











 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Similars in
SciELO
Similars in
SciELO 
 Permalink
PermalinkCardiac tumors are rare, with an incidence of 0.002%. They may originate from the pericardium or myocardium, and are primary or secondary, the latter being 20 times more common. 1
Primary cardiac neoplasms are infrequent, representing 0.25%. Most of them (75%) are benign and include myxomas, rhabdomyomas, fibromas, and lipomas. 2
Cardiac myxomas represent the most common benign cardiac tumor. They are found in the left atrium (75%), right atrium (20%), or ventricles (5%). Clinically, myxomas may occur in asymptomatic individuals and are detected incidentally, or may cause symptoms usually related to its mobility, size, and location within the heart. In general, the symptomatic triad includes systemic (fever, weight loss, fatigue) or cardiac symptoms (arrhythmias, mitral or tricuspid regurgitation due to interference with valve coaptation, pericarditis, dyspnea, syncope), and pulmonary and/ or systemic embolic phenomena. 2 While these are the most common manifestations, unusual forms of presentation have also been described.
Doppler echocardiography is the method of choice to diagnose and determine its characteristics and hemodynamic impact.
The clinical case of a left atrial myxoma with an unusual presentation is described below.
We report the case of a dyslipidemic, ex-smoker 61-year-old woman with no cardiovascular history, consulting for a several-month history of sacroiliac arthralgia; laboratory tests revealed elevated erythrocyte sedimentation rate (84 mm/h) and C-reactive protein (6.2 mg/L), and no other abnormalities.
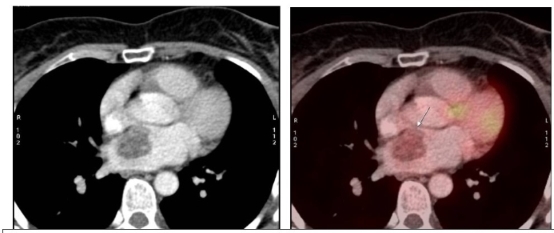
After evaluation by the Rheumatology Department, diagnosis was inflammatory spondyloarthropathy with persistently elevated inflammatory markers not meeting the criteria for rheumatic disease; the positron emission tomography (PET) scan revealed a single tumor in the left atrium (Figure 1).
Doppler echocardiography showed a rounded, heterogeneous, sessile left atrial mass attached to the interatrial septum, with wide anarchic movement, and in non-invasive contact with the right upper pulmonary vein. This mass did not interfere with the opening and closing of the mitral valve (Figure 2).
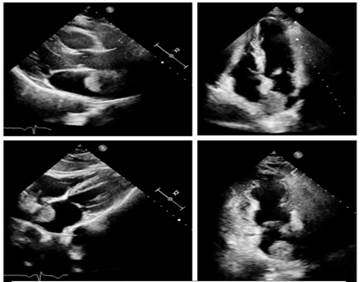
Fig. 2 Doppler echocardiography views showing a rounded, heterogeneous, left atrial mass attached to the interatrial septum.
CT scan revealed a 30 x 22 mm heterogeneous left atrial mass attached to the interatrial septum, with regular borders, enhanced after intravenous contrast injection, and no evidence of invasion of the pulmonary veins. The result was interpreted as a possible atrial myxoma, and surgical resection was performed using a transseptal approach; a 5 cm tumor was resected without complications, and a biopsy was sent to Pathology.
Results revealed proliferation of perivascular spindle cells without atypia, in streaks and in a lax stroma, with signs of old and recent hemorrhage, scant fibrous tissue and myocytes, consistent with myxoma.
After surgical resection, follow-up showed improvement of joint symptoms until their disappearance and normalization of inflammatory markers.
Myxomas are the most common benign cardiac tumors, usually found in older women, 2 as was the case described here.
They are most commonly found in the left atrium (75%), as a sessile or pedunculated intracavitary mass, attached by a stalk to the interatrial septum.
Clinical manifestations are related to their cardiac location, size, and mobility. The most common symptomatic triad includes intracardiac obstruction, embolism, and systemic symptoms.
According to a French series of 112 cases, heart failure secondary to mitral valve obstruction was present in 67% of the patients, followed by cerebral emboli in 29%, and 34% with general symptoms such as fever, weight loss or symptoms resembling connective tissue disease. 3
Intracardiac obstruction often occurs in pedunculated left atrial myxoma protruding to the left ventricle and causing mitral valve coaptation deficit and subsequent regurgitation. While uncommon, myxomas found in the right atrium may protrude into the tricuspid valve and cause regurgitation. In both cases, they can occur with heart failure or syncope. 3
Emboli are more common in papillary myxomas, as they are less solid and become more fragile with anarchic movement. The site of the emboli depends on the location of the tumor. Left atrial myxomas have the potential for embolism to the central nervous system, resulting in stroke or amaurosis. The involvement of coronary, renal or lower limb arteries is uncommon. 4
Constitutional symptoms may appear as connective tissue disorders, with poor general condition, weight loss, anorexia, and fever. These symptoms are more common in women than in men, and in right atrial myxomas. 4
It is believed that extracardiac manifestations are often caused by embolic phenomena and inflammation due to the intrinsic secretion of cytokines. 5 Polymyalgia rheumatica -the manifestation that motivated our patient's consultation- is uncommon. Polymyalgia rheumatica is characterized by pain in the proximal muscles and increased serum levels of inflammatory markers. It is also one of the most common diseases in young adults and affects women more frequently than men (ratio 3:1). 6
Doppler echocardiography is essential for the diagnosis of myxomas, and to define location, size, and complications. Both cardiac magnetic resonance imaging and cardiac multislice computed tomography provide additional information for decision making.
Myxoma needs surgical excision to reduce the risk of embolization. While the rate of recurrence is low, follow-up Doppler echocardiography is recommended. 4 In the case reported, our patient debuted with rheumatologic manifestations with persistently elevated inflammatory markers; left atrial myxoma was incidentally found after several diagnostic tests.
Undoubtedly, myxoma remains a challenging entity to diagnose. The fact that they are typically asymptomatic or present with nonspecific symptoms makes it a non-suspected entity, mostly diagnosed incidentally. It is vital to be aware of the possible cardiovascular and systemic manifestations to suspect, diagnose and treat myxomas in a timely manner.

