











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Similars in
SciELO
Similars in
SciELO 
 Permalink
PermalinkIntroduction
Chronic obstructive pulmonary disease (COPD) is the fourth leading cause of mortality throughout the world. It is estimated that it affects more than 5 percent of the world population1, and 8-10% people older than 40 years2-4. However, despite the fact of being a very common and well-known disease in the medical practice, it is highly underdiagnosed. The reason for this underdiagnosis is that patients do not attend their consultation because they have become used to the symptoms or they don’t know for sure if COPD can be treated. Also, the spirometry isn’t easily interpreted by some medical care providers and sometimes COPD is mistaken for asthma, because both conditions may show fixed airflow obstruction5-7.
One of the questionnaires to be used was the Chronic Obstructive Pulmonary Disease Population Screener (COPD-PS)5. It consists of five items: three items related to symptoms (dyspnea, produc tive cough and activity limitation), a fourth item related to smoking history (100 or more cigarettes smoked throughout the patient’s life) and the last item associated with age. It has a maximum score of 10 points10. In its initial validation study done in the United States in 2008, with a cut-off point ≥ 5, it showed 84.4% sensitivity and 60.7% specificity. Then it was validated in 2021 and 2014 in Spain and Japan with a cut-off point of 4, and obtained the following results: 93.6% sensitivity and 64.8% specificity in the Iberian country.
In Colombia, COPD is a prevalent disease, where the medical record or the use of screening question naires may be useful for searching patients with this disease4,15,16; however, in order to use screening instruments, it is necessary first to conduct validation studies ideally in the populations where they are intended to be used. In the country there is lack of data about the diagnostic performance of specific questionnaires such as the COPD-PS. The objective of this study is to determine the reproducibility and validation of the COPD-PS questionnaire in a Colombian population.
Methodology
We carried out a prospective cohort with the objective of determining the reproducibility and valida tion of the COPD-PS questionnaire in a Colombian population. The participants attended an external consultation at the Clínica Universidad de la Sabana, Chía, Colombia. Patients were enrolled between 2015-2020.
Population
Individuals older than 40 years who were asked to undergo a spirometry to be performed in the lung function laboratory of a third level clinic, regardless of their indication. Individuals needed to have enough time available for this study and had to give their consent to answer a lung function question naire. We excluded subjects whose spirometry didn’t fulfill the acceptability or reproducibility criteria of the American Thoracic Society (ATS) guidelines, or subjects with some kind of limitation on their communication that would complicate the development of clinical questionnaires. The spirometry was performed by the duly qualified and trained staff of the lung function laboratory, with previously cali brated equipment. COPD was defined as the presence of fixed airflow obstruction with a FEV1/FVC ratio of less than 0.7 after the administration of the bronchodilator, according to the ATS definition, and with a smoking history of more than 10 packs per year.
Study variables and data gathering
