











 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkKEY POINTS
• The outbreak of monkeypox occurred in 2022, lesions were mainly located in the genitalia and perianal region, while pro dromal symptoms were either mild or ab sent.
• In our study, sexual transmission was the main route of contagion. Almost all pa tients were young men, homosexual, and engaged in high-risk sexual practices. In 86.3% of 124 patients, systemic symptoms were present, and in 64.5% they occurred before the appearance of skin lesions. Most patients had regional lymphadenopathies and a moderate form of the disease. Com plications were seen in 55.6% of cases, and proctitis was the most frequent. The qPCR Ct was similar in samples of vesicles, pustules and scabs, regardless of duration of the disease.
Monkeypox (mpox) was first described in 1958 in Denmark in laboratory monkeys brought from Singapore, and the first case in humans was reported in 1970 in the Democratic Republic of Congo. Since then, epidemic outbreaks have occurred, especially in African countries, and since 2017, other countries have also reported cases. On July 23, 2022, the World Health Orga nization (WHO) declared a public health emer gency due to a new outbreak originated in May in Great Britain that spread quickly to the rest of the world. In November 2022, the WHO renamed the disease as mpox1,2.
The mpox virus (MPXV) belongs to the Pox viridae family (double-stranded DNA virus), Chordopoxvirinae subfamily and Orthopoxvi rus genus. There are two clades in Africa: one in Central Africa and one in Western Africa, with different epidemiological characteristics. The clade of Central Africa is prevalent in the Demo cratic Republic of Congo and other countries; it is clinically associated with a more severe dis ease and mortality may reach 11%. The clade of Western Africa is detected in Nigeria, Ivory Coast and Sierra Leone; it exhibits less human to human transmission and less clinical sever ity, with a mortality rate of up to 6%. A third variant appears to be responsible for the current outbreak; it is linked to the second variant, but is less virulent2,3.
The virus spreads from person to person through direct contact with the lesions in the skin, mucosae, body fluids, fomites and respira tory secretions, as well as via the placenta. Following the infection, the incubation period lasts between 5 and 21 days. Prodromal symptoms are fever, headache, asthenia and lymphadenopathy, followed by a rash that progresses through the stages of macules, papules, vesicles, pustules and scabs. The disease usually lasts 2 to 4 weeks2.
Historically, the clinical manifestation of mpox was a rash affecting multiple body re gions. In the current outbreak, lesions were mainly located in the genitalia and perianal re gion, while prodromal symptoms were either mild or absent2,4-6.
The goal of this study is to describe the epi demiological, clinical and virological character istics observed in the group of patients included. Among our specific goals, we sought to compare the incubation period in patients with confirmed and probable epidemiological link, analyze the relation between the type of sexual contact and the site of initial lesions, evaluate potential fac tors associated with complications and the se verity of the disease, and to analyze the relation of real-time PCR cycle threshold (qPCR Ct) with sample type and the time elapsed since the on set of the rash.
Materials and methods
Study design and participants
We performed a retrospective, observation al and analytical study in patients seen at the Dermatology Unit of a public Infectious Disease Hospital from the Government of Buenos Aires city. Outpatients were evaluated at the Sexually Transmitted Diseases (STDs) Clinic or the Der matology Urgency Room, while inpatients were seen in the hospitalization room, due to con sultations requested by other Departments. Pa tients included were assessed during the study period, from July 1st to October 31st, 2022.
The study was approved by the Ethics Com mittee of the hospital. Data were collected and analyzed anonymously and were not associated to patients’ identity. Patient consent was ob tained for publication of images.
Procedures
Patients were evaluated by 4 dermatologists. Subjects of any sex and age were included, with a confirmed diagnosis of mpox by viral detection with real-time PCR (qPCR) in swab samples of le sions and/or scabs.
Data were obtained from the medical records and the detailed clinical data were entered into a spreadsheet. Outpatients were initially evalu ated and followed with a weekly telephone call; at the end of the isolation period they were re-evaluated or before, if they presented intense pain, complications or at the request of the pa tients.
