











 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Similars in
SciELO
Similars in
SciELO 
 Permalink
PermalinkKEY POINTS
• The chronic regional pain syndrome (CRPS) is a painful chronic disorder usually affecting the limbs after trauma or surgery. Its clinical presentation is heterogeneous. It is diagnosed by clinical criteria, while imaging tests help to identify the pathology and to differentiate it from other conditions. There is no treatment of choice, and the use of bisphosphonates has not been deeply studied but it has shown good results.
• This study revealed that DXA scans as a diagnostic tool for CRPS have sensitivity to detect and to objectivize the changes provoked by the syndrome in the affected limb and, also, post-treatment. The treatment with IV bisphosphonates (pamidronate, ibandronate and zolendronate) was efficient and with few adverse events.
Chronic regional pain syndrome (CRPS), also known as Sudeck syndrome, has been one of the most enigmatic medical pathologies since it was first described 150 years ago. Its name has undergone several changes over the years and more than 200 names, in different languages, have been identified for this syndrome1. The International Association for the Study of Pain (IASP) defines it as a chronic painful condition, characterized by spontaneous and evoked re gional pain, which usually starts in a distal limb and which is disproportionate in magnitude and duration to the typical course of pain after a similar tissue trauma2. In 1994, the IASP coined the name CRPS, with 2 subtypes, I and II, which share identical clinical features the only differ ence being the presence of a lesion in the pe ripheral nerve in type II. In a consensus meeting of the IASP which took place in Budapest in 2003, new clinical diagnostic criteria were proposed, which have been since known as “the Budapest Criteria”3. In 2007, due to a tendency towards overdiagnosis, the Budapest criteria were modi fied to include at least one symptom in 3 of the 4 categories, and the display of at least one sign found in the physical exploration in 2 or more of the considered categories4 (Table 1). By doing so, they retained a high sensitivity for CRPS (90%), but they improved its specificity enormously (69%). Imaging techniques such as Tc-99 bone scintigraphy and magnetic resonance imaging (MRI) are useful to make differential diagnosis with other pathologies and to confirm bone involvement5.
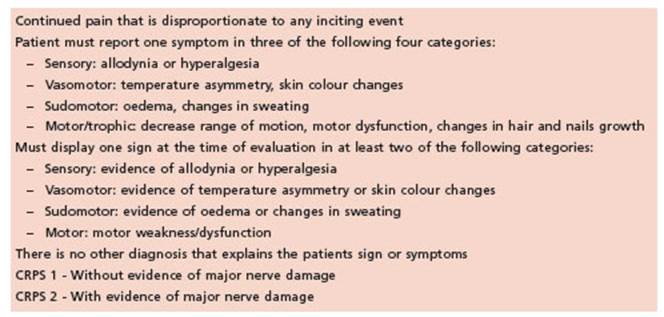
Table 1 The International Association for the Study of Pain criteria for complex regional pain syndrome5
The condition presents itself with chronic pain usually affecting only one limb, togeth er with a combination of distinctive signs and symptoms6. The main feature is pain, some times disabling, accompanied by a series of sen sory, motor, autonomic, skin and/or bone disor ders. The patient presents with different degrees of pain, allodynia, hyperalgesia, oedema and changes in skin color and temperature. Regional osteopenia, changes in hair and nail growth, and skin dystrophy can also be found1.
CRPS has a high impact on the person´s life, and it represents a high economic burden for health systems. However, it still does not have a categorically effective treatment, probably because its physiopathology is not fully un derstood. Bisphosphonates (BP) are often used, but data on their efficiency and dosage are still scarce in the literature.
The objectives of this paper were to describe the features in a series of patients with diag nosis of CRPS in lower limbs followed up in our institution; to examine the inciting events; to evaluate the imaging methods used for their as sessment, especially dual energy X-ray absorp tiometry (DXA), and to analyze the results of treatment with BP.
Materials and methods
We carried out a retrospective, descriptive, observa tional cross-sectional study of 54 health records of ambu latory patients who had been evaluated in a bone clinic in Buenos Aires, Argentina.
We selected all the patients who had a diagnosis of “Sudeck” in their electronic health records between June 2013 and September 2017.
In a database, we recorded their demographic features (sex and age); inciting events; site of the lesion, results of imaging tests (radiographic images, Tc-99 bone scintigra phy, MRI and DXA), prescribed treatment (drugs and ad verse events) and evolution (time of recovery and return to daily activities).