Data gathering included a first visit to obtain demographic information: age, sex, race, weight, height, level of education, respiratory symptoms, history of exposure to tobacco smoke, wood smoke or other occupational exposure to smoke, history of medical diagnosis of COPD or asthma (confirmed or not confirmed) and lung function values. The COPD-PS questionnaire was applied at the end of the spi rometry and subsequently during a second visit with a minimum difference of 15 days between them, where the questionnaire was repeated for the reproducibility analysis.
COPD-PS questionnaire
The Spanish version of the COPD-PS questionnaire consists of the following 5 questions: 1. For the past 4 weeks, how many times did you feel breathless? 2. Do you sometimes expel something such as mucus or sputum when you cough? 3. During the last year, did you reduce your daily activities due to your respiratory problems? 4. Did you smoke at least 100 cigarettes throughout your life? 5. How old are you? Each question has multiple answers with a score that goes from 0 to 2, with a maximum total score of 10 points. A value ≥ 4 is considered high risk of having chronic obstructive pulmonary disease (COPD) and need to do additional tests.
Sample size
In order to calculate the sample size, we used data from the studies of Martínez FJ, which showed 84.4% sensitivity and 60.7% specificity (5) for the COPD-PS questionnaire; also, the studies of Miravitles M, who reported 93.6% sensitivity and 64.8% specificity10, and of Tsukuya G, who found 67.1% sensitivity and 72.9% specificity for the same questionnaire11. With this information, for a COPD prevalence of 8.9%4, 95% confidence level and 2% precision we required a minimum of 2012 subjects. The subjects entered the study in a sequential manner, and those who didn’t fulfill the inclusion criteria were re placed by others until the sample size was exceeded.
Data analysis
Data were obtained through the REDCap platform (web platform for building and managing online surveys and databases), and then they were analyzed with the statistical program SPSS, version 25. An initial description of qualitative variables was made in frequencies and percentages, and a description of quantitative variables was carried out using mean and standard deviation if their distribution was normal, or median and interquartile range if it wasn’t. Then, we compared and analyzed quantitative variables through the Student T Test or the Mann-Withney U Test according to their distribution and also compared qualitative variables through the Chi-Square Test. We calculated the sensitivity, specific ity, positive predictive value (PPV), negative predictive value (NPV), positive likelihood ratio (LR+), negative likelihood ratio (LR-), number needed to screen and number needed to harm. To evaluate reproducibility, we calculated the kappa coefficient and the intraclass correlation coefficient (ICC). Finally, we calculated the area under the receiver operating characteristic curve (AUROC) with the values of the COPD-PS questionnaire. We estimated the 95% confidence intervals for the reproduc ibility measures obtained and considered p <0.05 as statistically significant.
Ethical considerations
The research protocol followed the international ethical guidelines of the Declaration of Helsinki, the country’s ethical considerations of the 8430 resolution of 1993 and the Data Protection Law 1581. It was presented and approved by the Research Committee of the Universidad de la Sabana and by the Ethics Committee of the Clínica Universidad de La Sabana.
Results
Of a total of 2199 potentially eligible subjects for the study, 1662 participated in the final analysis. Figure 1 shows the flow of subjects through admission to the study and the respective exclusions.

