consecutive measurements of the cuspal
deflection were made. The mean distance of the composite
resin spheres prior to application of the load
was subtracted from the mean distance of the spheres
after application of the load. Thus, the cuspal deflection
value was obtained. After 24 h, the cuspal deflection
was measured again using a 300 N load.

Fig. 1: Schematic figure of the cuspal deflection test: a) tooth;
b) resin spheres; c) micrometer.
Statistical analysis
All statistical analyses were performed using SPSS
version 10.0 (SPSS Inc., Chicago, IL, USA). After
data collection, cuspal deflection data were submitted
to the Kolmogorov–Smirnov normality test. To
compare the study groups under the same load, the
ANOVA and Tukey parametric statistical tests were
applied. To compare each group under the different
loads, student t-test for dependent samples was
applied. The significance level was 5%.
RESULTS
The ANOVA showed that there were statistically significant differences among the groups (p<0.05). For both occlusal loads, the sound teeth had the lowest mean cuspal deflection, differing statistically from the other groups. The highest cuspal deflections were obtained in SeT group and cavity group, with no statistical difference between them. Intermediate values were obtained in RelyX ARC group and RelyX Unicem group, which differed statistically. The Student t-test showed that there were statistically significant differences between the 200 N and 300 N occlusal loads for the cavity group (p = 0.002), the RelyX Unicem group (p = 0.000), and the SeT group (p = 0.004). There was no statistical difference for the sound teeth group (p = 0.389) or the RelyX ARC group (p = 0.188) (Table 2).
Table 2: Mean cuspal deflection and standard deviation of the groups under 200 N and 300 N loads.

DISCUSSION
The hypothesis was accepted, as there were differences
in cuspal deflection among the experimental
groups.
Premolars were used in this study because they have
an unfavorable anatomic shape, crown volume and
crown/root proportion, making them more susceptible to cusp fractures than other posterior teeth
when submitted to occlusal load 24. The dimensions
of the cavity preparation were standardized in all
groups, representing a clinical situation of advanced
caries, for which preparation becomes extensive.
Cuspal deflection is a non-destructive methodology
that verifies the deformation of the cusps when a
load is applied in the occlusal region. In this study,
a 200 N occlusal load was applied to perform the
cuspal deflection test. The 200 N load is the intermediate
value between 100 and 300 N, which corresponds
to the range of normal biting force for
maxillary premolars 25,26. Cuspal deflection under a
300 N load was also verified. According to Jantarat
et al.1, a load of up to 300 N can be applied without
the risk of tooth fracture. The results showed that
the application of greater occlusal load produced an
increase in intercuspal distance, in agreement with
the study by Gonzalez-Lopez et al. 2. This finding
proves that the deformation depends on the intensity
of the force applied 1.
The highest cuspal deflection was obtained for the
cavity group, and the lowest values for the sound
teeth.
This small cuspal deflection in sound teeth is
due to the very stiff behaviour of sound teeth under
load 1. Intact teeth with a complete enamel covering
are very stiff, and an occlusal load causes only
a small deformation. Sound teeth distribute loadgenerated
stress more homogeneously, because the
enamel is not appreciably deformed and the deformation
is transferred to the more resilient dentin 27.
When the continuity of the enamel is lost as a result
of preparation, the properties of the dentin play a
major role in cusp behaviour 28. Loss of dental structure
causes a decrease in tooth stiffness, and consequently
there is an increase in cuspal deflection
under occlusal loads 1,2. It is important to recover
the stiffness of the teeth after restoration. Nevertheless,
when the teeth were restored with composite
resin inlays and luted with RelyX ARC, RelyX
Unicem or SeT, none of the groups replicated the
stiffness of natural teeth.