Samples were obtained from at least two dif ferent sites by swabbing vesicles or pustules or by scabs collected in sterile vials.
When more than one sample was obtained from the same patient, the sample with lower Ct value was selected for analysis.
Real time PCR for MPVX
Molecular diagnosis of MPXV was performed at the National Reference Institute for Infectious Diseases INEI-ANLIS Dr. Carlos Malbrán between May and August of 2022. Afterwards it was de centralized and the Virology Unit at our Hospi tal centralized the molecular diagnosis from the public health system of Buenos Aires city. The Ct values were only evaluated in the samples stud ied at our Hospital.
Extraction of nucleic acids was performed with automated equipment (MagnaBio plus Vi rus DNA/RNA purification kit III, Bioer), and the swabs were re-suspended in 600 μl of sterile saline solution; 300 μl were used for the extrac tion and a 300 μl aliquot was stored. Scabs were treated with tissue lysis buffer (DS BIO Quick Tissue/Culture cells Genomic DNA extraction kit, Dongsheng Biotech), and 300 μl were used for extraction.
The qPCR assay recommended by PAHO was employed which allows the detection of all MPXV strains form the G2R_G gene7,8, and the detection of the RNase P gene as sample’s cell control9. All swab samples with Ct values ≥34, and those with discordant results were re-ana lyzed from the nucleic acid extraction step on. In the case of scab samples with Ct values ≥34, the qPCR reaction was repeated before reporting the final result.
All patients were offered work-up studies to rule out other STDs (syphilis, HIV and hepatitis B and C).
Variables
Variables assessed are described in Tables 1 and 2.


Sexual orientation and gender identity: sexual orientation was classified as heterosexual, ho mosexual and bisexual, and gender identity as cis, trans and non-binary10.
Vaccines: the smallpox vaccine was adminis tered in our country until 1978, and individuals born until 1977 received at least one dose. The vaccine against mpox was not available in our country during the study period.
High-risk sexual practices: these comprised: lack of barrier methods during genital, anal or oral sexual relations during the past month, a history of STD during the past year, or the prac tice of chemsex.
Epidemiological link: it was considered con firmed when any of the following had a con firmed diagnosis of the disease: a sexual part ner, a non-sexual contact living with the patient, or a non-sexual contact not living with the pa tient. It was considered probable when there was no confirmed epidemiological link, but the patient had engaged in sexual intercourse during the previous 21 days, in an anatomical site coinciding with the site of the initial lesions. When none of the previous criteria were pres ent, the epidemiological link was considered to be absent.
Incubation period: interval between contact with the confirmed or suspicious case and the beginning of symptoms.
Initial symptoms: they were categorized as sys temic and cutaneous, and when both symptoms appeared concomitantly, they were included in the first group.
Time elapsed until scabs fall-off: interval be tween the appearance of the cutaneous and mu cosal lesions and fall-off of the last scab.
Body areas affected: they were divided into trunk (including the gluteal region), limbs (upper and lower limbs, palms and soles), genital region (including the pubis), perianal region (including the anal region) and cephalic pole (including the mouth). The disease was considered dissemi nated when 3 or more areas were affected.
Treatment with opioid pain relievers or corticoste roids: due to pain and inflammation caused by mpox.
Disease severity: it was categorized as mild (less than 20 lesions, without complications or disseminated disease, not requiring treatment with systemic corticosteroids or opioid pain killers), moderate (more than 20 lesions or with complications not requiring treatment with sys temic corticosteroids or opioid painkillers) and severe (at least one condition present: hospital ization -except for social reasons-, death due to mpox-related causes, complications requiring treatment with systemic corticosteroids and/or opioid pain relievers).
Time elapsed from skin involvement until viro logical testing: interval between the first sign of skin involvement and the moment in which the sample was obtained.
