ARTÍCULOS ORIGINALES
Oral health in drug addict adolescents and non psychoactive substance users
Pablo C. Gigena1, Lila S. Cornejo1, Alfonsina Lescano- de- Ferrer2
1 Contextual Promotion Research Group. Faculty of Dentistry. National University of Córdoba. Argentina.
2 Comprehensive Dentistry children and adolescents. Faculty of Dentistry. National University of Córdoba, Argentina.
CORRESPONDENCE Dr. Pablo Cristian Gigena Facultad de Odontologia. UNC. La Haya de la Torre s/n. Ciudad Universitaria. (CP 5000) Cordoba, Argentina e-mail: pablo_gigena@hotmail.com
ABSTRACT
The purpose of this study was to compare oral health between adolescents who are recovering drug addicts and adolescents who report not having used psychoactive substances. A retrospective observational Case-Control study was conducted on 60 subjects per group, aged 15 to 25 years, paired according to sex, age and educational vulnerability. Dental and sialochemical examinations were used to determine oral health/disease/care indicators. Psychoactive substance use habits were obtained from clinical records. DMFT index for Case adolescents was 8.58}4.34, doubling the mean value for the Control group, which was 4.33}4.30. CPI was compatible with gingival-periodontal health in 45% of the Control subjects, but only 20% in the Case group. CPI categories 2 and 3 had different distributions according to the study group, with CPI2=33%, CPI3=0% for the case group and CPI2=57%; CPI3=5% for the control group. Mean values for stimulated saliva for Case and Control groups, respectively, were: salivary flow (ml/min) 1.42}1.08; 0.98}0.41, salivary pH 6.96}0.33 6.86}0.27, and buffer capacity expressed as final pH, 6.73}0.29, 6.61}0.28. Wilcoxon's test for independent samples showed significant differences (p<0.05) between Case and Control for the variables White Spot, Non-Cavitated Carious Lesions, Cavitated Carious Lesions, DMFT, Components D and M, Salivary Flow and Buffer Capacity. There was significant association between the D component in DMFT and use of psychoactive substances, both in single drug and polydrug users. Oral component status was worse in recovering drug addicts than in non-users of psychoactive substances.
Key words: Dental Caries Susceptibility; Oral Health; Drug users.
RESUMEN
Salud bucal en adolescentes drogodependientes y en no consumidores de sustancias psicoactivas
El proposito de esta investigacion fue comparar el estado de salud bucodental en adolescentes drogodependientes en recuperacion y los que no refieren consumo de sustancias psicoactivas. Se realizo un estudio observacional tipo Caso y Control, retrospectivo de 60 adolescentes de 15 a 25 anos para cada grupo, apareados segun: sexo, edad y vulnerabilidad educativa. A traves de examen clinico odontologico y sialoquimico se relevaron indicadores de saludenfermedad- atencion del componente bucal. Los habitos de consumo de sustancias psicoactivas se obtuvieron de historias clinicas. El indice CPOD en los adolescentes Casos resulto 8,58}4,34 valor que dobla la media que presenta el grupo Control 4,33}4,30. El Indice IPC presento una situacion compatible con salud gingivo-periodontal en el 45% de los sujetos Control, mientras que solo alcanzo al 20% en el grupo Caso. Las categorias 2 y 3 del IPC mostraron distribucion diferente segun el grupo de estudio siendo IPC2=33%; IPC3=0% y IPC2=57%; IPC3=5%, respectivamente para casos y controles. Los valores medios de los regis tros de saliva estimulada fueron para flujo salival (ml/min) 1,42}1,08; 0,98}0,41, pH de saliva 6,96}0,33 6,86}0,27, y la capacidad amortiguadora o buffer expresada como pH final 6,73}0,29, 6,61}0,28 para el grupo Caso y Control respectivamente. La prueba de Wilcoxon para muestras independientes puso en evidencia diferencias significativas (p<0,05) entre Caso y Control para las variables Mancha Blanca, Caries no Cavitada, Caries Penetrante, CPOD, Componentes C y P, Flujo salival y Capacidad buffer. Se observo asociacion significativa entre el componente C del CPOD y el consumo de sustancias psicoactivas tanto para la modalidad de monoconsumo como para la de policonsumo. La situacion del componente bucal de los sujetos drogodependientes en recuperacion, presenta mayor deterioro, respecto a los no consumidores de sustancias psicoactivas.
Palabras claves: Caries; Salud bucal; Drogadependencia.
INTRODUCTION
The increasing complexity of the modern world has
led to a sharp increase in misuse of psychoactive
substances (PAS), which produce severe physical
and mental effects, leading to individual, family and
social conflict, with serious impact on society. Reliable
research is needed to support intervention
strategies for regional programs for promotion, prevention
and control.
Changes in the interrelationship between human
beings and their world include the use of psychoactive
substances (PAS)1. The analysis and treatment
of PAS addiction disorders are currently tackled
from and comprehensive approach which claims
that "there is no single factor" leading to the process
of addiction, and that different personality subsystems
(environmental-behavioral, biological, cognitive,
affective, spiritual, unconscious and systemic)
may be involved2-4. Drug is considered to be any
substance whose use/abuse can cause psychoneuro-
bio-socio-toxic consequences5. "Drug" is
commonly used to refer to chemical substances
which can cause dependence. The World Health
Organization Expert Committee on Drug Dependence
defines drug as a chemical, whether natural or
synthetic, which, when introduced into a live organism
by any route (inhalation, ingestion, intramuscular,
intravenous), is capable of acting on the
central nervous system, producing physical and/or
psychological alteration, experience of new sensations
or modification of a psychological state, i.e. is
capable of altering the person's behavior.