Among the restored groups, RelyX ARC had the
lowest cuspal deflection. RelyX ARC is a conventional
resin cement that is applied with an adhesive
system. In this study, the preparation was etched with
37% phosphoric acid, followed by primer and bond
applications, which allow hybrid layer formation on
enamel 29 and dentin 30. The micro-mechanical retention
obtained with the hybrid layer may explain the
smaller cuspal deflection in the RelyX ARC group
than in the RelyX Unicem and SeT groups.
RelyX Unicem had the third lowest value of cuspal
deflection. It is a self-adhesive resin cement that
consists of alkaline fillers and specific multifunctional
phosphoric-acid methacrylates, which are
ionized at the time of mixing and which react with
the hydroxyapatite of the mineral tissues of the
tooth 31. On dentin, this material was unable to demineralize
or dissolve the smear layer completely, no
decalcification and infiltration of dentin occurred
and no hybrid layer or resin tag was observed 14,17,32.
The bond mechanism of RelyX Unicem to the tooth
appears to be more chemical rather than micromechanical
in nature. As RelyX Unicem have lower
bond strength to enamel 12,19 and dentin 20- 22 than do
multistep systems, the bond to the dental tissues
may not have been as strong as the bond encountered
at the DEJ or when a hybrid layer is formed.
This may explain the higher mean cuspal deflection
of the RelyX Unicem than of the sound teeth and
RelyX ARC groups.
An alternative for increasing the bond strength of
self-adhesive resin cements was to apply phosphoric
acid etching on the enamel 12,19,33, and polyacrylic
acid on the dentin 32,34 before the application of selfadhesive
resin cements. The presence of the smear
layer has been recognized as the weak link in bonding
self-adhesive resin cements 18,32. These pretreatments
represent an additional step in the application
of self-adhesive resin cements, which were developed
with the aim of simplifying the application
procedure. However, it would be interesting to conduct
the same study of cuspal deflection when specific
pretreatments are applied on enamel and
dentin before luting with RelyX Unicem, once all
the inlay margins of the prepared teeth were within
enamel, and a significant quantity of dentine was
exposed by the inlay preparation.
The self-adhesive resin cement SeT contains an acid
monomer that is responsible for etching the tooth surface.
However, it is not known specifically what type
of acid monomer is used, or whether it has a chemical
interaction with the tooth. In the study conducted
by Stona et al.32, the adhesion of SeT to dentin did
not withstand the cutting methodology used to obtain
the test specimens (beams) for evaluating microtensile
bond strength. It probably presented less interaction
with dental substrates than RelyX Unicem,
explaining the highest cuspal deflection.
Comparing 200-N and 300-N occlusal loads, RelyX
ARC was the only resin cement that allowed an
increase in cuspal deflection without statistical difference.
The micro-mechanical retention obtained
with the hybrid layer formed on enamel and dentin
by the 37% phosphoric acid etching and subsequent
adhesive polymerization is probably important for
bond stability when the load is increased.
In the case of inlay restoration, the stiffness of the
tooth tends to be restored when the material used
for luting bonds strongly with the tooth tissues and
restorative material, with the formation of a
monobloc restoration, in which two bond interfaces
are formed, corresponding to the tooth/luting
material and restoration/luting material.
Among the experimental groups in the present
study, variation occurred only at the tooth interface.
The same treatment was used at the restoration
interface, which consisted of sandblasting
with 50 μm aluminum oxide, followed by silane
application. According to Zang and Degrange 35,
the adhesion of self-adhesive resin cements to the
restorative material depends on the nature of the
multifunctional monomer contained in the formulation,
and these luting agents have potential for
specific adhesion to selective restorative substrates.
In addition, the different viscosities and
the different penetration capabilities of the RelyX
ARC, RelyX Unicem and SeT into surface irregularities
may have influenced the adhesion of the
resin cements to the inlay restoration.
The clinical importance of cuspal deflection is that
the greater the magnitude of this deflection, the
greater the deformation, and consequently, the
greater the possibility of fatigue failure. This type
of failure, characterized by fracture in the presence
of stress far below the maximum strength of the
restored tooth, occurs in most dental fractures 36.