Bone mineral density (BMD) and bone mineral content (BMC) measurement:
BMD (g/cm2) and BMC (g) were measured by Lunar Prodigy DXA (GE Healthcare, Madison, WI, USA). We con sidered two regions of interest (ROIs) in the site of the le sion and two in the symmetric contralateral site (of equal surface area). We calculated the mean values of the BMD and the BMC of both the affected and the healthy limb (± standard deviation) and the difference between them. The results were expressed as mean ± SD (standard de viation). The comparison between groups was made us ing the Student’s t-test. A p value of <0.05 was considered statistically significant.
Results
The search for the term “Sudeck” as a diagno sis resulted in 77 patients, with a final cohort of 60 as 17 were excluded for lack of data and /or diagnostic mistakes. The diagnosis was primar ily performed based on clinical findings with the support of imaging tests. Out of the 60 patients, 6 had upper limb involvement and were excluded.
Demographic characteristics and inciting events
The average age was 55 ± 13 years (range 24-85 years of age) and 74% were females.
Trauma was the most frequent inciting event (n = 32, 59% of the cases), especially when ac companied by fractures. Falls were the main cause of trauma, whereas strains, sprains and bumps followed in frequency. Other inciting events were programmed surgeries, mainly hal lux valgus. Intense workout and immobilization were considered inciting events in a lesser pro portion of patients, and no apparent cause was found in 5 cases.
The most common symptom was pain, which was present in 50 patients. Among the descrip tive features, patients mentioned allodynia both while resting and walking, exacerbated when resting. Oedema was described in 35 pa tients. Seventeen patients presented with ery thema, and 15 patients described an increase in skin temperature, whereas one patient showed just the opposite sign. One patient presented changes in sweating and another, less growth of nails and body hair.
Complementary tests: X-rays showed decalci fication or loss of bone structure (characteristic findings of CRPS) in 87% of the patients. In 100%, Tc-99 bone scintigraphy was described as a hy per-capture pattern compatible with CRPS. MRI described oedema and bone involvement as the main findings in 87% of the cases.
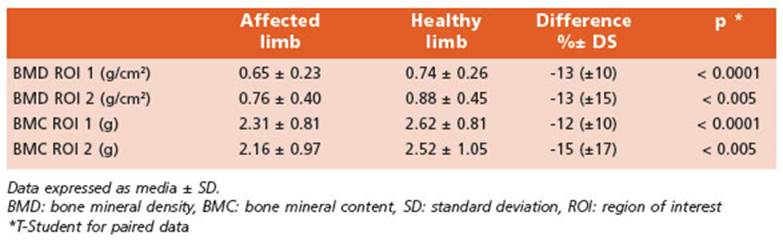
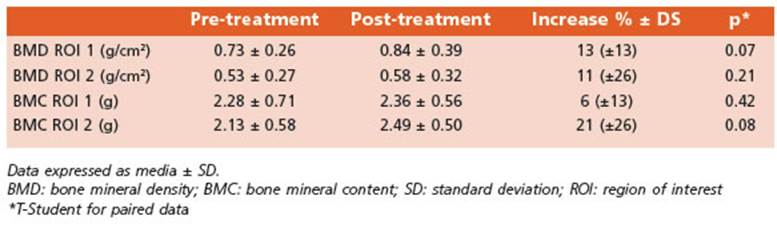
Bone mineral densitometry tests were per formed in 23 patients. All the averages (BMD of ROI 1 and 2, BMC ROI 1 and 2) of the affected side were lower (from 12% to 15%) than those of the healthy side, with statistically significant differences (Table 2). Individually, 21 of the cas es showed 1 or the 2 ROIs with lower BMD and BMC in the affected side as compared with the healthy side. In 9 patients, we also performed a post-treatment control. The time elapsed be tween the two studies was 10 ± 5 (range 4-18) months. The comparison of the affected limb before and after the treatment showed an im provement both in the BMD and in the BMC, although the differences were not statistically significant. The average increases ranged from 6 to 21% (Table 3).
Treatment with bisphosphonates
A total of 44 patients received BPs. Ibandro nate was the most widely used (n = 19) both orally (monthly) and intravenously; in 7 pa tients it was used more than once (maximum 5 infusions). The second most used drug was zoledronic acid (n = 15) and none of the patients repeated the treatment. Pamidronate was used in 10 patients, of which 5 had a particular regi men: 30- 60 - 90 mg (once a week) and the rest received an irregular dosage, sometimes 30 or 60 mg. Only 2 patients were treated with 2 dif ferent BPs: one received pamidronate and an other one ibandronate in the first instance and both received zoledronic acid later.