Adolescent health is a key factor in the economic,
social and political development of Latin American
countries, upon which the success, development
and competencies of the societies to which they
belong depends6.
Adolescence is considered to be a stage which
begins at puberty and lasts until the beginning of
adulthood, when the subject becomes autonomous,
assumes responsibility for his own life, and
achieves his identity. How this process evolves
depends on the characteristics of the context (the
person's particular situation regarding family, gender,
location, social class, education, among others)
and the time in history in which the adolescent
lives7. During the construction of identity, the adolescent
endeavors to differentiate him/herself, and
this may include attitudes ranging from personal
untidiness, lack of interest in cleanliness and neatness,
challenging authority, direct provocation of
adults, poor school performance, dropping out of
school, and sleeping too much or loafing, to behaviors
that place him/her at real risk,8 such as premature
sexual activity, running away from home,
alcohol and/or drug abuse, eating disorders, and
criminal acts, in an attempt to distinguish him/herself
clearly from his/her past world and seek limits
imposed by adults9.
One of the systems affected by exposure to PAS is
the stomatognathic system. It may be affected by
lesions caused by the psychoactive substances
themselves, or related to negligence in attention to
oral hygiene, e.g. diseases such as gingivitis and
extrinsic discoloration10. Substance users have
many clinical odontological alterations such as
xerostomia11, alteration of saliva flow, reduction in
saliva buffer capacity12, erosion, abrasion, atypical
caries and tooth loss13. Many factors can reduce
saliva flow, including physiological situations with
anticholinergic effect, medications14,15, diseases of
the salivary glands or systemic processes affecting
them16. The reduction in saliva flow is explained in
marihuana users as a parasympatholytic effect17. Di
Gugno18 considers that there are three main factors
causing deterioration in PAS users: reduction in
saliva pH and saliva flow, low concentration of
inorganic phosphate, which hinders remineralization,
and high intake of refined carbohydrates.
Also frequent are changes in the pain threshold and
perception of taste, atrophy of salivary glands, erosions
and ulcers of the oral mucosa.
Marihuana users have greater deterioration in the
oral cavity than non-users, with increased risk of
caries and periodontal disease19. Smoking marihuana
is also carcinogenic and associated to dysplastic
changes and precancerous lesions of the oral
mucosa, increasing the incidence of squamous cell
carcinoma, xerostomia, severe gingivitis, ischemic
necrosis of palate, and bruxism20. Marihuana users
are more prone to oral infections, possibly due to
the alteration in oral immunology. Higher DMFT
and bacterial plaque indices have been found in
marihuana users than in non-users17,21.
Drug addicts are careless of their general health and
have behavioral disorders and infections associated
to addiction22, as well as high incidence of caries
and periodontal diesase23.
The aim of this study was to compare the oral health
situation of adolescent and young adults who are
recovering drug addicts to that of adolescents and
young adults who do nor report PAS use.
MATERIALS AND METHODS
A retrospective observational Case-Control study was conducted on adolescents aged 15 to 25 years, of both sexes, paired according to sex, age, and educational vulnerability, following the classification by Gonzalez, 200724,25, who classified the areas in Cordoba Capital district into five levels: cluster 1 – areas with medium high income; cluster 2 – areas with medium income; cluster 3 – areas with low income and clusters 4 and 5, rural areas with few inhabitants per square kilometer. The "Case" group was further characterized by considering their use of psychoactive substances based on clinical records prepared by the institution when subjects enrolled at the Recovery Treatment Program. Pursuant to the Tokyo convention, written informed consent was obtained prior to participation in the study. For adolescents under 18 years old, the informed consent had to be signed by the tutor or guardian.
Inclusion criteria
Adolescents aged 15 to 25 years at the time of the
interview. All subjects included in the Case and
Control groups were social tobacco smokers and
regular alcohol drinkers (at least once a week).
Exclusion criteria
Diagnosis of systemic disease (metabolic, infectiouscontagious,
autoimmune, HIV, transplanted patients,
among others); reporting taking prescribed medication
for over 1 year at the time of the interview; wearing
orthodontic appliances or having had them
removed up to 12 months prior to the interview.
Case group
60 institutionalized drug addict adolescents in
recovery period, aged 15 to 25 years, who voluntarily
joined the NGO "Programa CAMBIO". As a
result of the care system and institutional approach,
participants were subjects who had joined the program
and undergone not more than one month's
treatment to recover from addiction, with a recent
history of exposure to PAS from 2007 to 2010.
International criteria were followed to determine
drug addict status26, and the psychoactive abuse
drugs were classified following the Diagnostic and
Statistical Manual of Mental Disorders of the American
Psychiatric Association –DSM IV TR27.
Control group
60 adolescents who during the interview did not
freely and voluntarily report PAS use, aged 5 to 25
years, of both sexes, who attended the school Colegio
Nacional del Monserrat (formal teaching center)
and the Centro de Orientacion Vocacional
(informal teaching center), both located in Cordoba
city. In order to facilitate the validity of the self
report on PAS use, a prior instance of personal interrelation
was established, at which the subjects felt
free from pressure to express their experience of
possible exposure to PAS. For the Control group,
subjects were paired according to sex, age and educational
vulnerability with regard to the subjects in
the Case group, which was formed first.
Clinical – odontological assessment
A clinical examination28 was conducted in classrooms
assigned by the institutions, using non-conventional
simplified methodology with an exploration
kit consisting of mirror, tweezers, explorer and periodontal
probe, under artificial light (surgical headlight).