The result obtained for cuspal deflection showed
that the self-adhesive resin cements RelyX Unicem
and SeT showed less capacity to maintain the stiffness
of the tooth/restoration complex than did the
conventional resin cement RelyX ARC, which may
foster greater longevity of the restored tooth. However,
clinical studies are necessary to confirm this
supposition.
1. Jantarat J, Palamara J, Messer H. An investigation of cuspal deformation and delayed recovery after occlusal loading. J Dent 2001;29:363–370.
2. Gonzalez-Lopez S, De Haro-Gasquet F, Vilchez-Dias MA, Ceballos L, Bravo M. Effect of restorative procedures and occlusal loading on cuspal deflection. Oper Dent 2006; 31:33-38.
3. Reeh ES, Messer HH, Douglas WH. Reduction in tooth stiffness as a result of endodontic and restorative procedures. J Endod 1989;15:512-516.
4. Shahrbaf S, Mirzakouchaki B, Oskoui SS, Kahnamoui MA. The effect of marginal ridge thickness on the resistance of endodontically-treated, composite restored maxillary premolars. Oper Dent 2007;32:285-290.
5. Bitter K, Meyer-Lueckel H, Fotiadis N, Blunck U, Neumann K, Kielbassa AM, Paris S. Influence of endodontic treatment, post insertion, and ceramic restoration on the fracture resistance of maxillary premolars. Int Endod J 2010;43:469-477.
6. Yamada Y, Tsubota Y, Fukushima S. Effect of restoration method on fracture resistance of endodontically treated maxillary premolars. Int J Prosthodont 2004;17:94-98.
7. Monga P, Sharma V, Kumar S. Comparison of fracture resistance of endodontically treated teeth using different coronal restorative materials: an in vitro study. J Conserv Dent 2009;12:154-159.
8. Reeves GW, Lentz DL, O'Hara JW, McDaniel MD, Tobert WE. Comparison of marginal adaptation between direct and indirect composites. Oper Dent 1992;17:210-214.
9. Dalpino PH, Francischone CE, Ishikiriama A, Franco EB. Fracture resistance of teeth directly and indirectly restored with composite resin and indirectly restored with ceramic materials. Am J Dent 2002;15:389-394.
10. Santos MJMC, Bezerra RB. Fracture resistance of maxillary premolars restored with direct and indirect adhesive techniques. J Can Dent Assoc 2005;71:585-585d.
11. Camacho GB, Goncalves M, Nonaka T, Osorio AB. Fracture strength of restored premolars. Am J Dent 2007;20:121-124.
12. Abo-Hamar SE, Hiller KA, Jung H, Federlin M, Friedl KH, Schmalz, G. Bond strength of a new universal self-adhesive resin luting cement to dentin and enamel. Clin Oral Investig 2005;9:161-167.
13. Burke FJT. Trends in indirect dentistry: 3. Luting materials. Dent Update 2005;32:257-260.
14. De Munck J, Vargas M, Van Landuyt K, Hikita K, Lambrechts P, Van Meerbeek B. Bonding of auto-adhesive luting material to enamel and dentin. Dent Mater 2004;20: 963-971.
15. Monticelli F, Osorio R, Mazzitelli C, Ferrari M, Toledano M. Limited decalcification/diffusion of self-adhesive cements into dentin. J Dent Res; 2008;87:974-979.
16. Vaz RR, Hipolito VD, D´Alpino PH, Goes MF. Bond strength and interfacial micromorphology of etch-and-rinse and self-adhesive resin cements to dentin. J Prosthodont 2012;21:101-111.
17. Goracci C, Cury AH, Cantoro A, Papacchini F, Tay FR, Ferrari M. Microtensile bond strength and interfacial properties of self-etching and self-adhesive resin cements used to lute composite onlays under different seating forces. J Adhes Dent 2006;8:327-335.