Statistical analysis
Quantitative variables were reported as mean and standard deviation (SD) or median and in ter-quartile range (IQR), according to their distri bution (Shapiro-Wilk test). Categorical variables were described as absolute and relative frequen cies. To compare quantitative variables, we used the t-test o Mann-Whitney-Wilcoxon test, ac cording to their distribution. For comparison of categorical variables, the Chi square or Fisher’s test were used. When p values were < 0.05 they were considered statistically significant. All sta tistical analyses were performed with R® soft ware, version 4.2.2, and its RStudio® interface, version 2022.07.1.
Results
A total of 126 patients with mpox were evalu ated during the study period; 124 were included and 2 were excluded because of missing data.
Demographic and epidemiological characteristics
Patients’ demographic and epidemiological characteristics are detailed in Table 1. Median age was 31.5 years (IQR: 28-38), 123 (99.2%) were men, of whom 107 (86.3%) were homosexual. High- risk sexual practices were recorded in 102 patients (82.3%), and the most frequent one was not using a barrier method in 97 (95%). Seven ty-five patients were HIV positive (60.5%) and only 10 (13.3%) had a CD4 T lymphocyte count (CD4TL) of less than 350/mm3.
Fifteen patients (12.1%) had received a small pox vaccine during childhood. No difference in disseminated disease was found between pa tients of this group and non-vaccinated patients [13 (86.7%) vs. 74 (67.9%), p = 0.23].
Among the 124 patients, 32 (25.6%) had a con firmed epidemiological link (87.5% referred a sexual contact with the source), 62 (50%) had a probable epidemiological link, and in 26 (20.9%) no link was found. In 4 cases (3.2%), this infor mation was not available.
Median duration of the global incubation pe riod was 7 days (IQR: 5-11), and no difference was found between patients with a confirmed versus probable epidemiological link [median (IQR) 7 (4.0-9.5) vs. 7 (6.5-12.5), p = 0.14].
Infection features
Mpox infection features are described in Ta ble 2. All patients exhibited skin involvement and 107 (86.3%) also had systemic symptoms, which were present since the beginning of the disease in 55.6% of cases (prodromal symptoms). The most frequent systemic symptom was fever (80.3%) and 112 patients (90.3%) had lymphade nopathy, which was generally regional (75.9%).
All patients had vesiculopustular rash (Fig. 1). Lesions began as papules, evolved to vesicles and then to pustules, many of them had a cen tral umbilication and were surrounded by an erythematous halo. Subsequently, the lesions became unroofed, leaving an erosion or ulcer ation and finally were covered by scabs. Vesicles and pustules were the most frequently found le sions on initial consultation (91.1%). Ninety-six patients (77.4%) presented with polymorphic skin lesions, i.e., appearance of more than one type of elementary lesion simultaneously.

Figure 1 Rash features of mpox: erythematous papules (A), pustules with central umbilication (B and C), erythematous halo (D), scabs (E) and lesion polymorphism (F)
The lesions first appeared in the genital and perianal regions in 74.2% of patients. Initial le sions in the genital region were seen more fre quently in patients who reported having genital intercourse compared to those who didn’t [47 (60%) vs. 0 (0%), p = 0.00007]. Likewise, lesions that appeared initially in the perianal region were seen most often in patients who reported having receptive anal intercourse vs. patients who didn’t [28 (48.3%) vs. 3 (11.1%), p = 0.0002]. In contrast, mouth lesions were not more fre quent in patients who had engaged in oral sex (p = 0.4221) (Table 3).

During the whole period of disease, 65.3% of patients had less than 20 lesions. The median number of affected body areas was 3 (IQR: 2-4): the limbs (77.4%) and genital area (73.4%) were the most affected regions. Most of cases (70.1%) were classified as disseminated skin disease, af fecting at least 3 body areas. Oral involvement was present in 39 patients (31.5%); erythema tous enanthema of the fauces (79.5%), erosions (51.3%) and petechiae (7.7%) were observed. Among those 39 patients, 14 had tonsillitis as a complication.
The last scab fell off after a median of 16 days (IQR: 13-18). In addition to the vesiculopustular rash, a small number of patients (6.5%) exhibit ed a concomitant maculopapular (morbilliform) rash involving the trunk.