Observations were recorded on a card designed
ad-hoc, which in addition to personal data and general
health background, provided space for information
on cariogenic-periodontopathic risk categories. For
hard tissues: the following were recorded: number of
teeth in the mouth, presence of caries (D), discriminating
White Spot incipient caries (WS)29 and noncavitated
caries (nCD); fillings (F); extractions (M).
WHO criteria were followed to diagnose lesions28.
This information as used to calculate the DMFT and
DMFS indices30. Considering that the DMFT index
provides information limited to cavitated carious
lesions, for a more reliable analysis of real conditions
of the health-disease process, the variable "total
caries" was used, which was the sum of all the evolutionary
stages of the disease: WS, nCD and DT (component
D in DMFT). Gingival-periodontal tissue was
assessed using Loee Silness plaque index (PI)31 and
Community Periodontal Index (CPI)28. Saliochemical
assessment
Sialochemical assessment was performed on total
mixed saliva samples, stimulated by chewing a 4cm
x 4cm piece of Parafilm. It measured saliva flow in
ml/min.; pH; and buffer capacity following Ericsson32 and expressed as final pH. A portable manual
pH-meter with temperature probe was used (Adwa).
Statistical analysis
Centralization and dispersion measures were used
to describe the behavior of quantitative variables:
mean } SD and median for discrete variables. Nonparametric
Mann Whitney-U test was used to assess
the significance of the differences in behavior of
the variables in the Case and Control groups33. Pearson's
Chi squared was used to establish differences
between proportions or associations among categorical variables. Contingency 2x2 tables (in
dichotomic variables) were used to establish Odds
Ratios (OR) and their respective confidence intervals
(CI)33. Statistical significance was established
as p = 0.05 for all cases. Data were processed using
Infostat software version 201034.
RESULTS
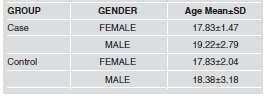
The study was conducted on 120 adolescents, 91% male and 9% female, mean age 19}2 and 18}3 years, distributed in two groups (Case and Control) paired according to sex, age and educational vulnerability. Table 1 shows the distribution according to groups. Characterization of the "Case" group: Subjects in the Case group began using alcohol at age 13 } 0.5 years, and PAS at 16 } 0.3 years, with marihuana being the most frequent substance used first (83%) followed by inhalants (11%) and psychopharmaceuticals without medical prescription (5%). The remaining 1% began directly with cocaine. In the year prior to joining the Institution, (considered recent use), prevalence of psychoactive substances used (statistically significant, Chi squared <0.000) was: marihuana 58%, followed by a combination of other drugs 28% (polydrug use, including marihuana, cocaine and psychopharmaceuticals), cocaine 10%, and psychopharmaceuticals without medical prescription 4%.
Table 1: Distribution of gender and age in Case and Control groups.
Exposure time to PAS (time between first use reported by the subject and date he/she joined the recovery program), varied significantly (Chi squared <0.000). For adolescents and young adults in the Case group it was 1 to 14 years, with a median of 4 years and a mean of 4.4 } 2.6 years. Twenty- two (22) (36.6%) subjects had been addicts for 4 or more years and 38 for less than 4 years (63.3%). Frequency of use in the last year prior to joining the Institution was daily in 70% of the Case group. Clinical-odontological assessment: No alteration was found for pain threshold, taste perception, atrophy of salivary glands, erosions and ulcers of the oral mucosa. Table 2 provides the mean values for tooth status indicators regarding caries experience.
Table 2: Central measurements of DMFT and DMFS indices, and their components.
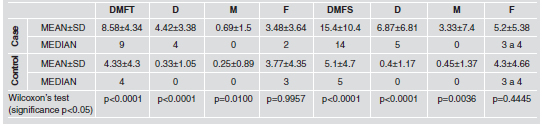
DMFT differed between groups, with the mean and
median values for the Case group being twice as high
as for the Control group, mainly due to the difference
in the D component. Upon considering DMFS, the
values were three times as high for the Case group.
With regard to the D component in DMFT (Fig. 1),
83% of the subjects in the Control group (n: 50) had D
= 0 and 90% of the subjects in the Case group (n: 54)
had D ≥ 1, with OR=45; CI 95% [15.74%; 128.65]. Table 3 shows dental status, with statistically significant
differences between Cases and Controls.
CPI was compatible with gingival-periodontal
health in 45% of the subjects in the Control group
and 20% in the Case group. The distribution of CPI
categories showed differences in frequencies: CPI
2=33%; CPI 3=0% for the Control group and CPI
2=57%; CPI 3=5% for the Case group (Fig. 2).
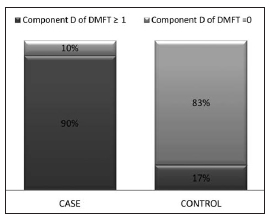
Fig. 1: Distribution of the D component of DMFT in the study
groups.
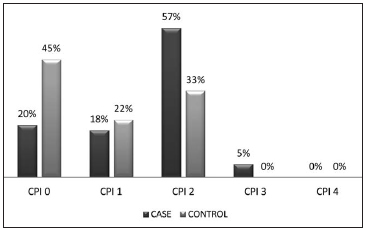
Fig. 2: Distribution of Community Periodontal Index *categories in the study groups.
Table 3: Situation of developmental status of caries in Case and Control groups.
