











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Similars in
SciELO
Similars in
SciELO 
 Permalink
PermalinkKEY POINTS
• ANCA-associated vasculitis affects small to medium-sized vessels
• They can be associated with irreversible damage to the organ function or even the death of the patient
• The generalized and severe clinical forms were the most frequent
• Survival rate was lower in patients with microscopic polyangiitis, Five Factor Score of 2, age ≥ 55 years old and alveolar hemorrhage
Anti-neutrophil cytoplasmic antibodies (ANCA) were first described in 1982 in a patient with pauci-immune glomerulonephritis1. ANCA-associated vasculitides en compass four entities: granulomatosis with polyangiitis (GPA), eosinophilic granulomatosis with polyangiitis (EGPA, also known as Churg-Strauss syndrome), mi croscopic polyangiitis (MPA) and renal-limited vasculitis (RLV)2. In Argentina, Pierini estimated the incidence rate of GPA and MPA at 9 and 14 cases per million person-year, respectively, and the prevalence rate at 7.4 and 5.2 cases/100,000 people, respectively3.
GPA often involves upper and lower respiratory tract and biopsy samples typically show the presence of granulomas. Often MPA occurs as pulmonary capillaritis associated with renal involvement, with no granulomas on biopsy. Asthma is the principal clinical feature of EGPA. Eosinophilia and vasculitis manifestations appear later; the histology reveals granulomas with plenty of eosinophils. Although all forms of vasculitides may appear as rapidly progressive glomerulonephritis, the characteristic of RLV is that clinical manifestations are limited to the kidneys with no other organ involvement. The pathological findings are indistinguishable from those in the other entities4.
Treatment options depend on the severity of clinical manifestations. In general, treatment includes two phases: remission induction and maintenance. Despite the fact that significant progress has been made in both phases during the last decades, the relapse rates and the toxicity associated with treatment remain high5,6.
The factors associated with prognosis include, among others, older age, a higher initial BVAS (Birmingham Vasculitis Activity Score) or FFS (Five Factor Score), MPO-ANCA positivity, renal involvement and a high VDI (Vasculitis Damage Index)7-10.
The aim of the present study was to describe the clinical features, as well as the prognostic factors, of the patients with ANCA-associated vasculitides treated in a university hospital in Buenos Aires during the last 35 years.
Materials and methods
A descriptive study by reviewing the medical records of pa tients with ANCA-associated vasculitis who had their first symptoms between July 1984 and March 2019 was carried out. The study included patients over 18 years old who met the American College of Rheumatology (ACR) classification criteria for GPA or EGPA, or the GPA, EGPA or MPA defini tions according to the 2012 Revised International Chapel Hill Consensus Conference Nomenclature4,11,12. It was considered that a diagnosis of pauci-immune glomerulonephritis confirmed by renal biopsy in an ANCA-positive patient with no clinical manifestations other than renal involvement was consistent with RLV. The protocol was approved by the Ethics Commit tee of the Institution and was conducted in accordance with the guidelines set by Act 3301/09 of the Ministry of Health of the Government of the City of Buenos Aires and those of the Helsinki Declaration.
Our Institute has had indirect immunofluorescence (IIF) for ANCA detection since 1992 and enzyme immunoanalysis technique (ELISA) since 1996. At least one determination of these antibodies using anyone of these methods was recorded for each of the patients included in the study. Two patterns were identified by IIF: cytoplasmic (c-ANCA) and perinuclear (p-ANCA), which were considered to correspond to autoan tibodies against Myeloperoxidase (MPO) and Proteinase 3 (PR3) antigen respectively, according to ELISA.
Demographic data were collected, as well as clinical mani festations at diagnosis, the complementary studies performed and the treatments received during the course of the disease. Diagnosis delay was defined as the time to diagnosis after the onset of vasculitis-related symptoms. Pulmonary-Renal Syndrome (PRS) was defined by the occurrence of renal and respiratory failure as a manifestation of rapidly progressive glomerulonephritis and diffuse alveolar hemorrhage. Anemia was defined as hemoglobin in blood < 12 g/dl and < 13 g/dl in men and women, respectively13. BVAS was calculated at diagnosis, after treatment and at every relapse, and 2009 FFS was calculated at diagnosis5,14.