Complications
Half of the patients (55.6%) had complications (Table 2, Fig. 2); among them, proctitis was the most common (59.4%) and in 68.2% of these pa tients, initial lesions appeared in the anal/peri anal region (Table 3).

Figure 2 Complications in individuals with mpox. Perianal lesions with proctitis (A), penile edema causing phimosis (B), purpuric plaque (C), ulcers with necrotic scabs (D), ulcers surrounded by pustules with an erythematous halo (E), and tonsillitis (F)
As to the overall frequency of complications, a significant difference was seen in patients with disseminated disease vs. those with local ized disease [56 (64.4%) vs. 13 (36.1%), p = 0.007]. Also, complications were greater in patients who presented initially with systemic symptoms vs. those with skin lesions [46 (66.6%) vs. 21 (41.2%), p = 0.009]; and the main complication was procti tis [31 (45.6%) vs. 8 (15.7%), p = 0.002]. By contrast, in patients with systemic symptoms no differ ence was seen between those with and without proctitis [38 (95.0%) vs. 68 (84.0%, p = 0.14]. Among the HIV population, proctitis was more frequent [33 (44.6%) vs. 8 (17.0%), p = 0.003], although they hadn’t an overall increased risk of complications [47 (63.5%) vs. 22 (45.8%), p = 0.08]. Also, no differ ence in the overall frequency of complications was found in patients with HIV and less than 350 CD4TL when compared to those with higher counts [29 (58.0%) vs. 8 (80.0%), p = 0.29]. Patients who had been vaccinated against smallpox dur ing childhood had a lower overall frequency of complications than non-vaccinated patients [4 (26.7%) vs. 65 (60.2%) respectively, p = 0.03]. How ever, and probably related to the small sample size, no difference was found when complica tions were analyzed individually (Fig. 3).

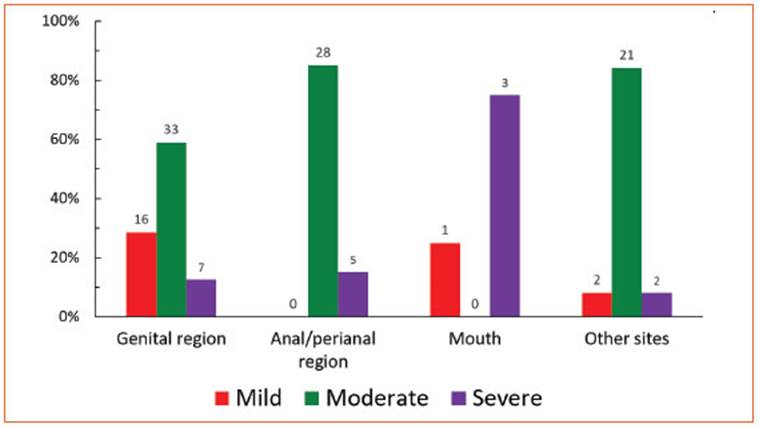
Disease severity
In 21 patients (16.9%) the disease was mild, while it was moderate in 85 (68.5%) and severe in 17 (13.7%); in one patient this information was not available (Table 2). Severity of the dis ease differed according to the site of initial le sions (p = 0.00004) (Fig. 4). In all patients with onset of the rash in the anal/perianal region, the disease was moderate or severe, in 82.3% due to proctitis. In contrast, severity of the disease was not different between patients with or without systemic symptoms (p = 0.16), between those who started the disease with systemic symp toms vs. with rash (p = 0.44), between patients with and without HIV (p = 0.82), nor between patients with HIV and CD4TL higher or lower than 350/mm3 (p = 0.13). All patients vaccinated against smallpox during childhood had moder ate disease.
Virological diagnosis of MPXV
The diagnosis of MPXV was made with a swab of a lesion in 102 cases (82.3%), with scab sam ples in 6 cases (4.8%), and in 16 cases (12.9%) us ing both types of samples. A qPCR Ct analysis was performed in the samples of the 98 patients assessed at the Virology Unit (Table 2).