As regards BPs adverse events, 6 patients (14%) experienced pseudoflu syndrome and acute phase symptoms (3 had received zole dronic acid, 2 ibandronate and 1 pamidronate with the 30-60-90 mg regimen).
An improvement in symptoms, mainly pain intensity, was reported in 75% of patients. The individual analysis of each BP used showed that the best response, considering the percentage of patients whose symptoms improved and re turned to their daily activities, was obtained with ibandronate (16 out of 19 patients). All the patients who reported improvement did so with in the first six months post treatment; two who received zoledronic acid and two who received intravenous ibandronate described improve ment in their symptoms a week after treatment.
Discussion
In this paper we describe the experience of the management of 54 patients with CRPS in lower limbs who were treated in an institution special ized in osteology. The epidemiological charac teristics of our cohort, the female predominance and the average age (55 years) coincide with the data published in the literature7. Other authors found a male predominance, suggesting it might be due to men’s higher disposition to trauma8. As regards age, some series described a higher prevalence of CRPS in older people, related to the higher rate of injuries and fractures associ ated with this age group7. A higher risk has also been described in post- menopausal women, suggesting that hormonal factors might be in volved in the pathogenesis of CRPS9.
In our cohort, trauma was found to be the main inciting event for CRPS as described in many series7,8,10-12. Among trauma, fractures car ry more risk of developing CRPS as the presence of fracture is usually related to more severe in juries, extensive destruction of tissue, the need for surgery in many cases, and a higher rate of medical complications11. There are some other conditions associated to fractures that might in crease the risk, such as the need for reduction on a displaced fracture, the pressure of the cast used to immobilize it, the type of anesthesia used (local vs general), inappropriate physio therapy10 and intra-articular involvement of the fracture9. Despite discrepancies, most authors believe that the higher the severity, the greater the risk13.
Though it varies in different series, there is, in most cases, a predominant involvement of the upper limbs7,8. However, in our initial cohort, 90% of the patients showed involvement of the lower limbs, which is probably due to an institu tional bias as 85% of the referring physicians, are traumatologists who specialize in foot patholo gies. In this context, which differs from what is described in the literature; only those patients with lower limb involvement were analyzed and described in this study.
Programmed surgeries were the second cause of CRPS, in agreement with the literature data14, with a higher prevalence of Hallux Valgus15.
Complementary imaging tests are used to study CRPS and they are mainly useful to make a differential diagnosis with other chronic pain syndromes16. DXA scans of feet carried out in our center showed that in healthy patients there is no difference in BMD or BMC between both feet17. DXA results coincide with those de scribed in the literature18 where some authors report even greater differences between both limbs. Some of our patients showed a mini mal difference between the affected and the healthy limb, sometimes only evident in a ROI, which might be explained by the patched and heterogeneous bone resorption pattern and is usually present in CRPS14. In the study of Br uscas Izu et al., this pattern was especially associated to hand/wrist and foot/ankle lesions8. Moreover, it has been reported that immobili zation and lack of use lead to bone loss of both the affected limb and the contralateral one, which decreases the sensitivity of the method to detect changes. Kumar et al. studied patients suffering from post-stroke CRPS in which the BMD loss was correlated with duration of immobilization, severity of pain and autonomic involvement of the affected limb20.
DXA was also sensitive to the increase in bone content related to treatment. Arriagada et al. describe the post- treatment results of 8 patients treated with prednisone or calcitonin, identifying an increase of 20% in the DXA of the affected limbs18. Chapurlat et al., in a longitudi nal study of CRPS patients, state that in those patients treated with pamidronate in an early stage, the DXA remained stable, preventing bone loss21. Our results reaffirm the assertion of the importance of DXA scans in the study of CRPS22. It is a simple, non-invasive method that involves minimum radiation and preparation that gives a quantitative measurement of the bone content and density.