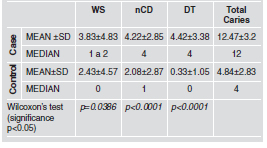
Mean PI values were 0.97}0.83 for the Case group and 0.8}0.52 for the Control group, Wilcoxon test p=0.4910 (significance p<0.05). Although the mean value for both groups reflected low risk (PI <1), it should be noted that BP plaque index indicated at risk (>1) for 33% of the Control group and 47% of the Case group.
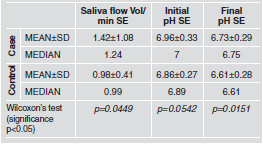
Saliochemical assessment
Table 4 provides the mean values for the variables
recorded in stimulated saliva: saliva flow, pH, and
buffer capacity expressed as final pH32.
Even though the mean value in both groups is compatible
with health, 41.6% of the Case group and
50% of the Control group were assessed as at risk
(salivary flow < 1 ml/m).
Wilcoxon's test for independent samples showed
significant differences (p<0.05) between Case and
Control for the variables Saliva Flow and Buffer
Capacity, with no statistical significance for saliva
pH between groups.
Table 4: Sialochemical variables in Case and
Control groups.
DISCUSSION
Drug addiction is a complex issue in the sphere of
Public Health, because it is associated with a series
of pathologies. This study found more males (91%)
than females in the group of drug addicts undergoing
recovery. Many studies conducted
at different places and
times35-37 agree that addiction to
psychoactive substances is more
frequent in males, except for
use of anxiolytics, sedatives and
tranquilizers, which are more
frequently used by females38.
Considering that the participants
in our study are undergoing
recovery, we should take
into account that several factors
may influence their interest or
decision to join a process to
recover from addiction; thus,
based on our study, we cannot
state that addiction is more frequent
in males.
Because alcohol use is associated as a necessary
antecedent to PAS use39, in our study, all subjects
had used alcohol, at least as weekend users. The
starting age for alcohol use in the Case group was
13 years, significantly lower than the age provided
in the latest national survey on PAS use conducted
by SEDRONAR (Secretariat of Planning for Prevention
of Drug Addiction and Trafficking) in 2010,
which reports 16 years as the starting age for alcohol
use40. Our results are closer to a study conducted
in Cordoba city by Godoy J 200941, where use is
"anticipated" in 11-year-old children.
Studies in other countries assessing the prevalence
of caries in alcoholics report different results42,43.
These are due to factors such as duration and type
of alcohol abuse, oral hygiene, smoking, time since
last visit to the dentist, sugar intake, and abnormal
liver function, among others. Dasanayake 201044
concludes that the group "alcohol and drugs" was
at greater risk of caries (38%) than the "alcohol
only" group, concluding that the risk of caries
among "alcohol only" abusers is significantly lower
than among "alcohol and drug" abusers. That study
suggests that alcohol needs to be taken into account
with regard to caries evolution conditions, based on
the biological model that would explain the association
between alcohol and caries. Microbial oxidation
of ethanol in the saliva of alcohol abusers
would produce acetaldehyde45, which can also alter
cariogenic flora by reducing levels of Streptococcus46.
Warnakulasuriya47 has demonstrated that certain
alcoholic beverages in the United Kingdom
contain high levels of fluoride and people who drink
three cans of beer per day receive the upper limit of
daily fluoride recommended. In Argentina there are
no available data on fluoride content among the
components of alcoholic beverages.
Starting age for PAS use in the Case group was 16
years, marihuana being the preferred first substance,
followed by inhalants and psychopharmaceuticals
without medical prescription. Prevalence
of PAS use in the past year in the Case group was
Marihuana 58.32%, polydrug 28.33%, cocaine 10%
and psychopharmaceuticals without medical prescription
3.33%, with oral intake as the most frequently
used route of administration. Studies
conducted in Spain at hospital detoxification centers
48 found that the variety of routes of administration
has increased over recent years. The
polydrug use detected matches data in the literature
reporting that patients who are addicted to substances
are not usually purists either with regard to
the substances or to the form of taking them, and
they combine different substances and alternate
nasal, oral and more rarely, venous routes 49, in
agreement with our results.
Although the literature reports frequent findings of
variations in pain threshold,50 taste perception, atrophy
of salivary glands, erosions and ulcers of the
oral mucosa51-53, our study found none of those
alterations. Incidence of lesions in the gingivalperiodontal
tissues increases with modality, duration,
frequency and intensity of PAS use, together
with lack of oral hygiene54,55, as reflected by the fact
that 47% of the Case group had at risk plaque index
(PI> 1), in contrast to 33.33% of the Control group,
although mean PI for both groups did not indicate
risk. This may be due to the fact that the patients
are institutionalized, and have therefore recovered
more regular hygiene and diet habits. The risk
shown by plaque index associated to gingival alteration
detected in almost 50% of the Case group, it
matches reports in the literature about the frequency
of chronic gingivitis in patients who are
addicts56. According to one study57 the type of
brush, and frequency and way of brushing differ
significantly between drug users and controls without
exposure to PAS. This variable was not considered
in our study.
With regard to periodontal status, in our study, CPI
was compatible with gingival-periodontal health in
45% of the Control group and 20% of the Case
group, with different distributions: CPI2=33%;
CPI3=0% in the Control group and CPI2=57%;
CPI3=5% in the Case group. Considering that grade
2 reflects the presence of dental calculus and not
necessarily the evolution of gingival-periodontal
disease, there is lack of evidence to suggest a link
between PAS use (primarily marihuana) and periodontal
disease in the adolescent population in the
Case group exposed to PAS, in agreement with
studies conducted in Chile58.
