English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Similars in
SciELO
Similars in
SciELO 
 Permalink
PermalinkKEY POINTS
Current knowledge
• Determinants of the clinical presentations of acute coro nary syndrome (ACS) as ST-segment elevation ACS (STEACS) or non-ST-segment elevation ACS (NSTEACS are not well stablished
• Patient´s risk profile and other clinical variables could influence the clinical presentation of ACS.
Contribution of the study
• Sex, active smoking, hypertension, dyslipidemia, age, prior myocardial infarction, chronic angina, comorbidities, and extension of coronary heart disease were associated with the clinical presentation of ACS.
• Our study confirms and define the influence of risk factors and clinical history on the pathophysiology and clinical presentation of ACS.
Coronary heart disease is the leading cause of global mortality and accounts for 50% of cardiovascular deaths1,2. Atherosclerotic plaque disruption with associated thrombo sis plays a key role in the pathogenesis of acute coronary syndromes (ACS)3-5. Clinical presentation of ACS will depend on the degree of acute coronary obstruction: if a total occlusion without distal coronary flow occurs, an ST-segment elevation ACS (STEACS) develops, and in the case of an incomplete obstruction with persistent distal flow, it manifests as a non-ST-segment elevation ACS (NSTEACS)3. Prothrombotic factors, local vasospastic re sponse, and coronary collateral circulation may influence the clinical presentation, and a subgroup of patients may develop ACS with non-atherosclerotic causes6-8. Some risk factors and other clinical variables may predispose to a certain cardiovascular event more than others. As an example, elevated plasma cholesterol is more related to ischemic heart disease than to stroke9,10; hyperten sion predisposes more to stroke than to ischemic heart disease11; and stroke is more associated with female sex than with the male sex, which is more related to ischemic heart disease12,13. Similarly, prior reports indicate that the patient´s risk profile and other clinical variables could influence the clinical presentation of ACS as STEACS or NSTEACS14-17. However, this evidence is weak because it is based on studies not designed for this purpose. To date, the independent association between risk factors and other clinical variables with the clinical presentation of ACS has not been defined. We hypothesize that risk factors and some clinical variables influence the clinical presentation of ACS. The aim of this study was thus to identify the risk factors and clinical variables that are associated with and influence the clinical presentation of ACS as STEACS or NSTEACS, describing the magnitude of this association and their interactions.
Materials and methods
All patients prospectively enrolled in the Epi-Cardio Registry from April 2006 to April 2018 with a diagnosis of ACS were included in the analysis, which was not pre-specified. Epi- Cardio is an observational, prospective, multicenter Argentine registry of patients with acute cardiovascular disease admitted to cardiovascular care units. Methods have been previously published18. Our study complies with the principles of the Declaration of Helsinki. Epi-Cardio registry has been approved by the Research Ethics Committee of the Argentine Society of Cardiology.
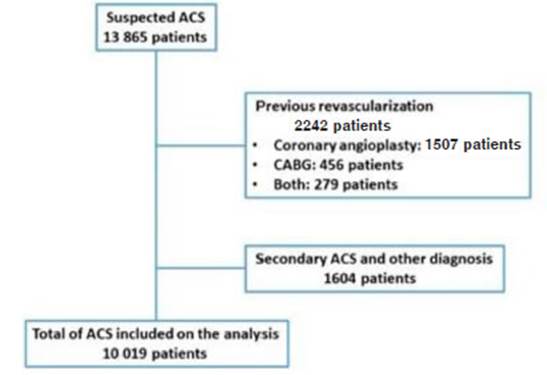
Inclusion criteria: age ≥18 years old, admitted for ACS or confirmed diagnosis during the hospital stay. Exclusion crite ria: patients with secondary causes of myocardial ischemia, such as severe anemia, active bleeding, sepsis, and tachyar rhythmia were excluded from the analysis. Patients with prior revascularization procedures (prior percutaneous transluminal coronary angioplasty or coronary artery bypass grafting) were excluded because they might develop ACS due to pathological mechanisms such as stent restenosis or thrombosis, or graft occlusion, which exceeded the objective of this study.