Bisphosphonates have traditionally been the most studied drugs for the treatment of CRPS23 and they should be considered the treatment of choice for patients with this diagnosis24. A marked loss of bone (positive uptake on scintig raphy, demineralization on X-ray, bone oedema on MRI and loss of mineral density on DXA) along with the analgesic effect shown in several bone pathologies25, are the reasons that justify their use in CRPS type I26. However, the increase in osteoclast activity has never been well dem onstrated in this pathology, which raises ques tions about the way bisphosphonates work in this syndrome27. A potential mechanism of pain in CRPS might be the activation of two main groups of acid-sensing nociceptors (TRPV1 and ASICs), due to local acidosis secondary to the hypoxemia produced by microvascular altera tions. BPs might act on this pathway as they decrease the proton concentration in the bone microenvironment. They also inhibit the growth, migration and activity of the mononuclear cells derived from the bone marrow28 with a reduced release of neuropeptides such as substance P and the calcitonin gene-related peptide26. Both in vitro and in vivo, they reduce the expression of TNF and of cytokines such as IL 1 and 629, and their effect on other cells such as macrophages and microglia has been demonstrated, includ ing those cells that release pro-pain substances such as nerve growth factor β. This mechanism via microglia, along with the inhibition of neurotransmitter release, might explain an addi tional analgesic effect of BPs at base level30,31. In conclusion, the potential beneficial effects of BPs in the treatment of CRPS are not related to their traditional antiresorptive activity, but to a much more complex interaction32.
In the literature, only five randomized, pla cebo controlled and well-designed studies eval uated the results of the use of oral33 and IV34 alendronate, clodronate35, pamidronate36 and neridronate27 in CRPS. They all showed reduction of pain and improvement of functionality of the affected limb - especially with alendro nate34,36 - and of oedema35. Other benefits described were improvement of vitality, of men tal state (feeling good) and of other indicators of quality of life27. The time elapsed before the improvement of symptoms was very variable, but an improvement in pain, oedema and mo bility could be observed as early as two weeks after starting treatment with IV alendronate34. Evidence shows that the antinociceptive effect of BPs on bone is dosage dependent37, therefore, some authors suggest using higher doses than those recommended for Paget disease and ad vise a regimen of 4 doses of 90 mg administered over 4 to 10 days27.
There are very few studies that analyze the efficiency of ibandronate and zoledronic acid. A study of 10 patients with CRPS38, used high doses of ibandronate (infusions of 6 mg /day for three consecutive days) and found a significant post-surgery improvement in the control of pain and in some features of neuropathic pain (sensitivity, depth, intensity) as well as in hyperalgesia and allodynia. The use of ibandronate 3 mg IV was also associated with improvement in pain and clinical signs39. As regards the use of zole dronic acid, Ahmad et al40 described the case of a patient with CRPS who was treated with zoledronic acid, after the failure of NSAIDs, cor ticoids and physiotherapy. The patient received 2 doses of 4 mg IV, separated by one month, showing improvement in pain, oedema and in the DXA scan, with partial functional recovery. A recent study published by Walfish et al.41 de scribes the case of 16 children and adolescents with CRPS treated with ibandronate and zole dronic acid who had recurrence or no response to conventional treatment. Nine of the 16 pa tients reported significant improvements in the score of the global impression of change (84% or more), 8 to 21 months after the last BP infusion. There was also a significant decrease in pain in tensity and in the need for analgesics. The num ber of patients with minimum or no disability increased, and almost all the patients resumed their school activities.
As regards adverse events associated with treat ment with BPs, we found 14% in our series, where as large series showed percentages as low as 5% (with oral alendronate)33 up to 50% (with IV pami dronate)36. In brief, the role of BPs in the treatment of CRPS is not very clear yet, and the published data are scarce. The proper dosages, along with the administration intervals have not been fully clari fied, but our results are encouraging due both to the reported efficacy and the speed of response.
This study has several limitations: 1) the population was heterogeneous and its evalua tion was carried out by different physicians, of varied specialties, therefore the study criteria, diagnosis and treatment were different; 2) as it usually happens with retrospective studies, the data and the results are limited to the in formation available; and 3) the population under study comes from an institution that specializes in osteology, which, is probably associated with an attention and population bias and 4) the pub lished results are those of patients with lower limb involvement. We do not know if they can be extrapolated to upper limbs or other variants of this syndrome.
On the other hand, it has several strengths: 1) its sample size, as we analyzed 54 patients suf fering from a syndrome that is considered rare; 2) the interesting results obtained using DXA scans, which open the way to a promising field in the study of this pathology and 3) the impor tant conclusions we could draw from the use of BPs for the treatment of this pathology, which turned out to be efficient and safe.
In conclusion, this research reflects the ex perience of a centre specialized in bone health regarding the study and treatment of this rare syndrome. Although our review has the above-mentioned limitations, it provides un published data that might open new lines of research in the future. The use of DXA in these cases offers a new perspective regarding bone involvement in this syndrome. Finally, the use of bisphosphonates for its treatment is very promising, and deserves to be evaluated in prospective studies involving a higher number of patients.