Persons who are still cannabis smokers can be classified
as ‘'long-term users, and thus at amotivational
risk" as described in Schwartz syndrome59,
characterized by lack of concern for personal
hygiene and appearance, suggesting self-abandonment.
In our study we may infer that the periodontal
effects of short-term exposure to cannabis
(participant ages in this study were 15 to 25 years)
may differ from the more serious effects of long
term exposure to it in an older population.
With regard to dental disease, specifically caries
prevalence, in the drug addict group, our research
found similar results to studies conducted in
Spain60,61, Italy62, Denmark63, United States64, France65
and Australia23.
It has been reported that caries experience in marihuana
addicts is high17,19,21. In our Case group,
DMFT showed a mean value of 8.58 } 4.34 teeth
with caries history, notably lower than values
reported in other papers, such as DMFT = 18.3 in
Aarhus, Denmark63, 16.9 in Holland among addicts
aged 20-40 years50, 12.9 in Mercato San Severino
(Salerno), Italy, for addicts aged 18 to 34 years62,
12.8 in Barcelona, Spain in addicts aged 17 to 40
years60, 13.03 in another group in Spain61, among
various other studies conducted in Australia23, United
States64 and France65. Nevertheless, upon considering
"total caries" in the Case group, which also
includes cavitated caries, incipient lesions (WS)
and non-cavitated caries (nCD), the mean value is
closer to the values mentioned above.
A paper by Reece 200766 reports a cross-sectional
study of 280 subjects aged 19 to 45 years, divided
into a group of drug addicts and another group of
non-drug addicts, showing that the addicts had a
higher percentage of decayed and missing teeth
than the non addicts. The pathology developed at
an earlier age in addicts. Among subjects younger
than 35 years old, 56.8% of addicts had the pathology
compared to 5.4 % of the non-addicts. This
agrees with our findings, in which the Case group
had greater number and severity of caries (reflected
by the higher number of caries with pulp complication)
than the Control group.
Szymaniak 199067 studied tooth status in 30 drug
addicts aged 21-34 years (duration of addiction 3 to
16 years) and compared the results to those from a
similar group of subjects of the same age who were
not drug addicts. The study found that drug addicts
had twice as many decayed and missing teeth and four
times fewer fillings than the controls. It concludes that
drug addiction activates the carious process and the
tendency to mutilation of the stomatognathic system.
Another study on addicts (mainly intravenous route
users) in India57, aged 18 to 48 years, found mean
DMFT 4.84 for addicts and 3.73 for controls, which
are lower than the values found in our study, possibly
related to the type of use.
Our study found no significant difference in the F
component between groups, so it is assumed that
there has been adequate dental care availability,
possibly before Case group subjects became addicted,
since there is a marked difference in the D components
and severity of lesions between groups.
For the M component, the Case group had higher
frequency, which may be evidence of lack of timely
dental care for restoration, conversely to what
happens with the F component.
Drug abuse may reduce pain associated to dental
caries, thus by the time PAS users are examined
they are late in the process of the disease, in agreement
with Charnock 200454.
In our study, the mean value for decayed teeth with
cavitated carious lesions (D) and missing teeth (M)
were higher in the Case group (5.11) than in the
Control group (0.58), reflecting access to dental
care and low self esteem during the addiction
process in the Case group, in agreement with studies
conducted in Spain60.
Addiction to PAS may thus be considered to act at
least as a factor which, from the socio-cultural to
the individual psychological, has negative influence
on timely visits to the dentist and thus, on receiving
early care for the pathology.
In our study, the Cochran-Mantel-Haenszel test
shows the variable Gender influenced behavior of
presence of caries in both groups.
Sialochemical assessment showed that saliva flow
differed significantly between Case (1.42 ml/min)
and Control (0.98 ml/min) groups. The value for
drug addicts was similar to those found in other
studies in Brazil68 in similar conditions on a population
exposed to PAS under study, who were found
to have mean values of 1.13 ml/min. It should be
noted that in this population in Brazil, 64% had saliva
flow >1, whereas in our study, only 41.1% did.
Although various studies mention dry mouth as an
effect of drugs18,69,70, it was not observed in our
study. Salivary glands might have normalized their
functioning after PAS use stopped, restoring the
salivary flow. Moreover, due to regulations at the
institution "Programa Cambio", it was not always
possible to know what type of medication the
patients were using in order to make a more specific
analysis of the effects of each drug prescribed by
the physician at the institution. It is worth highlighting
that because the institution is coordinated by
psychologists, its therapy minimizes the psychiatric
medication administered to institutionalized
patients, in contrast to other therapeutic communities
where there is a tendency to substitution therapy
with regard to psychiatric medication, which
may substantially modify saliva flow rates.
The pH was similar in both groups (Case group:
6.96; Control: 6.86), with no statistically significant
difference between groups, in a range compatible
with health, in agreement with other studies on
drug addicts in Spain,60 where pH was 6.80.
Buffer capacity in both groups was compatible with
healthy values (Δ pH 0.23 for the Case group and
0.25 for the Control group) in contrast to studies in
Brazil12,68 which found alterations in buffer capacity.
Although according to a study by Kumar in 2006
on 220 institutionalized psychiatric patients71,
caries index increases with age, our study did not
analyze the age factor as predictive, as being a PAS
addict was more important.
Some authors50,62,72 have suggested that in this type
of patients the degree of dental pathology is directly
related to poor oral hygiene and the years of
actively using psychoactive substances. The literature
in general reports data on oral use of marihuana
and cocaine in relation to lesions found in the
oral component19,21.