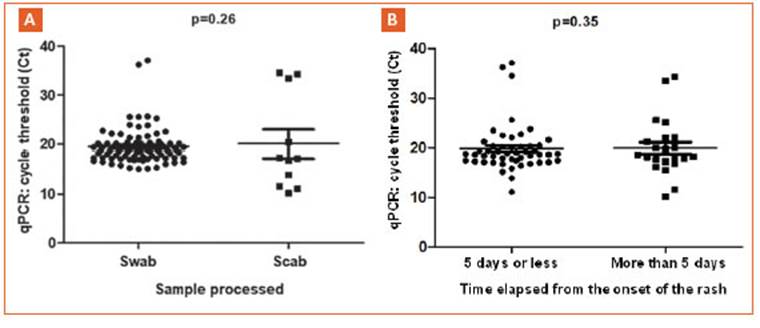
A median of 2 samples (IQR: 2-2) was ana lyzed for each patient. No difference was found in qPCR Ct between the samples of swabs vs. those of scabs [median (IQR) 18.8 (17.4-20.1) vs. 17.2 (12.75-26.9), p = 0.26], nor between samples from patients with evolution time of skin le sions of up to 5 days vs. more than 5 days [me dian (IQR) 18.9 (17.4-20.4) vs. 18.5 (17.2-20.1), p = 0.35] (Fig. 5).
Clinical course and treatment
Eight patients (6.4%) were hospitalized to pro vide pain management and treatment of com plications, and in two cases for contact isola tion. In our series, 18 patients (14.5%) required treatment with systemic corticosteroids and/ or opioid painkillers to reduce inflammation and pain. Two cases (1.6%) with HIV (CD4TL < 350/mm3) had severe disease with extensive skin necrosis, and required admission to the intensive care unit. Both patients were treated with tecovirimat at a dose of 600 mg BID, orally or by nasogastric tube; one during 4 days until his death due to ventilator-associated pneu monia11, and the other patient during 9 days with good clinical response.
Almost all patients recovered (99.2%). Con comitant STDs were detected in 42 patients (33.8%), syphilis being the most frequent.
Discussion
Since the beginning of the mpox outbreak in 2022, 87 113 cases have been reported world wide; affected countries are 111 and a 130 deaths were reported by the WHO. The highest number of cases was reported in the region of the Americas, and a per-country analysis shows that 84.4% of cases are concentrated in the U.S., Brazil, Spain, France, Colombia, México, Peru, the United Kingdom, Germany and Canada. Among affected patients, 96.2% were male, with a me dian age of 34 years12.
In Argentina, since epidemiological week 21, 2022, until week 16, 2023, confirmed cases were 1129, with 2 deaths. The highest number of cas es was reported between weeks 31 and 51, 2022. A 95% of the diagnoses was concentrated in the large urban conglomerates, i.e., Buenos Aires City, the Province of Buenos Aires and Córdoba. In Buenos Aires City, up to week 19, 2023, the to tal number of confirmed cases was 713, of which 215 have been studied at our institution12.
In our study we have included 124 patients evaluated at the Dermatology Department. Age, biological sex, sexual identity and sexual ori entation agree with the published data, with marked predominance of young men, cis and homosexual.
The following 4 findings of this study sup port the premise of sexual transmission as main route of contagion: 1) most patients (82%) re ferred high-risk sexual practices, in agreement with the literature13-15; 2) 87.5% of patients with confirmed epidemiological link had engaged in sexual contact with the source; 3) initial le sions in the genital and perianal regions were associated with a history of sexual genital and/ or anal receptive intercourse respectively, and 4) in 74.2% the onset of the rash was in the genital and perianal regions. Among these patients it is essential to rule out other STDs; in our series they were present in 33.8% of them.
The overall incubation period was 7 days, co inciding with observations of other authors2,4,13. No difference in incubation period was seen in patients with vs. those without a confirmed epi demiological link.
Systemic symptoms were frequent (86.3%) and they were present since the beginning of the disease in more than half of cases as pro dromal symptoms; fever was seen most often, as described by other authors2,4,13,16,17.