The diagnosis of myocardial infarction was made following the contemporary universal definition, and that of unstable angina according to specific clinical practice guidelines definitions6,7,19,20. The definitions accepted by scientific societies were used for risk factors and clinical variables. The clini cal presentation of ACS was determined according to the electrocardiogram performed on admission, which classified patients as STEACS or NSTEACS.ST-segment elevation was considered as new ST-elevation at the J-point in two contiguous leads with the following cut-off points: 0.2 mV in men or 0.15 mV in women in leads V2-V3 and/or 0.1 mV in other leads, according to the universal definition of myocar dial infarction6,7,20. Patients with presumed new left bundle branch block were classified as STEACS. Patients without ST-segment elevation criteria were considered as NSTEACS. Patients with myocardial infarction without ST-segment eleva tion but with a new Q wave (as the evolution of STEACS) were classified as STEACS.
We considered obstructive coronary heart disease when one or more epicardial coronary arteries had an obstruction ≥ 70% or ≥ 50% in the left main coronary artery.
Follow-up of the patients included in the Epi-Cardio Reg istry was limited to hospitalization.
Statistical methods
Continuous variables were described as median and interquar tile range and compared with the Kruskal Wallis test. Categori cal variables were described as percentages and compared using the x2 test.The x2 test for trend was used to evaluate the association between age by quintiles and clinical presentation of ACS. Univariate and multivariate associations between age, sex, hypertension, smoking, dyslipidemia, diabetes, extension of coronary heart disease, prior myocardial infarction, chronic angina, prior heart failure, major comorbidities (chronic kidney disease, chronic obstructive pulmonary disease and prior stroke) and clinical presentation of ACS were evaluated. The selection of the analyzed variables was based on previous reports from the medical literature. Logistic regression mod els were performed to define independent associations and to detect potential confounders. A stratified analysis and an interaction test were used to assess effect modifiers, as ap plicable. The area under the ROC curve (AUC) was used to assess discrimination, and calibration was evaluated with the Hosmer-Lemeshow goodness-of-fit test. Extension of coronary heart disease was quantified according to the number of coronary arteries with obstructive disease. It was included in the multivariate analysis as a continuous variable (1, 2, or 3 vessels). Left main coronary artery obstruction was quantified as 2 vessel-disease.
Due to the exploratory nature of the analysis, a prospec tive sample size calculation was not performed. However, 10 000 patients were considered a sufficient number to evaluate the proposed associations, even in smaller subpopulations.
All tests were two-tailed and α ≤ 0.05 was considered sig nificant. The analysis was restricted to patients with complete data, as only 0.2% of patients had missing data for clinical variables and the cardiac catheterization report was complete in more than 96% of patients. Data analysis was performed usingSTATA® 13.0 and Epi-Info® 7.2.4.0.
Results
A total of 64 health institutions enrolled 13 685 patients with ACS in the Epi-Cardio registry from April 2006 to April 2018. The final analysis included 10 019 patients (Fig. 1). Table 1 shows baseline characteristics of the total popula tion and stratified by ACS clinical presentation.

Univariate associations between risk factors, clini cal variables, and clinical presentation as STEACS are shown in Table 1. After multivariate analysis, male sex and smoking were positively associated with STEACS. Hypertension, dyslipidemia, age, prior myocardial infarction, chronic angina, and comorbidi ties were negatively associated with STEACS (Table 2). The AUC was 0.66, and the Hosmer-Lemeshow test p = 0.58.

Table 2 Multivariate association between clinical variables and risk factors with STEACS in total population, men and women
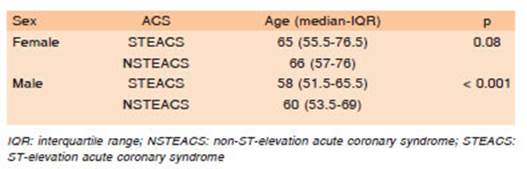
Among men, patients with NSTEACS were older than those with STEACS, but there was no association be tween age and the clinical presentation of ACS in women (Table 3).
Age presented the following distribution: firs quintile, < 51 years old; second quintile, 51 to 57 years old; third quintile, 58 to 63 years old; fourth quintile, 64 to 72 years old; fifth quintile, ≥ 72 years old. Figure 2-A shows the proportion of STEACS by age quintiles, stratified by sex. In both sexes, the proportion of STEACS decreased with age; however, among women, the association was less progressive and less strong (x2 for trend in men and women, p < 0.0001 and p = 0.02, respectively).

Fig. 2 Clinical presentation as STEACS according to age quintile, stratified by sex. A: Total population. B: Patients with severe coronary heart disease
Multivariate analysis stratified by sex is shown in Table 2. Models were built with the same variables and associations were similar, except for age. Older age was associated with NSTEACS in men. In women, there was no independent association between age and clinical presentation (p for interaction = 0.01). The AUC was 0.64 in men and 0.65 in women, with Hosmer-Lemeshow test p > 0.05 in both models.