In our study, adolescents in the Case group reported
that they use marihuana, usually smoked, together
with alcohol and tobacco, which makes it impossible
to discern whether the oral-dental component status in
the Case group can be attributed exclusively to PAS.
There is not enough evidence of association
between PAS addiction and caries. In our study, the
conditions of oral deterioration in the Case group
compared to the Control group cannot be attributed
exclusively to exposure to PAS. PAS use is a complex
phenomenon in which the psychological-emotional
factor has an impact on personal care,
including hygienic-dietary habits, generating an
unfavorable context which makes it difficult to
identify which effects on the oral component are
attributable to PAS use. Further studies are needed
on other therapeutic communities for drug addicts,
and which look in greater depth at other socio-cultural
aspects not considered in this study, in order
to identify the factors that have the greatest incidence
on the development of caries in drug addicts.
There is a wide gap between the oral-dental health
status of drug addict adolescents undergoing recovery
and adolescents who do not report use of psychoactive
substances. Worldwide, there are few
reliable epidemiological data on dental caries in
alcohol and drug users, even though both alcohol
and drug abuse, whether individually or combined,
have harmful effects on health. Further research is
needed to understand the true nature of the effect of
these damaging exposures on various components
of caries experience.
ACKNOLWEDGMENTS
We thank the Secretariat of Science and Technology of the National University of Cordoba (SECYT) for the grant awarded, and the Faculty of Dentistry for their financial support for the publication of results. We are deeply grateful to Irma Moncunill, Elena Hilas, Maria Fernanda Lucero, Ariel Herrera, Fabiana Carletto Korber, Natalia Aguero, and Mario Llanes, all members of the Contextual Promotion Research Group (PROCON), who cooperated with the survey and processing of data. We also wish to thank Mabel Brunotto for assistance in the statistics analysis.
1. D´agnone O. Capitulo 1: El Impacto de las Revoluciones Industriales y las Nuevas Tecnologias. En Nuevos desarrollos en prevencion y terapeutica de las adicciones. Argentina Editorial Salerno.1999:1-25.
2. Maturana H. Biologia de la cognicion y epistemologia. Temuco. Chile. Editorial Universidad de la Frontera. 1990:15-28.
3. Guajardo H, Bagladi V, Kushner D. Modelo integrativo de evaluacion para trastornos adictivos en un sistema terapeutico comunitario. Revista Eradicciones 2001;4:14-26.
4. Guajardo H, kushner D. La introvisacion a traves de la autobiografia: una tecnica para el reprocesamiento de la funcion de significacion del self en el paciente adicto. Revista Eradicciones 2001;7:49-58.
5. Kalina E. ADICCIONES. Aportes para la clinica y la terapeutica. Argentina, Editorial Piados. 2000:13-18.
6. Organizacion Panamericana de la Salud Oficina Sanitaria Panamericana, Oficina Regional de la Organizacion Mundial de la Salud. Proyecto de desarrollo y salud integral de adolescentes y jovenes en America Latina y el Caribe (1997- 2000). Fundacion W.K. Kellogg Division de Promocion y Proteccion de la Salud Programa de Salud Familia y Poblacion Salud del Adolescente. 1998. URL: http://http://www.bvsde.paho.org/bvsacd/cd59/saludintegral.pdf
7. Urresti M. Cambio de escenarios sociales, experiencia juvenil urbana y escuela. En: Tenti Fanfani, E. (comp.) Una escuela para los adolescentes. UNICEF/Losada. Buenos Aires, 2000: 4-7. URL: http://ei.org.ar/edumedia/pdfs/T01_ Docu1_Cambiodeescenariossociales_Urresti.pdf
8. Gomez de Giraudo MT. Adolescencia y prevencion: conducta de riesgo y resiliencia. URL: http://www.salvador.edu.ar/ua1-9pub01-4-03.htm.
9. Perez Gomez A. La cultura escolar en la sociedad neoliberal. Ed. Morata. Madrid. Espana. 1998:102-116.
10. Bullock K. Dental care of patients with substance abuse. Dent Clin North Am 1999;43:513-526.
11. Hubbard JR, Franco SE, Onaivi ES. Marijuana: medical implications. Am Fam Physician 1999;60:2583-2588.
12. Pedreira RHS, Remencius L, Navarro MFL, Tomita NE. Condicoes de saude bucal de drogaditos em recuperacao. Odontol Univ Sao Paulo 1999;13:395-399.
13. Sandoval C. Lesiones clinicas bucales en pacientes farmacodependientes / Clinical oral lesions in drug addict patients. Rev estomatologia Hered 1992;2:22-26.
14. Guggenheimer J, Moore PA. Xerostomia: etiology, recognition and treatment. J Am Dent Assoc 2003;134:61-69.
15. Smith RG, Burtner AP. Oral side-effects of the most frequently prescribed drugs. Spec Care Dentist. 1994; 14:96-102.
16. Rodriguez-Landa JF, Contreras CM. Algunos datos recientes sobre la fisiopatologia de los trastornos por ansiedad. Rev Biomed 1998;9:181-91.
17. Darling MR, Arendorf TM. Review of the effects of cannabis smoking on oral health. Int Dent J 1992;42:19-22.
18. Di Gugno F, Perec CJ, Tocci AA. Salivary secretion and dental caries experience in drug addicts. Arch Oral Biol 1981;26:363-367.
19. Cho CM, Hirsch R; Johnstone, S. General and oral health implications of cannabis use. Aust Dent J 2005;50:(2):70-74.
20. Fazzi M, Vescovi P, Savi A, Manfredi M, Peracchia M. The effects of drugs on the oral cavity. Minerva Stomatol 1999; 48:485-492.
