










Services on Demand
Journal

Article
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO
Related links
-
 Similars in
SciELO
Similars in
SciELO
Share

 Permalink
PermalinkActa Odontológica Latinoamericana
On-line version ISSN 1852-4834
Acta odontol. latinoam. vol.22 no.3 Buenos Aires Dec. 2009
ARTÍCULOS ORIGINALES
Malignant oral-maxillary neoplasm in children and adolescents. A retrospective analysis from the biopsy service at a school of dentistry in Argentina
María Julia Piloni, Gladys Molina, Alicia Keszler
Department of Oral Pathology. School of Dentistry. University of Buenos Aires.
CORRESPONDENCE Dra. Maria Julia Piloni Department of Oral Pathology, School of Dentistry, University of Buenos Aires. Marcelo T. de Alvear 2142 2o “A”. Buenos Aires C1122 AAH, Argentina e-mail: mjpiloni@hotmail.com
ABSTRACT
There are few studies on oral-maxillary lesions in children and adolescents, and reports on malignant neoplasms are scarce. Comparison of available data is difficult due to the different criteria and racial-ethnic origin of the populations in each study. The aim of this work was to perform a retrospective study of malignant oral neoplasms in patients aged up to 20 years diagnosed at a center specialized in histopathological diagnosis of oral diseases between 1990 and 2005. The 24 retrieved cases accounted for 0.9% (n: 2434) of total biopsies in this age group during that period, and for 8.4% (n: 236) of the tumors. Mean age of the whole population was 9.2 years with even distribution according to sex. The most frequent tumor types were extranodal non-Hodgkin lymphoma (7 cases), osteosarcoma (4 cases) and Ewing sarcoma (3 cases). These data can be considered representative of our population of children and adolescents and serve as a basis for recognition and presumptive diagnosis in clinical practice.
Key words: Pediatric pathology; Malignant neoplasm; Childhood neoplasm.
RESUMEN
Neoplasias malignas bucomaxilares en niños y adolescentes. Análisis retrospectivo del servicio de biopsias de una facultad de odontología en Argentina
Los estudios sobre neoplasias bucomaxilares en niños y adolescentes son relativamente poco comunes y escasos los reportes sobre neoplasias malignas. Los datos disponibles son difíciles de comparar debido a diferencias en los criterios de análisis utilizados en cada estudio y origen racial-étnico de la población. El objetivo del presente trabajo fue realizar un estudio retrospectivo de neoplasias malignas bucales en pacientes de hasta 20 anos de edad diagnosticados en un centro especializado en diagnostico anatomopatológico bucal entre 1990 y 2005. Los 24 casos hallados representaron el 0.9% (n: 2434) del total de biopsias de este grupo etario en ese periodo y el 8.4% (n: 286) de los tumores. La edad media general fue de 9.2 anos, con similar distribución según sexo. Los tipos tumorales mas frecuentes fueron los Linfomas No Hodgkin extraganglionares (7 casos), el Osteosarcoma (4 casos) y el Sarcoma de Ewing (3 casos). Estos datos pueden ser considerados representativos de nuestra población infanto juvenil y sirven de base para a su reconocimiento y diagnostico presuntivo en la practica clínica.
Palabras clave: Patologia pediatrica; Neoplasias malignas; Neoplasias infantiles.