EULAR (European League Against Rheumatism) recom mendations for conducting clinical studies in systemic vas culitides were used to assess the stages of the disease, the response to treatment and relapses. Localized forms were defined as the upper and/or lower respiratory tract involve ment, with no systemic involvement. Early systemic forms were defined as systemic involvement with no threat either to the function of the organ or to the patient’s life. Generalized forms of vasculitis were described as involving kidneys or other organs as well as their functions, with creatinine in blood lower than 5.6 mg/dl. Severe forms were defined as those including renal or another organ involvement, with creatinine higher than 5.6 mg/dl. Progressive refractory forms were defined as those that do not respond to corticosteroid or cyclophosphamide treatments15. To assess the effects of treatment, remission was defined as the absence of active disease (BVAS = 0) for at least 3 months with doses of prednisone or equivalent ≤ 7.5 mg/day, whether or not associated with a steroid sparing agent (methotrexate, azathioprine or mycophenolate). Response to treatment is defined as a reduction in BVAS ≥ 50%. Refrac tory forms were considered to include at least one of the fol lowing: 1) greater activity measured by BVAS with or without change in treatment after 4 weeks with cyclophosphamide and corticosteroids; 2) lack of response with <50% reduction in disease activity score (BVAS) and/or lack of improvement of at least one major item after 4-6 weeks’ treatment; (3) chronic persistent disease, defined as the presence of at least one major item or three minor items on BVAS in spite of 8 weeks’ treatment. Persisting minor symptoms that responded to a modest increase in the medication and did not require a further escalation of treatment were recorded as low activity disease14. The re-occurrence of disease activity attributable to active inflammation was considered a relapse. A major relapse was defined as the re-occurrence of organ- or life-threatening disease activity that could not be treated with an increase of corticosteroids alone and required further escalation of treat ment. All other relapses were classified as minor relapses.
The results are expressed as percentages for categori cal variables and as mean ± standard deviation or median (range) for numerical variables. To compare groups defined by prognosis scores and disease activity, Chi-square test or Fisher test were used for proportions and one-way ANOVA or Kruskal-Wallis test for numerical variables.
Survival analysis was performed using Kaplan-Meier meth od. Follow-up time was computed in years between diagnoses and death or until the last clinical evaluation available in the medical records. Cox proportional analysis was used to evalu ate factors associated with mortality. A p value below 0.05 was considered statistically significant.
Results
Forty-seven patients with ANCA-associated vasculitides were included in the analysis, 28 women (59.6%) and 19 men. Mean age at diagnosis: 53.5 ± 16.5 years. Twenty patients were diagnosed with GPA (42.5%), 17 with MPA (36.2%), 6 with RLV (12.8%) and 4 with EGPA (8.5%). Median diagnosis delay was 2.46 (range = 0-411) months and 70.2% of the patients were diagnosed less than 6 months after the onset of the symptoms. Table 1 and Table 2 show demographic, epidemiological char acteristics and clinical manifestations at diagnosis. In 11 patients, the initial presentation was as Pulmonary-Renal Syndrome (PRS).


All patients started treatment with corticosteroids (1 mg/kg/day of prednisone or equivalent). Severe cases (28 patients, 59.6%) were initially treated with a pulse therapy of methilprednisolone (0.5-1g/pulse/day) for 1-3 days. Another immunosuppressant, including cyclophos phamide (CYC), was added in 39 (83%) patients (Table 3). The median of the duration of the treatment with oral CYC was 13 months (range 3.8-66.5). The median of number of intravenous (IV) CYC pulses was 6 (range 1-16). Seven patients were later switched to azathioprine (AZA) and 2 to mycophenolic acid. Rituximab (RTX) was used in 2 cases and one of them was treated later with AZA for mainte nance. Six patients were treated with plasmapheresis and 12 needed dialysis (4 on a temporary basis).

The outcome results after not less than 3 months from the onset of the initial treatment could be recovered in 42 patients (Fig. 1).

