
Fig. 1: Multiplanar Reconstruction: right side at maximum intercuspation position.
ARTÍCULOS ORIGINALES
Perception of professionals in the assessment of coronoid hyperplasia by computed tomography
Vanda Domingos1, Adalsa Hernandez2, Cláudio F. Freitas1, Marlene Fenyo-Pereira1, Ricardo Raitz3
1 Department of Stomatology, School of Dentistry, University of São Paulo, Brazil
2 Félix Boada Imaging Clinic, Caracas, Venezuela
3 São Leopoldo Mandic School of Dentistry and Research Center, Campinas, Brazil
CORRESPONDENCE Professor Dr Ricardo Raitz Rua Heitor Penteado, 1832, 101A, cep: 05438-300, Sao Paulo, SP, Brazil email:ricardoraitz@ig.com.br
ABSTRACT
Coronoid Hyperplasia (CH) is a non-neoplastic and relatively rare enlargement of the coronoid process that may limit mandibular movement as a consequence of the close association between the hyperplastic coronoid process and the anterior region of the zygomatic bone. Computed tomography (CT) is extremely useful for the observation of this association and plays an important role in diagnosing and planning surgical treatment. Once the CT scan is performed, the data can be viewed in many different arrangements, including multiplanar (MPR) and 3D rendering, although the resolution of the latter may not be as good as that of the former. Our aim is to analyze the importance of and preference for multiplanar and 3D reconstruction images for diagnosing and interpreting Coronoid Hyperplasia (CH), by comparing the opinions of oral surgeons and oral radiologists who analyzed both temporomandibular joints (TMJ) in 20 patients. Three images of each TMJ comprised the set of scans (MPR, 3D reconstructions with maximum intercuspation and 3D reconstructions with maximum mouth opening). After each analysis, the members of the two groups answered a questionnaire about the usefulness of each examination and classified the association between the head of mandible and mandibular fossa. Hypomotility was present in 55.2%. Both groups stated that both MPR and 3D reconstructions, particularly the latter, were fundamental for diagnosing CH and that they would request them in order to interpret CH correctly. The examiners were found to differ significantly regarding their opinion of MPR; only radiologists considered MPR to be less elucidative for the diagnosis of CH.
Key words: Temporomandibular joint disorders; Computed tomography.
RESUMO
Percepção de profissionais na avaliação da hiperplasia coronóide pela tomografia computadorizada
A Hiperplasia Coronoide (HC) e um aumento nao-neoplasico e relativamente raro do processo coronoide que pode limitar o movimento mandibular, como consequencia da intima relacao entre o processo coronoide hiperplasico e a regiao anterior do osso zigomatico. A tomografia computadorizada (TC) e extremamente util para a observacao dessa relacao, desempenhando assim um papel importante no diagnostico e planejamento do tratamento cirurgico. Uma vez que a TC e realizada, os dados podem ser vistos em muitos arranjos diferentes, incluindo o multiplanar (MPR) e a reconstrucao em 3D, no entanto, a resolucao desta ultima pode nao ser tao boa quanto a primeira. Nosso objetivo e analisar a importancia e a preferencia por reconstrucoes de imagens multiplanares (MPR) e 3D para diagnosticar e interpretar a Hiperplasia Coronoide (HC), comparando cirurgioes buco-maxilo-faciais com radiologistas orais. Ambas as articulacoes temporomandibulares (ATM) de 20 pacientes foram analisadas pelos 2 grupos. Tres imagens de cada ATM compreenderam o conjunto de exames (MPR, reconstrucoes 3D em maxima intercuspidacao e reconstrucoes 3D com abertura maxima da boca). Apos cada analise, os grupos responderam a um questionario sobre a utilidade de cada exame e classificou a relacao entre a cabeca da mandibula e da fossa mandibular. A Hipomobilidade esteve presente em 55,2%. Ambos os grupos afirmaram que tanto MPR e as reconstrucoes em 3D, especialmente a ultima, foram fundamentais para diagnosticar CH e as requisitariam para interpretar a HC corretamente. Foi encontrada uma diferenca significativa entre os examinadores sobre a MPR; apenas o grupo de radiologistas considerou que este exame nao e tao elucidativo para o diagnostico da CH.