INTRODUCTION
Oral-maxillary neoplasms affecting children and adolescents may be benignant or malignant1. In recent years, several studies have dealt with the subject, but they are difficult to compare due to the different assessment criteria used by the authors. The maximum age limits considered are dissimilar2-9, the study periods range from 8 to 30 years and most of studies only make some reference to neoplasms within the full range of pathologies found. Those that specifically analyze tumor pathology report data mainly on benignant neoplasms, with little analysis or detail regarding malignant neoplasms3,10,11; while others are limited to some particular type of tumor12-14. The locations of the neoplasms considered also vary, and while some series include orofacial or oral-maxillofacial neoplasms5,15,16, others are limited only to maxillary neoplasms10,17. Moreover, the populations are of different racial-ethnic types2-5,7-11,15,16,18-20. Malignant oral-maxillary neoplasm affects all age groups16,21 and are in eighth place regarding frequency according to current statistics22. Nevertheless, they are infrequent in children. According to Keszler et al.1 in a previous retrospective study on the general distribution of pathologies among children and adolescents, malignant neoplasms represented 1.8% of total lesions diagnosed in this group of patients. Subsequently, Jones et al.8 reported a frequency of 1% in a study of similar design. When the scope of analysis in literature was limited exclusively to neoplasms, malignant neoplasms were found to have highly variable percentages of frequency according to different authors, and there were also differences in prevalent tumor types. According to Das et al.2 and more recently Shah et al.20, malignant neoplasms represented 1.2% and 0.8% respectively of total tumors found in the North American populations studied. In contrast, Sato et al.11, Chen et al.4 and Tanaka et al.5 reported that frequencies in Asian populations ranged from 2.8% to 7.1%; while according to Arotiba et al.3, Kalyanyama et al.23 and Aregbesola et al.16, they ranged from 40% to 51% in African patients. There are very few specific reports on malignant neoplasms in children and most of them refer to a particular type of tumor12,24-27. The only series of malignant neoplasms found in updated international literature was recently reported by Ajayi et al.28 in an African population; and no data on the subject were found for Argentina.
The aim of this work was to conduct a retrospective study of malignant tumor pathology in children and adolescents, from a laboratory specializing in oral pathology that receives samples for histopathological diagnosis from different geographic areas in Argentina.
MATERIALS AND METHODS
The study material was obtained from the archives of the Surgical Pathology Laboratory of the Oral Pathology Department of the School of Dentistry, University of Buenos Aires. We reviewed the cases with tumor pathology in patients up to 20 years of age from the 1990-2005 period and selected those with a histopathological diagnosis of malignant neoplasm. The clinical data were obtained from the respective biopsy protocols. All cases were re-evaluated microscopically. New histological sections and immunohistochemical techniques were performed in the cases for which it was necessary for diagnostic definition according to current criteria. The relative frequency of malignant neoplasms was estimated within the total pathologies and the specific tumor pathologies diagnosed for the period. The distribution by sex, age, localization and time of evolution was considered.
RESULTS
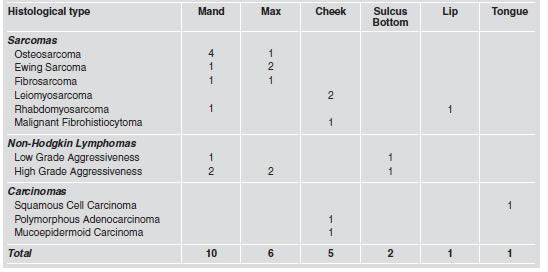
The 24 malignant neoplasms found accounted for 0.98% of the total lesions diagnosed in the 1990- 2005 period in children and adolescents (n: 2434), and 8.39% of the total number of neoplasms (n: 286). The overall mean age was 9.2 years with a range of 2.8 to 20 years and even distribution according to sex. Sixteen cases (66.6%) were intraosseous and eight (33.3%) were located in soft tissues. Clinical manifestations were rapidly growing, generally asymptomatic 2 to 5 cm tumors. Intraosseus tumors showed expansion of cortical plates, with erythematous mucosa in the area and effacement of the bottom of the sulcus, and radiographs showed an osteolytic lesion with undefined margins, with tooth displacement and rhizolysis. Tumors located in soft tissues had erythematous mucosa, very soft or friable consistency, and were sometimes ulcerated. Presumptive clinical diagnosis was malignancy in 40 % of the cases. Other assumptions included benign neoplasm or pseudo-tumors lesions (20%), and odontogenic lesions (15 %). No diagnosis was made in the remaining cases. The neoplasms found included 14 sarcomas, 7 lymphomas and 3 carcinomas. The sarcoma group included 4 osteosarcomas, 3 Ewing sarcomas, 2 fibrosarcomas, 2 leiomyosarcomas, 2 rhabdomyosarcomas and 1 malignant fibrohistiocytoma. For osteosarcomas, the M:F ratio was 3:1, mean age 11.3 years (7-18) and they were all located in the posterior mandibular area. For Ewing sarcomas, the M:F ratio was 2:1, mean age 10 years (6-14) and two of the three cases were located in the upper maxilla. The fibrosarcomas affected females aged 7 to 9 years; both were intraosseous, one located in mandible and the other in upper maxilla.