In a median follow-up period of 35.5 months (range 0.14-234) there were 21 relapses in 14 patients (6 with MPA, 6 with GPA, 2 with EGPA). Table 4 shows data for the patients who had a relapse and Table 5 for those with multiple relapses and refractory vasculitis.
After diagnosis, 32 infection episodes which required hospitalization were recorded for 16 patients: pneumonia (11), sepsis (11), infections by opportunistic pathogens (6, which included 3 by fungi, 2 by herpes zoster and 1 by Clostridium difficile), pyelonephritis (3) and dacryocystitis (1). Three patients had neoplasia (2, skin and 1, colon). There were 15 cardiovascular events in 10 patients: heart failure (6), venous thromboses (4), acute myocardial infarction (2), hypertension urgency (1), dilated cardio myopathy (1) and atrial fibrillation (1).
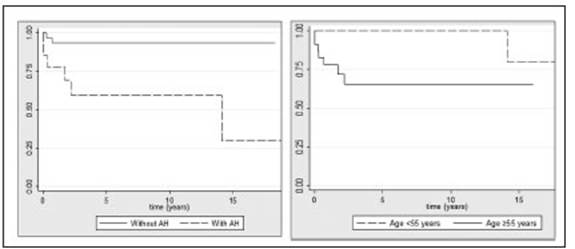
Nine patients died (4: GPA and 5: MPA), the causes of death were disease activity (5), infection (2) and cardio vascular (2). Of 11 patients who had PRS, 4 died within 16 weeks from diagnosis. Overall mortality was 3.5 deaths per 100 patient-year and was almost the same in subgroups defined by gender and BVAS at diagnosis. Out of 11 pa tients who had PRS, 4 died within 16 weeks. There were statistically significant differences comparing patients under 55 years old and ≥ 55 years old (p = 0.029) and between those who had had alveolar hemorrhage and those who had not (p = 0.011). Figure 2 shows survival curves. Sur vival was lower for patients with MPA (p = 0.074) and in patients with an FFS of 2 compared to 1 (p = 0.07), but the differences did not have statistical significance.
Discussion
ANCA-associated vasculitides are a heterogeneous group of rare autoimmune conditions, of unknown cause, that affect small to medium-sized blood vessels. They may involve many organs, including the upper airway, lung and kidney. Their incidence increases with age and they are more common in people of 60 years or older16,17. Our study evidenced a predominance of women, greater in MPA, according with findings by Cisternas, Paolini and Di Benedetto18-20 for the same continent and Schirmer JH et al24 in Germany. Although some studies described a similar sex distribution or a slight predominance in men17. Table 6 shows a comparison of the data of this study with those reported for other South American and European cohorts. All described a median age at diagnosis higher in MPA than in GPA18-21.



Delayed diagnosis of vasculitis may lead to irrevers ible damage to the organ function or even to death. There is great disparity among the different series17,19,21,22. In this study, 70.2% of the patients were diagnosed less 6 months after the onset of the symptoms. This could be accounted for by the fact that this is a third-level complexity center with experience in rare pathologies and the availability to perform biopsies and determine specific antibodies.
In GPA, upper airway involvement is often more frequent than pulmonary involvement; it may appear as frequent nasal discharge, crusts, rhinosinusitis or even po tential structural damage such as “saddle” nose deformity and subglottic stenosis. In one of the largest GPA series, with 158 patients, Hoffman et al reported upper (73%) and lower (45%) airway involvement at diagnosis25. In Argentina, Paolini showed greater pulmonary involvement at diagnosis (see table)19. Orden showed in 37 patients with GPA, after 6.2 years’ follow-up, that 48.6% had upper airway involvement and 81.1% had lower airway involvement26. In this study, we had similar results to those reported by these authors, with a predominance of lower airway involvement.
In MPA, clinical presentation generally includes less frequent involvement of upper airway and more severe renal involvement sometimes due to late diagnosis, also accompanied by greater renal damage and poor therapeu tic response29. In this study, diagnosis delay was similar in patients with MPA and patients with other entities, but MPA was associated with poorer prognosis, possibly related to older age at diagnosis and higher frequency of alveolar hemorrhage and renal involvement.