21. Darling MR, Arendorf TM. Effects of cannabis smoking on oral soft tissues. Community Dent Oral Epidemiol. 1999; 21:78-81.
22. Titsas A, Ferguson MM. Impact of opioid use on dentistry. Aust Dent J 2002;47:94-98.
23. Carter EF. Dental implications of narcotic addiction. Aust Dent J 1978; 23:308-310.
24. Alvarez M, Gonzalez L, Harrington M, Maccagno A, Pelaez E, Ribotta B. Vulnerabilidad socio-educativa. Un analisis transversal de la realidad de Cordoba. Argentina. Comunic-arte Editorial. 2004.
25. Gonzalez L. Vulnerabilidad Educativa en el Gran Cordoba. Argentina. Astrolabio no 4. 2007.
26. Secretaria de Programacion para la Prevencion de la Drogadiccion y la Lucha contra el Narcotrafico. (SEDRONAR). Observatorio Argentino de sustancias. Consumo de sustancias psicoactivas en estudiantes universitarios del interior del pais. Republica Argentina. (2006) URL: http://www.observatorio.gov.ar/ investigaciones/Consumo_de_sustancias_ psicoactivas_en_Estudiantes_Universitarios_en_el_interior_del_Pais.pdf
27. DSMIV. Manual diagnostico y estadistico de los trastornos mentales. Barcelona. 1995. Masson S.A.
28. WHO. "Oral Health Surveys, Basic Methods" 2nd ed. World Health Organization, Geneva. 1997.
29. Bordoni N, Dono R, Squassi A. PRECONC: Curso 1: Odontologia preventiva. Modulo 1: Diagnostico de enfermedades por placa bacteriana. Vol.1. Buenos Aires: Paltex. 1999.
30. Klein H, Palmer CE, Kunutson JW. Studies on dental caries. Dental status and Dental needs of elementary school children. Public Health Rep 1938;53:751-765.
31. Loee H, Silness C. Gingival index, the plaque index and the retention index system. J Periodontol 1967;38:610-618.
32. Ericsson Y. Clinical investigations of the salivary buffering action. Acta Odontol Scant 1959;17:131-165.
33. Pepe Sullivan, M. The Statistical Evaluation of Medical Tests for Classification and Prediction. Oxford University Press. Oxford UK. 2003.
34. Di Rienzo JA, Casanoves F, Balzarini MG, Gonzalez L, Tablada M, Robledo CW. Grupo InfoStat, FCA, Universidad Nacional de Cordoba, Argentina. 2010.
35. Gutierrez del Rio C, Casanueva-Gutierrez M, Fuente-Garcia B, Gallo-Alvaro C, Garcia-Alcalde Fernandez ML, Moris-Tassa J. Unidad de desintoxicacion hospitalaria: cuatro anos de experiencia. Tratamiento e infecciones. An Med Interna 1998;15:528- 530.
36. Grupo de Trabajo para el Estudio de Infecciones en Drogadictos. Estudio multicentrico de las complicaciones infecciosas en adictos a sustancias por via parenteral en Espana: analisis final de 17.592 casos (1977-1991). Enferm Infecc Microbiol Clin 1995;13:532-539.
37. Jimenez-Fabrega X, Carballo-Almeida A, Batalla-MartInez C, ComIn-Bertran E, Cuenca-Oliva AM, Ezpeleta-Garcia A, Lopez-Gonzalo E, Parellada-Esquius N. Prevalencia de la infeccion por los virus de la hepatitis B, C e inmunodeficiencia humana en usuarios de sustancias. Aten Primaria. 1999;24:368-371.
38. Secretaria de Programacion para la Prevencion de la Drogadiccion y la Lucha contra el Narcotrafico. (SEDRONAR). Observatorio Argentino de sustancias. Informe Final: "El Uso Indebido de Sustancias y la Consulta de Emergencia. Cuarto Estudio Nacional: 2009" boletin oficial No 31.843. URL: http://www.boletinoficial.gov.ar/DisplayPdf.aspx?s=04&f=20100215
39. Salas, C. La actuacion preventiva sobre el consumo de alcohol y drogas en el ambito laboral. "MC salud laboral" 2013; 1:6-9.
40. Secretaria de Programacion para la Prevencion de la Drogadiccion y la Lucha contra el Narcotrafico. (SEDRONAR). Observatorio Argentino de sustancias. (2010) Estudio nacional en poblacion de 12 a 65 anos, sobre consumo de sustancias psicoactivas. URL: http://www.observatorio.gov.ar/investigaciones/Estudio_Nacional_sobre_consumo_ en_poblacion_general-Argentina2010.pdf
41. Godoy JC. Los jovenes y el consumo de alcohol: estudios neuropsicologicos. 2009, Cordoba. Argentina. URL: http://www.secyt.unc.edu.ar/Nuevo/portada_contenido.php?idNota=234
42. Hornecker E, Muuss T, Ehrenreich H, Mausberg RF. A pilot study on the oral conditions of severely alcohol addicted persons. J Contemp Dent Pract 2003; 4:51-59.
43. Novacek T , Plachetzky U , Potzi R , Lentner S , Slavicek R , Gangl A , Ferenci P . Dental and periodontal disease in patients with cirrhosis – role of etiology of liver disease. J Hepatol 1995;22:576-582.