Cardiac catheterization was performed in 6210 patients (62% in the total population, 67.7% in STEACS and 56.4% in NSTEACS; OR 1.62; p < 0.001) and a total of 5970 cases (96.1%) had a complete report. The extension of coronary heart disease and its association with the clinical presentation of ACS is shown in Figure 3 and Figure 4. Among patients with obstructive coronary heart disease, a greater extension of coronary heart disease was as sociated with a lower presentation of STEACS (OR 0.84; 95% CI 0.78 to 0.91; p < 0.0001). After the extension of coronary heart disease was included in the model, sex did not show an association with the clinical presentation (OR 1.13; 95% CI 0.98 to 1.3; p = 0.09 for men). The AUC was 0.65, and the Hosmer-Lemeshow test p = 0.72.

Fig. 3 Association between the number of coronary arteries with obstructive coronary heart disease and clinical presentation of ACS
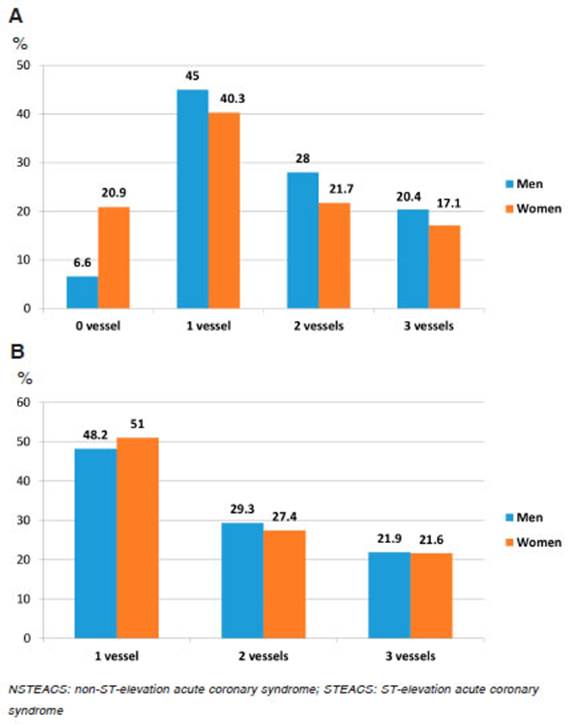
Fig. 4 Extension of coronary heart disease in both sexes. A: Patients with cardiac catheterization. B: Patients with obstructive coronary heart disease
In the total population, men presented a greater exten sion of coronary atherosclerotic disease than women (Fig. 4-A), but after the patients with non-obstructive coronary arteries were excluded, the differences were minimized and the extension of coronary heart disease was very similar in both sexes (Fig. 4-B), as well as the clinical presentation of ACS in all age quintiles (Fig. 2-B).
Multivariate analysis showed that male sex, diabetes, smoking, prior myocardial infarction, and STEACS were associated with obstructive coronary heart disease, and female sex and hypertension were associated with non-obstructive coronary arteries (Table 4).

Table 4 Multivariate association between clinical variables, risk factors and severe coronary heart disease
The multivariate analysis repeated using a cut-off value of ≥ 50% obstruction, according to the current MINOCA (myocardial infarction and non-obstructive coronary arteries) definition21, showed similar associations (data not shown).
Discussion
The population of our study represents a broad spectrum of ACS, with baseline characteristics similar to those of series of patients with ACS in the real world14,16,17. Our results show a proportion of STEACS higher than in other studies, due to the exclusion of patients with secondary ACS or previous revascularization procedures. After the excluded patients were added to the analysis, the propor tion of STEACS and NSTEACS was 42.9% and 57.1% respectively.
The statistical associations and regression models developed in our study confirmed our hypothesis: the clini cal presentation of ACS is influenced by the patient’s risk profile and other clinical variables. The p values confirm strong statistical associations, with a negligible probability of incurring in a type I error.
Smoking had the greatest positive association with STEACS, and our results confirm a solid and independent association. The prothrombotic effect of smoking appears to contribute to the pathophysiological mechanism3,5,22.
Previous studies showed a relationship between younger age and STEACS, and older age and NSTEACS, but did not evaluate the multivariate association in both sexes14-16,23. Our results confirm a strong association in men, with an increase in the proportion of NSTEACS associated with advanced age. Among women, there was no independent association between age and the clinical presentation of ACS due to a higher proportion of NSTEACS among younger women.