Pulmonary-Renal Syndrome (PRS), described by Goodpasture in 1919, may result in a life-threatening condition for patients and requires immediate immuno suppressive therapy27. It is characterized by crescentic glomerulonephritis and pulmonary capillaritis at pathologi cal anatomy. The most frequent causes of this syndrome are associated with ANCA vasculitides28. In this series, out of 11 patients who had PRS, 4 died within 16 weeks from diagnosis and the presence of AH was associated with poor prognosis.
With respect to ANCA antibodies, patients with GPA are usually c-ANCA positive, especially in the generalized and active forms of the disease, while p-ANCA positivity is more frequent in MPA and LRV. Up to 40% of the patients with EGPA are ANCA positive, predominantly p-ANCA30,31. In the present study, the proportions of ANCA positivity in GPA, MPA and LRV were similar to those studies, but patients with EGPA were mostly c-ANCA positive.
The treatment of ANCA-associated vasculitides has changed over time, always with the purpose of achiev ing remission with the least possible toxicity. So, the high doses of cyclophosphamide reported by Fauci and Wolff in 1973 and 1974, respectively, were switched to an induction phase with IV CYC pulses followed by a maintenance phase with less-toxic drugs32-34. Nowadays, rituximab appears as a new alternative in selected cases. This study covers a 35-year period and is representative of this treatment trend. During the first years covered by this study, most patients were treated with CYC during long periods of time, without maintenance treatment with another safer medication. Later, in an attempt to reduce toxicity, there was a switch to intermittent pulse intrave nous CYC and maintenance therapy with methotrexate, azathioprine or mycophenolate
In 2011, Flossmann et al. reported on the long-term follow-up of the most important clinical trials in ANCA-associated vasculitides. According to their findings, advanced age, glomerular filtration rate below 15 ml/min, high BVAS and low levels of hemoglobin at diagnosis were higher mortality predictors35. On the other hand, in a long-term follow-up of patients diagnosed with GPA and MPA enrolled in the WEGENT study, advancing age was the only factor significantly associated with the risk of death; each additional year of age increased the probability of death by 9%36. In this series, age, alveolar hemorrhage, FFS and MPA were related with prognosis. Unlike other series, renal involvement, ANCA pattern and BVAS were not associated to poor prognosis7-9,19.
BVAS was developed and validated in 1994 for use in the assessment of vasculitis activity and was subse quently modified to the current version: BVAS v.3. It is recommended by EULAR for use in clinical trials. It has proved to be a useful tool in the assessment of disease activity and response to treatment and as a prognostic factor14,15. In this series, the median BVAS at diagnosis was lower than that reported in other studies21,29,37, but similar to other cohorts34,38. The initial BVAS was not as sociated with mortality.
FFS was initially designed to predict survival at diagno sis in patients with polyarteritis nodosa, EGPA and MPA. It was developed by the French Vasculitis Study Group (FVSG) for use in a cohort the results of which were pub lished in 1996. A revised version in 2009 included patients with GPA and established that the following variables have a score of one point each: age above 65 years, heart failure, renal insufficiency (stabilized peak Cr ≥ 1.7 mg/dl), gastrointestinal involvement and absence of ear, nose and throat involvement5. The 5-year mortality rates for FFS 0, 1 and ≥ 2 were 9%, 21% and 40%, respec tively. A number of studies reported results on the use of this tool in the treatment of their patients, which included making therapeutic decisions or predicting relapses38-42. In this study, patients with an FFS of 2 had poor prognosis.
This study is limited by the size of the sample which did not allow for the adjustment of the analysis, and by its retrospective design that includes patients diagnosed during a 35-year period, under heterogeneous treatments which depended on the discretion of the treating physician at a given historical context. The strength of the study lies in the rare occurrence of this group of entities and the scarcity of literature on the subject in this region.
In summary, in this study we found a predominance of the female gender, mainly in MPA and greater involvement of lower airway in GPA, as other authors. Those over 55 years old, the presence of alveolar hemorrhage, those with FFS of 2 and patients with MPA had poor prognosis. Renal involvement, ANCA pattern and BVAS were not associated to a poorer prognosis.