44. Dasanayake A, Warnakulasuriya S, Harris C, Cooper D, Peters T, Gelbier S, Tooth Decay in Alcohol Abusers Compared to Alcohol and Drug Abusers. Int J Dent 2010; 2010: 786503.
45. Homann N, Tillonen J, Meurman HJ, Rintamaki H, Lindqvist C, Rautio M, Jousimies-Somer H, Salaspuro M. Increased salivary acetaldehyde levels in heavy drinkers and smokers: a microbiological approach to oral cavity cancer. Carcinogenesis 2000;21:663-668.
46. Kurkivuori J, Salaspuro V, Kaihovaara P, Kari K, Rautemaa R, Gronroos L, Meurman JH, Salaspuro M. Acetaldehyde production from ethanol by oral streptococci, Oral Oncol. 2007;43:181-186.
47. Warnakulasuriya, Harris C, Gelbier S, Keating J, Peters T. "Fluoride content of alcoholic beverages" Clin Chim Acta 2002;320:1-4.
48. Gutierrez del Rio C, Casanueva-Gutierrez M, Nuno-Mateo J, Fernandez-Bustamante J, Moris de la Tassa J. Unidad de desintoxicacion hospitalaria: cuatro anos de experiencia. Factores ambientales. An Med Interna 1998;15:584-587.
49. Cherubin CE, Sapira JD. The medical complications of drug addiction and the medical assessment of intravenous drug user: 25 years later. Ann Intern Med 1993;119:1017- 1028.
50. Molendijk B, Ter-Host G, Kasbergen M, Truin GJ, Mulder J. Dental health in Dutch drug addicts. Community Dent Oral Epidemiol 1996; 24:117-119.
51. Brezina J. Patologia odontoestomatologica en un establecimiento correccional. Bol Asoc Argent Odontol Ninos 1996;25:9-14.
52. Stolz A, Cossetin E. Relacao do uso de sustancias psicotropicas e lesoes orais / Relationship between psicotropics drugs use and oral lesions. Rev ABO nac 2002;9:356-359.
53. Pilinova A, Krutina M, Salandova M, Pilin A. Oral health status of drug addicts in the Czech Republic. J Forensic Odontostomatol 2003;21:36-39.
54. Charnock S, Owen S, Brookes V, Williams M.A community based programme to improve Access to dental services for drug users. Br Den J 2004;196:7.
55. Rooban T, Rao A, E Josue, Ranganathan K. Oral lesions of 500 habitual psychoactive substance users in Chennai, India. Indian J Dent Res 2009;20:41-46.
56. Solorzano-Navarro E, Davila-Barrios L, Quinonez B, Obediente- Sosa E. Efectos clinicos e histologicos de la cocaina sobre el periodonto de proteccion / Clinical and histologic effects of cocaine on protecting periodontium. Rev Asoc Odontol Argent 2003;91:222-225.
57. Rooban T, Rao A, E Josue, Ranganathan K. Dental and oral health status in drug abusers in Chennai, India: A cross-sectional study. Journal of Oral and Maxillo Facial Pathology. 2008;12:16-21.
58. Lopez R, Baelum V. Cannabis use and destructive periodontal diseases among adolescents. J Clin Periodontol 2009;36:185-189.
59. Schwartz RH. Marijuana: an overview. Pediatric Clin North Am 1987;34:305-317.
60. Jimenez-Polanco MP, Astudillo-Jimenez O, Mata-Brotons V, Jorge-Ferre J, Correia d' Oliveira NG. Depresion y drogodependencia: efectos sobre la salud dental. Av Odontoestomatol. 2011;27: 1.
61. Rodriguez Vazquez C, Cabello ML, Quijada E, Rioboo R. Evaluacion de la salud oral en una poblacion de drogodependientes. Av Odontoestomatol 2002;18:153-60.
62. Angelillo IF, Grasso GM, Sagliocco G, Villari P, D´Errico MM. Dental health in a group of drug addicts in Italy. Community Dent Oral Epidemol 1991;19:36-37.
63. Scheutz F. Dental health in a group of drug addicts attending an addiction-clinic. Community Dent Oral Epidemiol 1984;12:23-8.
64. Bernardini AM, Camus JP. Etat buccodentaire chez le toxicomanie. Rev Odontoestomatol 1983;12:169-173.
65. Rosenstein DI, Stewart A. Dental care for patients receiving methadone. J Am Dent Assoc 1974;89:356-359.
66. Reece AS. Dentition of addiction in Queensland: poor dental status and major contributing drugs. Aust Dent J 2007; 52:144-149.
67. Szymaniak, Waszkiel D, Dymkowska W. The condition of teeth and the need for teeth treatment in drug addicts. Czas Stomatol 1990;43:134-139.
68. Ribeiro EDP, Oliveira JA de, Zambolin AP, Lauris JRP, Tomita NE. Abordagem integrada da saude bucal de drogadependentes em processo de recuperacao. Pesqui Odontol Bras 2002;16:239-245.
69. Friedlander AH, Friedlander IK, Gallas M, Velasco E. Latelife depression: its oral health significance. Int Dent J 2003; 53:41-50.
70. Miers DR, Smith DP. Guidelines for treatment of recovering chemically dependent patients. J Am Coll Dent 1989; 56:4-8.
71. Kumar M, Chandu GN, Shafiulla MD. Oral health status and treatment needs in institutionalized psychiatric patients: one year descriptive cross sectional study. Indian J dent Res 2006;17:171-177.
72. Silvestre FJ, Bagan JV, Del Olmo JA, Jimeno V. Oral status of drug addicted patients. Study of 66 cases. Actual Odontostomatol 1990; 44:299-306.