The 2 leiomyosarcomas affected males in the second decade of life and were located on cheek. The rhabdomyosarcomas affected one male and one female, both aged 5 years, one was intraosseous and the other labial. All the lymphomas were extranodal non-Hodgkin type. The mean age of these patients was 7.9 years (2.8-16) and the M:F ratio was 1.3:1. Five were located on the maxillaries and two on the soft tissues. All 7 cases were phenotype B. According to the morphological and immunohistochemical study, there were 5 (71%) with high grade of malignancy and 2 with low grade of malignancy. The first group included 2 Large-cell lymphomas, 2 Burkitt lymphomas and 1 Lymphoblastic lymphoma. The 3 cases of carcinoma occurred in females in the second decade of life. Two of them were adenocarcinomas, one polymorphic and the other mucoepidermoid; both located in minor salivary glands of cheek mucosa. The other was a squamous-cell carcinoma located on the edge of the tongue in an HIV+ patient (Tables 1 and 2).
Table 1: Distribution according to sex and decade of life of the different histological types of malignant neoplasms.
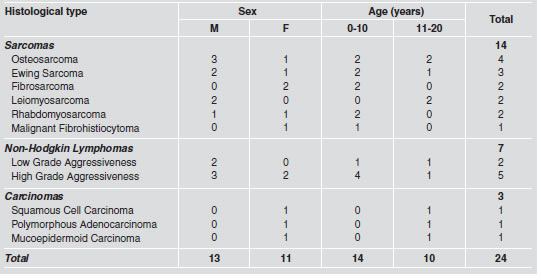
Table 2: Location of malignant neoplasms according to histological type.
Times to progression at the time of consultation recorded in the biopsy protocols were 30 to 60 days for the lymphomas and Ewing sarcoma; and up to 1 year for the osteosarcomas. For the other tumor types it ranged from 25 to 90 days.
DISCUSSION
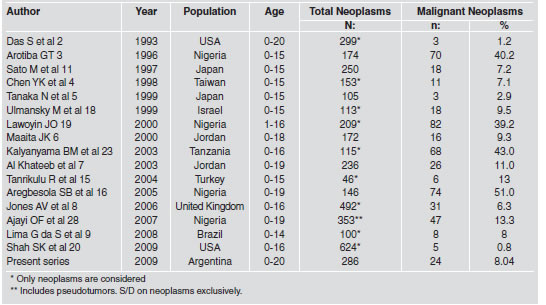
The frequency of malignant neoplasms in children and adolescents is highly variable according to data from international literature. While in the African population they represent 40 to 51% according to different authors3,16,19,23, in the Oriental population they range from 2.9% to 7.3%4,5,11. Data for Caucasian series are also dissimilar. The relative frequency of malignant neoplasms in this series is similar to that reported by Jones et al.8 and Ulmansky et al.18, but considerably higher than those reported by Das et al. in 19932 and recently by Shah et al.20. Although these differences may be due to geographic conditions and/or racial groups studied, even the variations observed between studies with the same geographic origin suggest that they may also be partly due to the different criteria used by the different authors to study them (Table 3).
Table 3: Frequency of malignant oral-maxillary neoplasms in children and adolescents according to international series over the past 15 years.
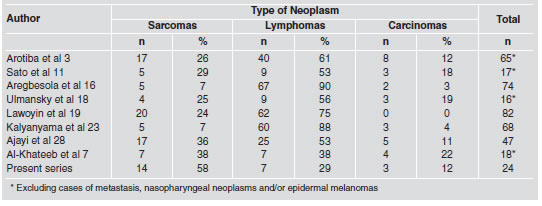
In this study, malignant neoplasms were evenly distributed according to sex and age; nevertheless, variations were found when specific tumor types were considered. Both sarcomas and lymphomas predominated in males, but while the former were distributed evenly over the first and second decades of life, the latter prevailed in the first decade. Sarcomas in general were the most frequent neoplasms (58%), followed by lymphomas (29%). These data differ from those reported by most authors, who find that lymphomas are the most common tumor type in this age group3,11,16,18,19,23,28 or report equal numbers of cases for both entities7 (Table 4).
Table 4: Histological types of malignant neoplasms found in children and adolescents compared to data from literature.