Key words: Articulacao temporo-mandibular; Tomografia computadorizada.
INTRODUCTION
Temporomandibular joint (TMJ) dysfunction is a
common disease that causes many people to seek
treatment at dental care centers to restore proper,
pain-free TMJ movement. However, it may be mistakenly
diagnosed as a different pathology. Some
patients in fact present Coronoid Hyperplasia (CH),
which is a non-neoplastic, relatively rare enlarge-
ment of the coronoid process1 that may limit
mandibular movement as a result of the close association
between the hyperplastic coronoid process
and the anterior region of the zygomatic bone2,3.
CH may be more common than is believed, but
because it is mostly painless, patients only seek
treatment if the inability to open the mouth is severe
enough to compromise mastication4-7. However, the
disease gradually becomes more severe during the
second decade of life. It can be unilateral (with only
one hyperplastic coronoid process) or bilateral.
In radiographs, a hyperplastic coronoid process is
generally large and long, projecting into the infratemporal
fossa, with normal trabecular bone8. Radiographs
are thus inappropriate to diagnose it9.
Computed tomography (CT), in contrast, is extremely
useful for the observation of the association
between the hyperplastic coronoid process and the
zygomatic bone4,10,11, and thus plays an important role
in diagnosing and planning surgical treatment. Treatment
consists of surgical correction of CH. Coronoidectomy
is the method of choice, followed by
intense physiotherapy 12,13.
Once the CT scan is performed, the data can be
viewed in many different arrangements, including
multiplanar (MPR) and 3D rendering, although the
resolution of the latter may be lower than that of the
former. The literature does not discuss which of
these arrangements dental specialists consider most
useful, or whether they would always use both of
them to make a safe, correct diagnosis of CH. The
purpose of this study was to analyze the importance
of and the preference for MPR and 3D reconstruction
images in diagnosing CH, by comparing the
opinions of oral surgeons and radiologists.
MATERIAL AND METHODS
Sample
Archival images of spiral CT scans of 152 patients
with signs and symptoms of TMJ dysfunction were
analyzed. Said patients had been referred to the
Dentomaxillofacial Imaging Department of a Dentistry
and Medical Clinic, for CT scan of the TMJ,
requested by specialized professionals (orthodontists
and oral surgeons) with diagnostic purposes.
This was a multicenter study which was approved
by the Research Ethics Committee of the School of
Dentistry of the University involved.
Among the 152 patients, 20 cases diagnosed with CH
were selected. The diagnosis was initially made by an
independent oral surgeon specialized in oral maxillofacial
radiology, who made the diagnosis based on
clinical (limitation of mouth opening) and imaging
information. The diagnosis of CH was made when the
coronoid process in patients with closed mouth
exceeded the zygomatic process and in multiplanar
images (MPR) whenever it exceeded the height of the
condyle. All diagnoses were revised and confirmed by
3 different independent oral maxillofacial radiologists,
who did not take part in the experiment. Age, sex and
race were not considered when selecting the sample.
The selected images were obtained through multiplanar
(Fig. 1) and 3D reconstruction (Figs. 2 and 3).
Fig. 1: Multiplanar Reconstruction: right side at maximum
intercuspation position.
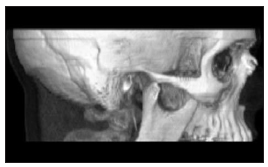
Fig. 2: 3D Reconstruction: right side at maximum mouth opening.

Fig. 3: 3D Reconstruction: right side at maximum intercuspation position.
CT acquisition
The images were acquired by a fourth generation
Toshiba Auklet™ CT scanner (Tustin, CA, USA)
with a matrix size of 512 X 512. Technical parameters
were as follows: 120 kVp, 250 mA, 2 mm slice
width, 1 mm pitch factor.
Eighty-eight axial 2 mm slices were obtained with
1 mm reconstruction intervals and a pixel size of
0.4688 mm. The images were acquired as follows:
a) maximum intercuspation position; and b) maximum
mouth opening (patients were instructed to open
the mouth to their limit and immediately bite a mouth
block - 40x30x20mm or 30x25x18mm Maquira,
Maringa, Brazil - throughout the acquisition).
