











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Similars in
SciELO
Similars in
SciELO 
 Permalink
PermalinkLivedoid vasculopathy (LV) is a rare cutaneous disease that manifests mainly as recurrent leg ulcers. It is also called “atrophie blanche’’ because of its characteristic white scars formed after slowly healing ulcers1,2, LV sig nificantly impairs quality of life3.
LV is a non-inflammatory thrombus occlusive condi tion whose pathogenesis is unknown, associated with coagulation abnormalities or fibrinolysis. Hypoxia and hypercoagulability are the main pathogenic factors with the latter being the most predominant among them1.
Treatment for LV aims to improve skin lesions, al leviate pain and prevent recurrence of the disease. The treatment is controversial, with antithrombotic measures taking precedence over the others. The recurrent nature and controversial pathogenesis make this disorder a very challenging one to treat. Hyperbaric oxygen therapy (HBOT) was used effectively like adjuvant therapy in many cases, improving the healing process and diminishing pain and recurrences4.
HBOT delivers high oxygen concentrations to hy poxic tissue systemically and allows patients to breathe in 100% oxygen while in the pressurized cabin. It is a recognized modality for treating various complex wounds and non-healing ulcers due to various etiologies such as diabetic foot and chronic osteomyelitis4-7. The European Committee of Hyperbaric Medicine recommended treat ment at > 2 atmospheres absolute (ATA) for wounds and burns6,8.
However, the therapeutic benefits of HBOT, like angio genesis, collagen synthesis, anti-inflammatory effect, and bactericidal effect are performed at pressures neurologi cally as safe as under 2 ATA9-11.
High-pressure hyperbaric chambers (between 2 and 2.5 ATA), were used to treat several LV cases4,12-14.
We report a case of this pathology treated with a low-pressure hyperbaric oxygen treatment (lower than 2 ATA).
This case report suggests that low pressure hyperbaric oxygenation therapy is a quick and effective alternative for the treatment of livedoid vasculopathy that does not respond to conventional antiplatelet, immunomodulatory therapy or oral corticosteroids.
Clinical case
A 26-year-old female, non-smoker, presented with a 4 year and 8 months-old history of recurrent multiple non-healing ulcers involving feet and ankles. The wounds were associated with severe pain and inflammation. Examination also revealed evidence of previous ulceration in the form of multiple hyper-pigmented scars on both feet and ankles.
The patient had been undergoing treatment with 2.5 mg / kg azatriopine, 15 mg/day prednisone for 22 days, folic acid and acetylsalicylic acid for two years, which had good results during the first year, but presented poor evolution in the second. A biopsy was performed and the results obtained confirmed the diagnosis of livedoid vasculopathy, for which the treatment with azatriopine was suspended. Histological findings revealed the upper dermis with capillaries with fibrin deposition on their walls and fibrin thrombi with perivascular lymphocytic inflammation and erythrocyte extravasation.
Patient did not give any history of any medical illness. The blood platelets value was within normal parameters. Systemic vasculitis, antiphospholipid syndrome and systemic lupus erythematosus were ruled out. There were no comorbidities or associated pathology.
She reported multiple recurrences in the last year, with higher levels of pain and inflammation, and also the presence of a painful refractory ulcer of a one and a half year-old evolu tion, with dermatitis and small painful macules, papules with purpuric erythematous plaques with small superficial ulcers on both feet. She presented a history of recurrent dermatitis with small, painful ulcers and 4 very strong episodes lasting between 2 and 6 months before.
Hyperbaric oxygen therapy was indicated as adjuvant therapy with a session of 60 min ≈ 100%O2 at 1.45 ATA (Revitalair 430 by Biobarica chamber). The two first weeks the treatment was three times a week and the following weeks was twice a week.
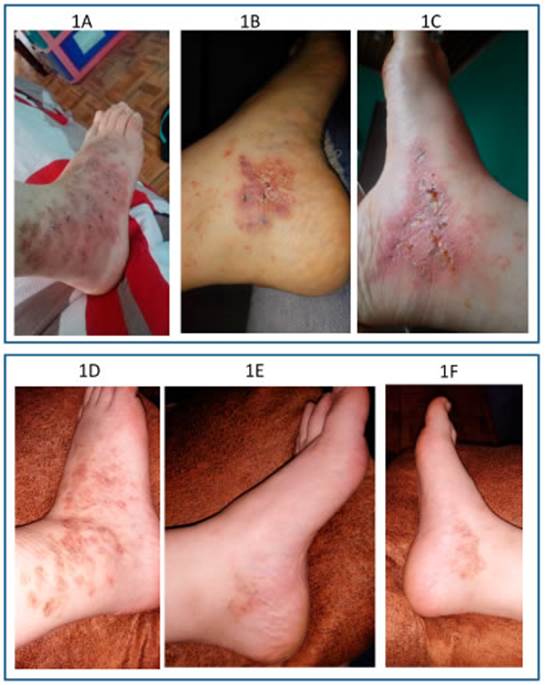
Complete healing and significant pain reduction was ob served after 12 sessions (Fig. 1). Follow-up was indicated to evaluate relapse-free time. The patient referred relief with a few sessions. She had complete healing of all ulcers, leav ing white polygonal scars with peripheral hyper-pigmented macules. New lesions ceased to develop and she had not recurrence for the following sixteen months.
Discussion
LV is the cutaneous manifestation of several diseases that lead to non-inflammatory thrombosis of dermal vessels. Reduced fibrinolytic activity in the blood of these patients, with reduced release of tissue plasminogen activator from vessel walls, leads to demonstrated increased aggrega tion activity1,2.
A variety of treatments with varying degrees of success have been used to treat LV. The efficacy of anticoagulants supports the main proposed pathogenic mechanism for LV of an occlusive vasculopathy. HBOT was described as treatment for LV in few cases, gener ally in combination with other drugs to be able to achieve remission4,12-14.
It has been shown that HBOT is able to increase the release of various fibrinolytic molecules from endothelial cells15,16. In vitro, in an ischaemia-reperfusion model using cultured endothelial cells, HBO stimulated the secretion of fibrinolytic factors including urokinase, plasminogen activator (t-PA) and plasminogen activator inhibitor type 1 (PAI-1)15.
Although clinical use of HBOT was defined at more than 1.4 ATA8, some authors suggest higher pressure hyperbaric for wound treatment7.
Actually, there is a rapid emergence of more acces sible, safer and portable hyperbaric chamber working at lower pressures17. Low pressure hyperbaric oxygen therapy is effective and proposed to neurological diseases but right now it is used in some refractory wounds17. Physiological benefits like angiogenesis, collagen synthesis and endothelial anti-inflammation are achieved at a pressure as safe as 1.45 ATA9-11. HBOT at 1.45 ATA generates a physical dissolution of oxygen in plasma and tissue fluids 10 times higher than that achieved by breathing room air at norm baric pressure17. Thus, HBOT uses hyperbaric chambers that work at 1. 45 ATA are effective in tissue oxygen ation. It creates a high oxygen gradient across the wound site and counteracts the damaging effect of tissue ischaemia6,17.
Authors had first used higher pressure HBOT for the management of LV with rapid healing of ulcers and sig nificant reduction in pain. As far as we are aware, this is the first report of low-pressure HBOT for LV treatment. We report pain relief with a few sessions and complete heal ing after 12 sessions of HBOT at 1.45 ATA. More studies and clinical cases series are necessary to demonstrate if low-pressure HBOT is effective for LV treatment and quality life improvement in these patients.