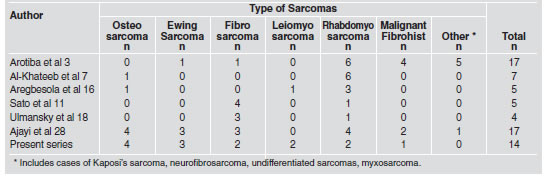
In this series, sarcomas included lesions with different kinds of histogenesis, but osteosarcomas prevailed, which was another difference with the data from literature. According to Arotiba et al.3, Al Khateeb et al.7 and Aregbesola et al.16, rhabdomyosarcoma was the most frequent sarcoma; Sato et al. 11 and Ulmansky et al.18 report a higher frequency of fibrosarcomas, while Ajayi et al.28 report the same number of osteosarcomas and rhabdomyosarcomas (Table 5).
Table 5: Types of sarcoma found in this series and in data from literature.
Carcinomas were the least frequent, in agreement with reported data7,16,18. This kind of tumor is infrequent in patients under 20 years of age and extremely rare in the first decade of life21. The three cases found were from females aged 15 to 20 years, and corresponded to 2 adenocarcinomas in minor salivary glands and 1 squamous cell carcinoma on lingual mucosa. The histological type of the salivary neoplasms reported in different series is variable and, due to the low number of cases reported, not comparable. This series includes one mucoepidermoid carcinoma and one polymorphic adenocarcinoma. These two types of tumor have been reported as the most frequent in a study performed exclusively on neoplasms of the major and minor salivary glands in a Chinese population29. The etiological factors of squamous cell carcinomas in adolescents have been widely discussed. The possibility of tobacco and alcohol having a carcinogenic effect of on young patients is low because exposure time would be relatively too low to establish a causeeffect. Nevertheless, other factors such as genetic predisposition, viral infections and states of immunodeficiency, among others, may condition their development30. The case included in this series corresponded to an HIV+ patient. Malignant neoplasms in children and adolescents are infrequent, but are usually high-degree, with rapid progression and potentially life-threatening, therefore an early diagnosis is vital. The data presented in this series may be considered representative of our environment and serve as a basis for recognition and presumptive diagnosis in clinical practice prior to biopsy.
ACKNOWLEDGMENT
The study was supported by the grant O012 from the University of Buenos Aires.
1. Keszler A, Guglielmotti MB, Dominguez FV. Oral pathology in children. Frequence, distribution and clinical significance. Acta Odontol Latinoam 1990;5:39-48. [ Links ]
2. Das S, Das AK. A review of pediatric oral biopsies from a surgical pathology service in dental school. Pediatr Dent 1993;15:208-211. [ Links ]
3. Arotiba GT. A study of orofacial tumors in Nigerian children. J Oral Maxillofac Surg 1996;54:34-38. [ Links ]
4. Chen YK, Lin LM, Huang HC, Lin CC, Yan YH. A retrospective study of oral and maxillofacial biopsy lesions in a pediatric population from southern Taiwan. Pediatr Dent 1998;20:404-410. [ Links ]
5. Tanaka N, Murata A, Yamaguchi A, Kohama G. Clinical features and management of oral maxillofacial tumors in children. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1999;88:11-15. [ Links ]
6. Maaita JK. Oral tumors in children: a review. J Clin Pediatr Dent 2000;24:133-135. [ Links ]
7. Al-Khateeb T, Al-Hadi Hamasha A, Almasri NM. Oral and maxillofacial tumours in North Jordanian children and adolescents: a retrospective analysis over 10 years. Int J Oral Maxillofac Surg 2003;32:78-83. [ Links ]
8. Jones AV, Franklin CD. An analysis of oral and maxillofacial pathology found in children over a 30 year period. Int J Paediatr Dent 2006;16:19-30. [ Links ]
9. Lima G da S, Fontes ST, de Araujo LM, Etges A, Tarquinio SB, Gomes AP. A survey of oral and maxillofacial biopsies in children: A single-center retrospective study of 20 years in Pelotas-Brazil. J Appl Oral Sci 2008;16:397-402. [ Links ]