In our population, diabetes was more common in pa tients with NSTEACS than among those with STEACS. However, the multivariate analysis did not show an inde pendent association. Diabetes is related to older age, dys lipidemia, hypertension, and prior myocardial infarction, all associated with NSTEACS. These variables could be confounding factors in the association between diabetes and the clinical presentation of ACS. Based on our find ings, we can conclude that diabetes is not independently associated with the clinical presentation of ACS, a result that had not been previously defined in other studies.
We reported a higher prevalence of hypertension and dyslipidemia among patients with NSTEACS compared with STEACS. The multivariate analysis confirmed both independent associations.
In our study, a history of myocardial infarction was as sociated with NSTEACS independently of other variables, which means that the probability of presenting STEACS is greater in the first ACS than in the next coronary event.
Chronic angina was the variable most strongly as sociated with the clinical presentation as NSTEACS. Usually, this symptom is related to older age, female sex, and diabetes. Our results confirm that chronic angina is independently associated with NSTEACS.
Major comorbidities are normally related to older age, history of myocardial infarction, extensive coronary heart disease, and NSTEACS17,24,25. In our study, comorbidities maintained an independent association with the clinical presentation as NSTEACS after the multivariate analysis.
Including the extension of coronary heart disease in our analysis was very important to understand some as sociations, and to unmask others. Logically, older age is related to a greater extension of coronary heart disease. Both variables are associated with a higher proportion of fibrotic and calcified lesions and with a lower proportion of lipid-rich lesions, as shown in pathological and invasive coronary imaging studies26-30. These findings are char acteristic of NSTEACS. Among patients with ACS and obstructive coronary heart disease, a greater extension of coronary heart disease was associated with the clinical presentation as NSTEACS. A finding of great importance emerges from this analysis: after coronary heart disease extension was included in the multivariate analysis, sex lost statistical association with the clinical presentation of ACS because women had less extension of coronary heart disease than men due to a more frequent occurrence of ACS without obstructive coronary lesions (20.9% vs. 6.6%) (Fig. 4-A). When selecting patients with obstructive coronary heart disease, its extension, and the clinical presentation stratified by age quintile were very similar in men and women (Fig. 4-B and Fig. 2-B), and sex lost an independent association with the clinical presentation. Therefore, in the presence of obstructive coronary heart disease, the association between risk factors and clinical variables with the clinical presentation of ACS was similar in both sexes. It seems that the main difference between sexes is that the pathophysiological mechanisms related to ACS with non-obstructive coronary arteries develop more frequently among women. Younger age, female sex, hypertension, and clinical presentation as NSTEACS were associated with ACS with non-obstructive coronary arteries.
The statistical models developed in this study confirm our hypothesis. However, the discriminative capacity of the models was low or moderate, which means that risk factors and clinical variables were associated with the clinical presentation of ACS, but they were not the only determinants. The magnitude of the associations was low to moderate since the ORs were mostly between 0.4 and 2.
The heterogeneity of ACS “subtypes” added to the overlap between risk factors and clinical variables makes it difficult to develop a unique association model with high discriminative capacity.
Our study has some limitations. We must mention the lack of survey of some variables, as family history of coronary heart disease and the use of illicit drugs such as cocaine, which can influence the pathophysiology and clinical presentation of ACS. Neither were socioeconomic and psychosocial risk factors surveyed.
The main analysis was based on statistical asso ciations between risk factors and some clinical variables with electrocardiographic findings that define clinical syndromes. Although the clinical-pathophysiological and clinical-pathological correlations described are supported by previous studies, we did not use Optical Coherence Tomography, Intravascular Ultrasound or pathological studies to corroborate them in our population.
The results of our study do not allow us to define whether the inability to develop statistical models with high discriminative capacity was due to the lack of survey of some variables or to a random component in the clinical presentation of ACS.
Previous studies have shown a univariate association between some risk factors and clinical variables with the clinical presentation of ACS. However, these studies did not evaluate the independent association between each variable and the clinical presentation of ACS. Defining the independent association between each variable and the clinical presentation as STEACS or NSTEACS in a large ACS population was the main strength of our study. The inclusion of a large and heterogeneous ACS population, with broad inclusion criteria, supports the generalizability of the findings.
Our study, based on a real-world population of 10 000 ACS, shows that some cardiovascular risk factors and other clinical variables are independently associated with the clinical presentation of ACS as STEACS or NSTEACS. These findings confirm the influence of risk factors and clinical history on the clinical presentation of ACS.