Regional lymphadenopathies were observed in the majority of cases and were generalized in 24%; this finding was not cited frequently in the literature.
All our patients exhibited skin involvement with a vesiculopustular rash and a median of 3 regions involved. Although this was similar to the findings published by Tarin-Vicente et al4, both studies classified body regions differently. Most of our cases (70.2%) were categorized as disseminated disease, which differs from what has been described for this outbreak, with le sions that tend to be located in the site of inocu lation. As previously reported4,13,18, we found that the 2 most affected regions were the limbs and genital area, although in our series the limbs were involved more often. This may be explained by the fact that in our study the hands and feet were included in the limbs region, while other authors did not group both areas. Macular exan thema was observed with similar frequency (6%) to that of previous reports4,17.
The mouth was affected in 31% of patients, a higher rate (7-25%) than that of other publi cations, and consisted in erythematous enan thema of the fauces, erosions, ulcerations and petechiae4,16-18.
In accordance with previous publications, proctitis was the most frequent complication (33%)2,4. We found a greater risk of complications among patients whose initial symptoms were systemic and/or who presented with dissemi nated lesions.
To classify severity we considered the num ber of lesions, areas involved, complications, re quirement of opioid pain relievers or systemic corticosteroids for pain management, hospitalization or progression with death; this dif fered from other studies that only considered the number of lesions for that purpose4. This classification would allow a better selection of patients requiring closer monitoring and/or antiviral treatment. Regarding severity of the clinical presentation, we found no difference between patients with and without HIV, which coincides with previous reports. Among patients with HIV, we found no difference between those with CD4TL titers higher or lower than 350/mm3. However, 2 patients with HIV (and less than 100 CD4TL) had severe disease associated with extensive skin necrosis. Oriol, Mitjà et al19, described this clinical presentation in a subgroup of patients with a CD4TL count of less than 200/ mm3, associated with a 15% mortality.
The Ct value indicates the number of cycles required for amplification and detection of the viral genetic material in a certain sample, and is inversely proportional to the amount of virus present in that sample. In our study, median Ct value was 18, similar in swab and scab samples (p = 0.26). Although the number of the latter was small, it allows to infer that scabs are useful samples, despite their processing is more com plex. Since Ct did not differ in samples from pa tients with skin affected for less or more than 5 days (p = 0.35), samples seem to be adequate for diagnosis and also a possible source of con tagion.
During the 2022 outbreak, worldwide mortal ity was 0.1%, related to encephalitis and in im munosuppressed hosts. In Argentina, the rate is similar and, of the two deaths reported, one was a patient with HIV who developed the se vere form of mpox and is included in this se ries2,11.
A literature review showed that during the current outbreak, about half of the patients required treatment for pain relief2. In our se ries the percentage is lower, since we only considered opioid pain relievers and systemic corticosteroids. In our country, specific treat ment for mpox is not available, however, two patients received tecovirimat as compassion ate use.
Few cases of re-infection have been reported until present20-22. One patient of our series pre sented reinfection after the study period. We be lieve that studies assessing the duration of im munity and long-term impact on re-infections, as well as the protective role of the smallpox vaccine administered during childhood are nec essary. Importantly, all countries should have access to specific treatment for mpox.
Among the study limitations, its retrospec tive nature could have led to omission of certain data, and the fact that only patients seen by the Dermatology Department were included. How ever, a substantial number of patients were as sessed in detail and all had a confirmed virologi cal diagnosis.
In conclusion, this study allows to better un derstand the clinical manifestations of mpox in our country. It is important to suspect the disease in subjects with high-risk sexual practices and a consistent clinical presentation, with or without systemic symptoms. Even if there is no history of travel or contact with foreigners, the diagnosis should be suspected. Because of the sexual trans mission of the disease, concomitant STDs should be ruled out. Swab samples of lesions as well as of scabs have proven useful for the diagnosis.
Additionally, the study contributes to expand the information and adopt prevention measures regarding this disease and to establish priorities for vaccination.