18. Al-Assaf K, Chakmakchi M, Palaghias G, Karanika-Kouma A, Eliades G. Interfacial characteristics of adhesive luting resins and composites with dentine. Dent Mater 2007;23: 829-839.
19. Hikita K, Van Meerbeek B, De Munck J, Ikeda T, Van Landuyt K, Maida T, Lambrechts P, Peumans M. Bonding effectiveness of adhesive luting agents to enamel and dentin. Dent Mater 2007;23:71-80.
20. Viotti RG, Kasaz A, Pena CE, Alexandre RS, Arrais CA, Reis AF. Microtensile bond strength of new self-adhesive luting agents and conventional multistep systems. J Prosthet Dent 2009;102:306-312.
21. Luhrs AK, Guhr S, Gunay H, Geurtsen W. Shear bond strength of self-adhesive resins compared to resin cements etch and rinse to enamel and dentin in vitro. Clin Oral Investig 2010;14:193-199.
22. De Angelis F, Minnoni A, Vitalone LM, Carluccio F, Vadini M, Paolantonio M, D'Arcangelo C. Bond strength evaluation of three self-adhesive luting systems used for cementing composite and porcelain. Oper Dent 2011;36: 626-634.
23. Cerutti A, Flocchini P, Madini L, Mangani F, Putignano A, Docchio F. Effects of bonded composite vs. amalgam on resistance to cuspal deflection for endodontically-treated premolar teeth. Am J Dent 2004;17:295-300.
24. Schwartz RS, Robbins JW. Post placement and restoration of endodontically treated teeth: a literature review. J Endod 2004;30:289-299.
25. Widmalm SE, Ericsson SG. Maximal bite force with centric and eccentric load. J Oral Rehabil 1982;9:445-450.
26. Tortopidis D, Lyons MF, Baxendale RH, Gilmour WH. The variability of bite force measurement between sessions, in different positions within the dental arch. J Oral Rehabil 1998;25:681-686.
27. Ausiello P, Apicella A, Davidson CL. Effect of adhesive layer properties on stress distribution in composite restorations – a 3D finite element analysis. Dent Mater 2002;18: 295-303.
28. Sakaguchi RL, Brust EW, Cross M, DeLong R, Douglas WH. Independent movement of cusps during occlusal loading. Dent Mater 1991;7:186-190.
29. Gwinnett AJ, Matsui A. A study of enamel adhesives. The physical relationship between enamel and adhesives. Arch Oral Biol 1967;12:1615-1619.
30. Nakabayashi N, Kojima M, Masuhara E. The promotion of adhesion by the infiltration of monomers into tooth substrate. J Biomed Mater Res 1982;16:265-273.
31. Gerth HUV, Dammaschke T, Zuchner H, Schafer E. Chemical analyses and bonding reaction of Relyx Unicem and Bifix composites – a comparative study. Dent Mater 2006; 22:934-941.
32. Stona P, Borges GA, Montes MA, Junior LH, Weber JB, Spohr AM. Effect of polyacrylic acid on the interface and bond strength of self-adhesive resin cements to dentin. J Adhes Dent 2013;15:221-227.
33. Duarte S Jr, Botta AC, Meire M, Sadan A. Microtensile bond strengths and scanning electron microscopic evaluation of self-adhesive and self-etch resin cements to intact and etched enamel. J Prosthet Dent 2008;100:203-210.
34. Pavan S, dos Santos PH, Berger S, Bedran-Russo AK. The effect of dentin pretreatment on the microtensile bond strength of self-adhesive resin cements. J Prosthet Dent 2010;104:258-264.
35. Zhang C, Degrange M. Shear bond strengths of self-adhesive luting resins fixing dentine to different restorative materials. J Biomater Sci Polym Ed 2010;21:593-596.
36. Anusavice KJ: Phillips - Dental Materials. Rio de Janeiro, Brazil: Guanabara, 1998:23-68.