10. Asamoa EO, Ayanlere AO, Olaitan AA, Adekeye EO. Paediatric tumours of the jaws in Northen Nigeria. J Cranio Maxillofac Surg 1990;18:130-135. [ Links ]
11. Sato M, Tanaka N, Sato T, Amagasa T. Oral and maxillofacial tumours in children: a review. Br J Oral Maxillofac Surg 1997;35:92-95. [ Links ]
12. Hicks J, Flaitz C. Rhabdomyosarcoma of the head and neck in children. Oral Oncol 2002;38:450-459. [ Links ]
13. Donaldson ME, Geist JR, Daley TD. Osteosarcoma of the jaws in children. Int J Paediatr Dent 2004;14:54-60. [ Links ]
14. Guerrisi M, Piloni MJ, Keszler A. Odontogenic tumors in children and adolescents. A 15-year retrospective study in Argentina. Med Oral Patol Oral Cir Bucal 2007;12:E180-185 [ Links ]
15. Tanrikulu R, Erol B, Haspolat K. Tumors of the maxillofacial region in children: retrospective analysis and long-term follow-up outcomes of 90 patients. Turk J Pediatr 2004; 46:60-66. [ Links ]
16. Aregbesola SB, Ugboko VI, Akinwande JA, Arole GF, Fagade OO. Orofacial tumours in suburban Nigerian children and adolescents. Br J Oral Maxillofac Surg. 2005; 43:226-231 [ Links ]
17. Skiavounou A, Iakovou M, Kontos-Toutouzas J, Kanellopoulou A, Papanikolaou S. Intra-osseous lesions in Greek children and adolescents. A study based on biopsy material over 26-year period. J Clin Pediatr Dent 2005;30:153-156. [ Links ]
18. Ulmansky M, Lustmann J, Balkin N. Tumors and tumorlike lesions of the oral cavity and related structures in Israeli children. Int J Oral Maxillofac Surg 1999;28:291-294. [ Links ]
19. Lawoyin JO. Paediatric oral surgical pathology service in an African population group: a 10 year review. Odontostomatol Trop 2000;23:27-30. [ Links ]
20. Shah SK, Le MC, Carpenter WM. Retrospective review of pediatric oral lesions from a dental school biopsy service. Pediatr Dent 2009;31:14-19. [ Links ]
21. Chidzonga MM. Oral malignant neoplasia: a survey of 428 cases in two Zimbabwean hospitals. Oral Oncol 2006;42: 177-183. [ Links ]
22. Parkin DM, Bray F, Ferlay J, Pisani P. Global Cancer Statistics 2002. CA Cancer J Clin 2005;55:74-108. [ Links ]
23. Kalyanyama BM, Matee MI, Vuhahula E. Oral tumours in Tanzanian children based on biopsy materials examined over a 15 years period from 1982 to 1997. Int Dent J 2002; 52:10-14. [ Links ]
24. Chigurupati R, Alfatooni A, Myall RWT, Hawkins D, Oda D. Orofacial rhabdomyosarcoma in neonates and young children: a review of literature and management of four cases. Oral Oncol 2002;38:508-515. [ Links ]
25. Al-Khateeb T, Bataineh AB. Rhabdomyosarcoma of the oral and maxillofacial region in Jordanians: A retrospective analysis. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2002;93:580-585. [ Links ]
26. Namin AK, Moshref M, Shahoon H, Mashhadi A, Khojasteh A. Intraosseous mucoepidermoid carcinoma of the maxilla in a teenager: A case report and review of literature. Oral Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2005;100:93-96. [ Links ]
27. Ugar DA, Bozkaya S, Karaca I, Tokman B, Pinarli FG. Childhood craniofacial Burkitt lymphoma presenting as maxillary swelling: report of a case and review of literature. J Dent Child 2006;73:45-50. [ Links ]
28. Ajayi OF, Adeyemo WL, Ladeinde AL, Ogunlewe MO, Omitola OG, Effiom OA, Arotiba GT. Malignant orofacial neoplasms in children and adolescents: A clinicopathologic review of cases in a Nigerian tertiary hospital. Int J Pediatr Otorhinolaryngol 2007;71:959-963. [ Links ]
29. Laikiu L, Hongwei L, Hongbing J, Zhixiu H. Epithelial salivary gland tumours of children and adolescents in west China population: a clinicopathologic study of 79 cases. J Oral Pathol Med 2008;37:201-205. [ Links ]
30. Seyedmajidi M, Faizabadi M. Squamous cell carcinoma of the tongue in a 13 year old boy. Arch Iranian Med 2008;11:341-343. [ Links ]

