











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Similars in
SciELO
Similars in
SciELO 
 Permalink
PermalinkVulvar cancer accounts for about 0.4% of all cancers, with preference for older-aged women in the seventh decade of life1. The most common histological type is the squamous cell carcinoma, diagnosed in 90% of cases, followed by melanomas, extramammary Paget’s disease, adenocarcinomas, basocelular carcinoma, sarcomas and undifferentiated carcinomas1,2.
Primary gynecological sarcomas are infrequent and account for 3 to 4% of all the malignant neoplasm of the female genital tract, with anatomical distribution as follows: uterus 85% of the cases, ovary 8%, vulva and vagina 5%, and the remaining 2% in other gynecologic organs, being leiomyosarcoma the most frequently seen histological type, followed by endometrial stromal sarcoma3.
The scientific literature has reported fewer than 60 cases of dermatofibrosarcoma protuberans (DFSP) with an extremely rare location in the area of the vulva4-6, according to the new WHO classification of soft tissue tumors, it belongs to the category of fibroblastic/ myo fibroblastic tumors with differentiation of intermediate biological potential7, being locally aggressive, marked tendency for local recurrence and extremely infrequent distant metastases2,6,8.
Clinical case
A 54-years-old woman with a lesion in labia majora, progres sive growth, painless, and firm on palpation, accompanied by slight hyperpigmentation of the surrounding skin. On physical examination no suspicious adenomegalies were identified in the inguinal region. The gynecological examination was otherwise normal. Non-contrast and contrast-enhancing MRI were obtained reporting an expansive growth tumor in the vulva, solid in appearance and infiltrating the subcutaneous tissue. The oncologic gynecology department decided to surgically excise the lesion with circumferential peripheral and deep margins.
The macroscopic histopathology report describes it as a tu mor which largest diameter measures 12 cm, partially covered by light brown skin with irregular edges and firm consistency (Fig. 1). The microscopic examination shows a proliferation of spindle cells with hyperchromatic nuclei, organized in a storiform pattern with frequent mitotic figures (7 mitoses per 10 high-power fields), infiltrating from the reticular dermis to the subcutaneous cellular tissue. No tumor necrosis was identified, nor lymphovascular or perineural invasion. Margins were lesion free. The immunohistochemistry exhibited strong positivity of the tumor cells for CD34 and Vimentin, and no reactivity for AML, S100, Factor XIIIA and Desmin: The cell proliferation index measured with KI-67 was 60% (Fig. 2). With these findings the diagnosis of Dermatofibrosarcoma Protuberans was established. Since the peripheral and deep margins were not involved, the patient continued under strict monitoring, not requiring other surgeries and/or drugs.

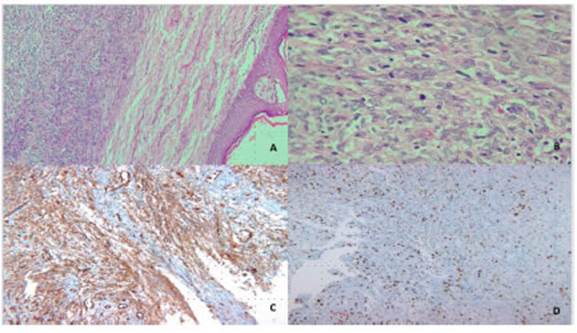
Fig. 2 A and B: Hematoxylin and eosin (H&E) staining, 10x and 40x. A tumor is found in the reticular dermis, pleomorphic spindle cells with frequent atypical mitotic figures in a storiform pattern. C: Strong and diffuse immunohistochemistry marking of tumor cells for CD34. D: 60% cell proliferation index measured with KI-67
Patient had a local recurrence at 6 months from the diagnosis, with a new 5 cm tumor in the previous scar area, which required the complete excision of the lesion with broad surgical margins. Therefore, molecular cytogenetic studies were carried out in biopsy, finding the chromosomal translocation t (17; 22) (q22; q13) with the COL1A1-PDGFB fusion gene, which motivates the initiation of neoadjuvant therapy with imatinib, to perform tumor cytoreduction, showing as response the decrease of 1.5 cm in diameter. Subsequently, the complete excision of the lesion was carried out with surgical margins of 2.2 cm and 1.5 cm towards the circumferential and deep lateral edges. The patient is currently progressing satisfactorily without evidence of new local recurrences and without metastatic lesions.
Written informed consent was obtained from the patient for the publication of this case report and its accompanying images.
Discussion
Dermatofibrosarcoma protuberans is a rare skin mesen chymal fibrohistiocytic lineage neoplasia which arises in the dermis and hypodermis and accounts for 1% of all soft tissue sarcomas9. The most frequent locations are the trunk, proximal extremities and in lower proportions the head and neck2,9, with equal distribution in men and women towards the fourth decade of life6.