The acquired images were sent to an Alatoviewa
workstation (Tustin, CA, USA), where volume reconstruction
was carried out. Only multiplanar and 3D
reconstructions were used in this study. The images
were converted from DICOM to TIFF format, transferred
to a conventional computer and stored on CD.
Image analysis
Image analysis was performed by two groups of
examiners with at least twenty years' experience in
their specialties. One group included five oral maxillofacial
radiologists and the other group included
five oral and maxillofacial surgeons, all of who
were renowned professors and PhDs in their areas.
Both groups received 20 sets of scans (20 cases),
composed of multiplanar reconstructions (MPR at
maximum intercuspation position, right side and
left side) and 3D reconstructions (right side and left
side at maximum intercuspation and maximum
mouth opening). A total of three images of 40 TMJs
were analyzed (Figs. 1, 2 and 3).
After analyzing the images of each of the 20 cases,
each examiner answered a questionnaire about the
comparison between MPR and 3D reconstructions.
Each examiner thus answered 20 questionnaires.
The questionnaire was composed of the following
questions:
1) Do you think that 3D reconstructions were more
elucidative than MPR to correctly diagnose and
interpret these images of CH? Score 1 – Yes;
Score 2 – No.
2) Do you think that MPR was more elucidative
than 3D reconstructions to correctly diagnose
and interpret these images of CH? Score 1 – Yes;
Score 2 – No.
3) How important are these imaging methods, analyzed
separately or simultaneously, to help establish
a correct diagnosis and interpretation of CH?
Score 1 – Very important; Score 2 – Not so
important; Score 3 – Not important.
4) Would you request one or both of these imaging
tests to analyze CH? Score 1 – Yes; Score 2 – No.
5) By interpreting 3D reconstructions of maximum
mouth opening, it was possible to conclude that
the patient had: Score 1 – Hypermobility; Score
2 – Hypomobility; Score 3– Normal jaw movement;
Score 4 – It was not possible to establish a
diagnosis.
In relation to the question 5, the following classification was explained for each examiner before evaluation: Normal: the uppermost portion of the head of mandible is below the bottommost portion of the articular tubercle of temporal bone. Hypermobility: the uppermost portion of the condylar process is beyond the bottommost portion of the articular tubercle of temporal bone. Hypomobility: the uppermost portion of the condylar process does not reach the bottommost portion of the articular tubercle of temporal bone. The data obtained were tabulated and submitted to statistical analysis by the Analysis of Means (ANOM), Kruskal-Wallis test and Fisher's exact test.
RESULTS
The answers to questions 1 and 2 were transformed
into dichotomous variables: "yes" represented
Score 1 (examiner agrees) and "no" represented
Score 2 (examiner disagrees). Thus, the tables that
represent questions 1 and 2 show the percentage of
affirmative answers.
For the analysis of question 3, means or medians of
the scores were used. The answer to question 4 was
also transformed into a dichotomous variable: "yes"
represented Score 1 (examiner would request imaging
tests) and "no" represented Score 2 (examiner
would not request imaging tests). The tables that represent question 4 also show the percentage of
affirmative answers.
Tables 1 and 2 show the proportion of affirmative
answers to questions 1 and 2 and 4, as well as the mean
score for the answers to question 3 for both groups.
For the analysis of question 5, a graph that expresses
in percentage hypermobility, hypomobility or normal
jaw movement (relation between the head of mandible
and mandibular fossa) was used and showed that
55.2% of the cases had hypomobility, 24.1% had normal
mobility and 20.7% had hypermobility (Fig.4).
The Kruskal-Wallis test was used to compare the
scores for both groups (oral radiologists and oral surgeons),
revealing no significant difference between
them either for the right side (p=0.934) or the left side
(p=0.064). Diagnosis of mandibular movement was
based on the relation between the head of mandible
and the mandibular fossa, analyzed by both groups
upon observation of 3D reconstructions.
The answers to each question provided by the five
examiners in each group were compared by means
of statistical analysis. ANOM was used to calculate
a general average for the five examiners and an
interval that indicated which examiners had similar
opinions and which had different ones. ANOM
compares group means to the overall mean, providing
a graphic procedure for comparing a collection
of means, rates or proportions to determine whether
any of them differ significantly from the overall mean, rate or proportion. ANOM is a type of multiple
comparison procedure.
