











 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkINTRODUCTION
Tracheal plasmacytomas are unusual findings. In our case, the patient has multiple myeloma of poor evolution with hemoptysis caused by the tracheal lesion. Due to the fact that it is a high-risk patient, we decided to use minimally invasive endoscopic techniques, and a good result was obtained without recurrence of blood expectoration.
CASE REPORT
Patient diagnosed with multiple myeloma, IgG kappa, stage IIIA, ISS (International Staging System) 2, who has been receiving follow-up treatment by the Hematology Service of the Hospital Universitario Miguel Servet since 2014. The patient showed torpid evolution with eight lines of treatment, including autologous hematopoietic stem cell transplant in 2015, with disease progres sion until today. The patient is currently receiving treatment with daratumumab.
The patient went to the Emergency Department due to hemoptysis and said that he/she had expecto rated red blood and hadn’t had any previous episodes. He/she had a thrombocytopenia of 59,000 platelets per milliliter; chest X-ray without acute alterations. Due the acute condition, he/she was admitted to the Pulmonology Department to be evaluated.
At the time of admission, the patient was hemo dynamically stable, with blood-streaked sputum. He/she was referred to the Otolaryngology Service for assessment: it reported normal oropharynx without blood residue, normal cavum and normal hypopharynx and vallecula. The epiglottis was free and without lesions, and the pyriform sinuses were free and open. Finally, the vocal cords were free, mobile and lesion-free. When the patient was asked to cough, a bloody mucus clot was observed. No lesions or blood were observed at the upper level of the airway.
Due to the suspicion that blood could be com ing from the bronchial tree, a bronchoscopy was requested.
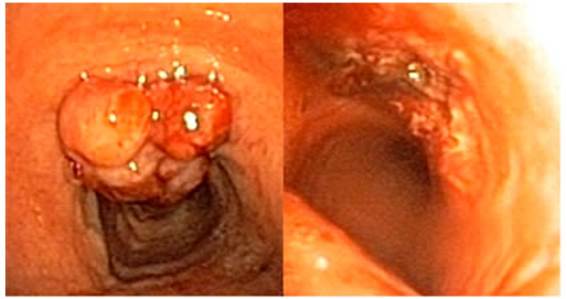
The bronchoscopy showed an irregular papilli form nodule of exophytic growth in the anterior wall of the trachea, two centimeters apart from the vocal cords, showing signs of recent bleeding but without active bleeding at the time of the screening. Despite the lesion, the trachea had a 70% free lumen.
Considering such findings and taking into ac count that the patient had thrombocytopenia, a new bronchoscopy was set for two days later, with biopsies and laser vaporization of the lesion.
When screening the patient’s trachea, a clear increase in the size of the lesion was observed. The bi opsy was performed without significant findings, and samples were sent to the hospital’s pathology labora tory. After laser vaporization of the lesion, there was 100% tracheal lumen, with good macroscopic result. The patient didn’t show signs of extrinsic compression or dynamic collapse of the airway.
The final pathology report characterized the le sion as plasmacytoma with diffuse plasma cell pro liferation, with restriction of the Kappa light chain.
A new positron emission tomography was per formed six weeks after resecting the lesion. The tomography showed multiple myeloma with signs of progression due to a lesion in the anterior wall of the trachea. Pre-existing lytic lesions showed an increase in the metabolic activity together with generalized hypermetabolism in the spinal cord.

DISCUSSION
This case is interesting because this type of tumor in the trachea is very rare,1,2 and because of the good results obtained with the endoscopic tech niques that were used. The tumors of plasma cells are divided in: multiple myeloma, extramedullary plasmacytoma, and solitary plasmacytoma of bone.3
Extramedullary plasmacytomas more com monly occur in the upper part of the digestive tube and the upper airway. We might find this type of neoplasm generally in the nasal cavity, nasal sinuses, and the oronasopharynx. 1,2
This finding has been described in the literature on rare occasions. Clinical symptoms can be non-specific and often related to tracheal invasion. Croup, chronic cough, dyspnea, voice alterations, sibilance or hemoptysis, as in our case, can be manifestations of this disease.1,2,4
The diagnosis of this particular case couldn’t be considered as extramedullary plasmacytoma itself, since this disease refers to only one lesion without affecting the bone marrow or skeleton, and without causing anemia, hypercalcemia or renal alterations.5
Our patient shows multiple myeloma refractory to treatment. It is true that 20% of patients with extramedullary plasmacytomas can progress to multiple myeloma.3
The presence of extramedullary disease in a patient diagnosed with multiple myeloma is associ ated with a worse prognosis and could be related to secondary changes in the cell clone, aggressive progression of the disease or treatment resistance, like in our case.6
The cell clone that is responsible for the my eloma could even be different from the one respon sible for the extramedullary plasmacytoma, thus the treatment becomes complex.6
The treatment of soft-tissue plasmacytomas is controversial, and is commonly managed with sur gery or radiation therapy.5 In our patient, the lesion was resected by endobronchial laser vaporization. Despite the resection, the positron emission tomogra phy showed a metabolically active uptake in the site where the lesion had previously been found, so it will be necessary to perform a clinical follow-up in order to evaluate the effectiveness of the intervention.