General characteristics of the population
The mean age was 70.04 years (SD: 10.8); 86.1% were mixed-race; 56.8% were males and there was a COPD prevalence of 21.2%. 89.04% had indicated some respiratory symptom and 51.9% of the popu lation had completed basic primary education. Table 1 shows the characteristics of the population, respiratory symptoms, their background and the results of the lung function tests.

Results of the COPDS-PS questionnaire
Table 2 shows the answers to the COPD-PS questionnaire, classified by each one of the questions and with the total score, both in subjects with and without COPD. It is evidenced that each question and the average score of the questionnaires in both groups have a statistically significant p value for the diagnosis of COPD. The average response time for the questionnaire was calculated at 1 minute.

Reproducibility of results and validation of the COPD/PS questionnaire
Table 3 shows the analysis of sensitivity and specificity characteristics of the COPD-PS questionnaire at different cut-off points. The Youden index that determined the highest sensitivity together with the specificity (0.77-0.46, respectively) used a cut-off point ≥ 4. Also, for that cut-off point we found a posi tive predictive value of 2.279 and a negative predictive value of 0.883, and a positive likelihood ratio of 1.439 and a negative likelihood ratio of 0.490.

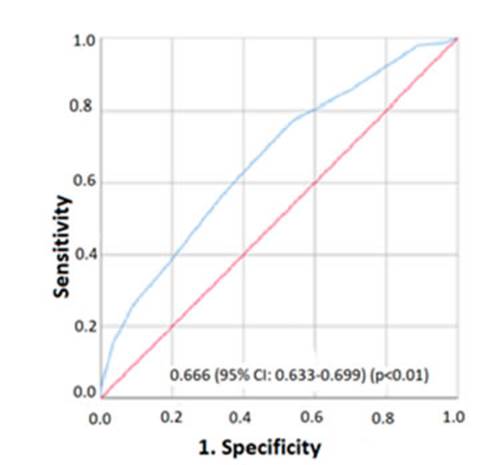
Table 3 Validation results and area under the receiver operating characteristic curve of the COPD-PS questionnaire
Discussion
In this study we evaluate the validation of the COPD-PS questionnaire for the screening of COPD in a Latin American population; the performance is good when compared to the value of the FEV1/FVC ratio of less than 0.7 post- bronchodilator (AUROC:0.666 95% CI:0.633-0.699). This performance was similar to that found by Tsukuya G11, who found an AUROC of 0.74 in the healthy overall population; however, with this score, AUROC values of even 0.88 have been found and reported by Miravitlles M10 in a population of patients at the first level of care. The sensitivity in the last study reached 93.6%; that is 16.4 points higher than the sensitivity observed in our study. Such difference may be due to a higher degree of exposure to smoking in the Spanish population studied by Miravitlles M et al., where the mean PYI was 42.79, twice as much as the one found in our study (PYI: 22).
The specificity found in our study (46.3%) is the lowest, compared to the validation studies of the COPD-PS questionnaire mentioned before; given the fact that this questionnaire evaluates respiratory symptoms, its capacity depends on the expression of such symptoms. In our population, the respiratory symptoms may eventually be expressed in a different way, maybe due to the high frequency of chronic bronchitis (CB) and the influence of the altitude. Subjects with CB can have mild obstruction not ex pressing tobacco exposure exclusively, thus affecting this score17,18. On the other hand, Horner found that subjects who live in geographical areas higher than 1500 MASL show less respiratory symptoms, even the ones with COPD19. We shall remember that when doing screening tests, we expect sensitivity to be higher than specificity.
Other validations prior to our study used two cut-off points. In the first validation analysis conducted in the United States a cut-off point of five was used. It reported adequate sensitivity and specificity values4. But subsequent validation analyses conducted in Spanish and Japanese populations used a cut-off point of four, also used in our study, because with that number a better sensitivity can be ob tained, with an acceptable reduction in the specificity of these populations10,11. The reason for these differences is not clear, but the cut-off points of different diagnostic tests may vary depending on the characteristics of the populations being evaluated, hence the importance of conducting the respective validation analyses. In our study, the COPD-PS questionnaire showed excellent test-retest reproduc ibility and reliability, with very good intraclass correlation coefficients and kappa coefficients for the dichotomous responses, both in the overall population and in the COPD and non-COPD groups. This favors the use of this tool.
In our study, the prevalence of COPD was 21.1%, similar to that reported in the PUMA study in a hospital environment; and obviously higher than the one reported in a general Colombian and Latin American population. The PREPOCOL study carried out in a community-based population showed that 9 out of 100 people older than 40 years had COPD, setting a prevalence of 8.9%4,20,21. It is known that a higher prevalence affects the positive predictive value and limits the extrapolation of the study results to the overall population; however, this questionnaire may be useful for the medical evaluation of different care levels where COPD underdiagnosis rates are still high, as shown by a study conducted in Argentina which found an underdiagnosis rate of 77.4%. And, in the PLATINO study the rate was 88.7%19,22-24.
To make the diagnosis of COPD, it is necessary to have tools that are easy to use, access and under stand by the overall population, that can be used for case detection or screening both in the community and in the hospital environment, and that aren’t used exclusively by professionals specialized in internal medicine and pulmonology. The objective of having such tools is to raise awareness among patients about their health status but also to create an alert in the healthcare personnel that makes them do tests such as a spirometry for early diagnosis, and take preventive measures such as quitting smoking and timely treatment. Despite its validation, reproducibility and potential benefits as a detection test for COPD patients in our population, some weaknesses should also be taken into account: the type of population of the study, which may limit the extrapolation of results, and the lack of cost estimates with which the findings of this study could have been strengthened. In future studies in our population, we could include in the evaluation of these scores the assessment of risk factors such as exposure to wood smoke and the estimation of the economic impact upon the use of these tools.