Table 1: Percentages of affirmative answers and scores for oral surgeons.
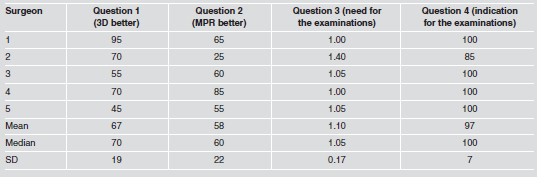
Table 2: Percentages of affirmative answers and scores for oral radiologists.


Fig. 4: Percentage of the jaw movement (relation between the head of mandible and mandibular fossa).
The groups were compared (radiologists and oral and maxillofacial surgeons). Since questions 1 and 2 and 4 dealt with proportions, the proportion test was used to compare them. No significant difference (p=1.000) was observed between groups with regard to question 1 (3D better). Regarding question 2 (MPR better), the oral and maxillofacial surgeons had a higher percentage of affirmative answers than the radiologists. This was confirmed by the proportion test, which revealed statistically significant differences between groups (p=0.006). For the analysis of question 3, the Kruskal-Wallis test was used to compare the scores, revealing no significant difference between them (p=0.194). For question 4, Fisher's exact test was used, revealing no significant difference between groups (p=0.621).
DISCUSSION
Diagnosis of CH is only possible by image examination.
Most authors highlight the role of CT with
coronal slices and sagittal reconstructions in the
analysis of this disease. They also highlight the relation
between the hyperplastic coronoid processes
and zygomatic arches.1,4,10-12,14-17 We confirm, based
on this and other preliminary studies, that CT is
essential for distinguishing CH from TMJ dysfunctions
through different imaging exams. This is of
particular importance because upon further investigation,
many supposed TMJ disorders are found to
be CH. Our data confirm this, as 7.6% of the "TMJ
problems" were in fact CH pathologies.
In the present study, MPR and 3D reconstructions
showing hyperplasia of the coronoid process were
analyzed by experienced oral maxillofacial radiologists
and oral maxillofacial surgeons, the specialists
that deal with this type of pathology, and their
preferences were compared.
Tables 1 and 2 show that both the oral surgeons and
the oral radiologists stated that imaging methods,
combined or not, were essential for diagnosing and
interpreting CH correctly (Question 3), and that
they would request these tests to analyze and diagnose
the condition (Question 4).
The proportion test revealed no significant difference
between groups with regard to Question 1. The
percentage of affirmative answers was higher for
3D images than for MPR images. This means that
both the oral surgeons and the oral radiologists consider
that in most of the cases, 3D images were more
elucidative than MPR images to diagnose and interpret
CH correctly. This agrees the findings of
Guimaraes and Marie 18 (2005), who highlighted
the use of 3D reconstructions for the analysis of the
relation between hyperplastic coronoid processes
and zygomatic arches and bones.
Regarding Question 2 (MPR better), the oral surgeons
had a higher percentage of affirmative answers than
the radiologists. This was confirmed by the proportion
test, which revealed statistically significant differences
between groups. We believe that the difference is due
to the fact that oral surgeons are more familiar with
this imaging method, since it is used in a variety of
clinical situations in Oral and Maxillofacial Surgery.
Both groups considered the two imaging methods,
combined or not, very important for analyzing CH,
as shown by the percentage of answers to question
3 (need for these examinations). The Kruskal-Wallis
test revealed no significant difference between
groups. Participants would also request one or both
of the imaging tests to analyze CH. Fisher's exact
test revealed no significant difference between
groups for Question 4 (indication of examinations).
When the oral surgeons and the oral radiologists
analyzed the 3D reconstructions to evaluate
mandibular movement, hypomobility was present
in 55.2% of the cases analyzed (Graph 1) on the
same side of the affected TMJ. This agrees with the
findings of some authors, who report that limited
mouth opening was often due to CH rather than to
TMJ dysfunctions, as was believed at first.2,9,16,19 Imaging examinations are essential for analyzing
clinical cases of limited mouth opening with no pain,
as shown in this and in other preliminary research.
These examinations would allow practitioners to
analyze soft and bony structures of TMJ, as well as
the relation between the coronoid process and zygomatic
bone. By requesting such examinationss, specialists
would avoid overlooking the possibility of
hyperplasia of the coronoid process.