The finding of such a tumor in the vulva is very unusual and only series of reported cases are found in the inter national scientific literature2,5,6,8,10-12, with the pathology prevailing in young adult females (fourth or fifth decade of life), clinically described as a firm and nodular mass, growing slowly, asymptomatic, painless, with an average largest diameter of 4.2 cm 4 and located predominantly in the labia majora, followed by the mons pubis and the area adjacent to the clitoris2,4-6,8,10-12. In the current case, the patient showed the initial large lip lesion and local recur rence on the surgical scar, following the 6 months after the first intervention, denoting clinically aggressive biological behavior. Among the differential diagnoses included in the clinical analysis are the following: abscess, Bartholin gland cysts, sebaceous cyst and other soft tissue neoplasms2.
Histologically, it is represented by neoplastic spindle cells arranged in storiform or honeycomb patterns, dif fusely infiltrating the dermis, subcutaneous adipose tis sue and on many occasions even the adjacent muscle tissue, as observed in the histopathological study of the case show, where the positivity of the strong and cyto plasmic immunohistochemical markers for CD34, with a high mitotic index measured with KI-67 and negativity for AML, Factor XIIA, HMB45, STAT-6 and S100, support a diagnosis of dermatofibrosarcoma protuberans, this im munophenotype being commonly reported in the scientific literature as characteristic of this tumor lesion, together with the expression of other markers such as PDGFR-a, PDGFR-b and c-Abl2,6. This immunoprofile allowed to rule out the diagnostic possibilities from the histological point of view, such as neurofibroma, cellular dermatofibroma, malignant tumor of the peripheral nerve sheath, Schwan noma, desmoplastic melanoma, myxoid liposarcoma, leiomyosarcomas and solitary fibrous tumor2,6.
In the vast majority of classical dermatofibrosarcoma protuberans cases and its variants the recognized carci nogenesis mechanism is the presence of chromosomal translocation t (17; 22) (q22; q13), resulting in a ring chromosome from the fusion of the gen collagen type I alpha 1 chain and platelet-derived growth factor B-chain gene (COL1A1-PDGFB), which encodes a chimeric pro tein structurally indistinguishable from subunit β of the platelet-derived growth factor (PDGF), which receptors are expressed in the DFSP tumor cells, and capable of stimu lating cell proliferation through autocrine mechanisms2,4,9.
Recently, in case series the presence of alternative rearrangements in dermatofibrosarcomas protuberans without PDGFB fusions, in which the fusion Collagen Type VI Alpha 3 Chain - Platelet Derived Growth Factor D (COL6A3-PDGFD)13 was more frequently identified in chromosomal position 2q37.3 - 11q22.3, evidencing ge nomic imbalance in the breakpoints and some numerical alterations with additional copies, which mainly through PDGFD, stimulates cell proliferation and angiogenesis14. Another fusion recognized in association with PDGFD is elastin microfibril interface-located protein 2- Platelet Derived Growth Factor D (EMILIN2-PDGFD)13, whose chromosomal location is 18p11.32-11q22.3 and is as sociated with homozygous deletion of CDKN2A, whose biological behavior reveals fibrosarcomatous transforma tion and tumor growth in the hypodermis with no connec tion to the dermis14.
The recommended treatment for DFSP in the vulva according to the National Comprehensive Cancer Network Guidelines is surgical excision with Mohs micrographic surgery or other surgical techniques for Complete cir cumferential peripheral and deep margin assessment (CCPDMA)15, with a strict post-op follow up. However, in surgically unresectable tumors neoadjuvant therapy is considered with imatinib, a tyrosine kinase inhibitor that blocks the cell cycle progress, in a context where cytoge netics (conventional or molecular) allows to identify the translocation t (17; 22) (q22; q13)15. On patients with mar gin involvement, surgical extension is recommended and in local recurrences and metastasis, adjuvant radiotherapy is indicated with 50-60 Gy, or the use of imatinib2,6,15.
In this case, it was decided to performed neoadjuvant imatinib therapy, a tyrosine kinase inhibitor that blocks the advancement of the cell cycle15, because the t (17; 22) (q22) translocation was identified through molecular cytogenetic studies in the tumor; q13), with the aim of reducing the tumor size and carrying out its complete resection, preserving the largest healthy tissue and thus allowing the anatomical functions of the patient to be preserved, following the recommendations provided in the NCCN treatment guidelines15. Next, surgical excision was performed, repairing and orienting the specimen, thereby allowing a complete evaluation of the deep and circumferential peripheral margins, the patient progressing satisfactorily after the second intervention.
By way of conclusion, dermatofibrosarcoma protuber ans in the vulva is an infrequent pathological condition affecting the adult female population locally devastating and with a tendency to local recurrence, therefore, it re quires a multidisciplinary approach for proper diagnosis. It requires a multidisciplinary approach to identify the right diagnosis and indicate individualized treatment, through highly effective surgical techniques and recognizing al terations in genetic checkpoints that can offer therapeutic options with less side effects when they are unresectable, recurrent or metastatic.