We conclude that both groups of examiners believe
that the combination of MPR and 3D reconstructions
are fundamental to correctly diagnose and
interpret CH, especially the latter, and would
request one or both examinations to diagnose it. A
significant difference was found between the examiners
regarding the use of MPR (p=0.006), with
only the oral radiologists considering that it is not
so elucidative for the diagnosis of CH.
1. Coll-Anglada M, Acero-Sanz J, Vila-Masana I, Navarro- Cuellar C, Ochandiano-Caycoia S, Lopez de-Atalaya J, Navarro-Vila C. Jacob's disease secondary to coronoid process osteochondroma. A case report. Med Oral Patol Oral Cir Bucal 2011;16:e708-710.
2. Pregarz M, Fugazzola C, Consolo U, Andreis IA, Beltramello A, Gotte P. Computed tomography and magnetic resonance imaging in the management of coronoid process hyperplasia: review of five cases. Dentomaxillofac Radiol 1998;27:215-220.
3. Mano T, Ueyama Y, Koyama T, Nishiyama A, Matsumura T. Trismus due to bilateral coronoid hyperplasia in a child: case report. J Oral Maxillofac Surg 2005;63:399-401.
4. Tucker MR, Guilford WB, Howard CW. Coronoid process hyperplasia causing restricted opening and facial asymmetry. Oral Surg 1984;58:130-132.
5. Balcunas BA, Gallimore R. Bilateral coronoid hyperplasia. Dentomaxillofac Radiol 1985;14:41-44.
6. Blanchard P, Henry JF, Souchere B, Breton P, Freidel M. Permanent constriction of the jaw due to idiopathic bilateral hyperplasia of the coronoid process. Rev Stomatol Chir Maxillofac 1992;93:46-50.
7. Giacomuzzi D. Bilateral enlargement of the mandibular coronoid processes: review of the literature and report of case. J Oral Maxillofac Surg 1986;44:728-731.
8. Loh HS, Ling SY, Lian CB, Shanmuhasuntharam P. Bilateral coronoid hyperplasia-a report with a view on its management. J Oral Rehabil 1997;24:782-787.
9. Hecker R, Corwin JO. Bilateral coronoid hyperplasia: review of the literature and report of case. J Oral Surg 1980; 38:606-608.
10. Munk PL, Helms CA. Coronoid process hyperplasia: CT studies. Radiology 1989;171:783-784.
11. Totsuka Y, Fukuda H. Bilateral coronoid hyperplasia: report of two cases and review of the literature. J Craniomaxillofac Surg 1991;19:172-177.
12. Gerbino G, Bianchi SD, Bernardi M, Berrone S. Hyperplasia of the mandibular coronoid process: long term follow-up after coronoidotomy. J Craniomaxillofac Surg 1997;25:169-173.
13. Halaszy EP, Palmero MG. hiperplasia coronoidea bilateral: un factor a considerar en la limitacion de la apertura bucal: reporte de tres casos. Acta Odontol Venez 1988;26:37-40.
14. Colquhoun A, Cathro I, Kumara R, Furguson MM, Doyle TC. Bilateral coronoid hyperplasia in two brothers. Dentomaxillofac Radiol 2002;31:142-146.
15. Gibbons AJ, Byrne AJ, Key SJ. Trismus due to bilateral mandibular coronoid hyperplasia. J R Army Med Corps. 2001;147: 311-313.
16. Hall RE, Orbach S, Landesberg R. Bilateral hyperplasia of the mandibular coronoid processes: A report of two cases. Oral Surg Oral Med Oral Pathol 1989;67:141-145.
17. Izumi M, Isobe M, Toyama M, Ariji Y, Gotoh M, Naitoh M, Kurita K, Ariji E. Computed tomographic features of bilateral coronoid process hyperplasia with special emphasis on patients without interference between the process and the zigomatic bone. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2005;99:93-100.
18. Guimaraes AS, Marie SK. Dominant form of arthrogryposis multiplex congenita with limited mouth opening: a clinical and imaging study. J Orofac Pain 2005;19:82-88.
19. Isberg A, Eliasson S. A cephalometric analysis of patients with coronoid process enlargement and locking. Am J Orthod Dentofac Orthop 1990;97:35-40.