











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Similars in
SciELO
Similars in
SciELO 
 Permalink
PermalinkINTRODUCTION
Molar Incisor Hypomineralization (MIH) is a developmental defect in the structure of the dental enamel, affecting the mineralization of one to four first permanent molars, frequently associated with affected mineralization in one to eight permanent incisors1.
Histologically, the hypomineralized enamel shows areas of increased porosity2 and the enamel structure itself is disorganized, depending on the degree of hypomineralization3. Clinically, MIH is characterized by creamy white, yellow or brown demarcated opacities on the enamel surfaces, while in severe presentations, the tooth structure is lost4.
The etiology of MIH has not been entirely elucidated. MIH is usually caused by systemic alterations occurring during the prenatal period or during the first three years of life, thus affecting enamel development5, 6. Furthermore, it has been proposed that the etiology of this condition is associated with the gene variations involved in amelogenesis7. Teeth affected by MIH, due to the hypomineralization and their morphological characteristics may cause sensitivity and pain, particularly in children. Moreover, affected molars are more susceptible to the accumulation of biofilm, due to the loss of enamel structure, which occurs after tooth eruption and is usually caused by mastication forces8. Epidemiological studies show a wide range in the prevalence of MIH, from 2.8% in children in Hong Kong, 9 to 9.7% in children in India 10 and 40.2% in children in Brazil11. The literature provides information on the association between dental caries and MIH, and studies in Spain show that children with severe MIH are more likely to present dental caries12. However, a study conducted on German children found no association between MIH and dental caries13. While a systematic review of published research suggested an association between these conditions, the results should, however, be interpreted with caution due to the lack of high-quality studies14.
The limitations to comparing the results found for the association between MIH and dental caries include the different criteria used in the studies to evaluate the presence and severity of MIH and dental caries. In recent years, new caries indices have been used, one such being ICDAS (International Caries Detection and Assessment System). ICDAS considers the degree of progress of the carious lesion, and includes the identification of incipient lesions, microcavities, and lesions that involve the destruction of more than half the tooth surface. Furthermore, the criteria developed by the European Academy of Paediatric Dentistry for the evaluation of MIH in index teeth considers the extent of the affected area, the loss of tooth structure and color of the lesion, which are characteristics associated with the severity of MIH15, 16. The use of these indices would enable a more detailed analysis of the association between MIH and dental caries. Therefore, the aim of this study was to identify the relationship between molar incisor hypomineralization (MIH) severity and cavitated carious lesions in schoolchildren in Mexico.
MATERIAL AND METHODS
Study group
This study comprised a cross-sectional design. The area selected had a population of 833,779 inhabitants (5.4% of the total population of the State of Mexico), in which 55.5% of people over 15 years of age did not have higher education, and 55.8% had access to health services. Government statistics indicated a very low socioeconomic level in study area17. For convenience, three schools were selected, one each from the northern, central and southern sections of the study area.
The sample size was calculated to detect an Odds Ratio (OR) = 2.5 with 80% power and an alpha of 0.05, considering a probability of 0.18 and MIH= 0.30 = dental caries. The study group included schoolchildren aged 8 to 12 years presenting the eruption of at least one first permanent molar. The exclusion criterion was presence of orthodontic attachments that prevented the examination of the tooth surface. A total 650 parents were asked to provide consent to the participation of their children in the study, with 600 accepting and signing an informed consent form (response rate 92.3%). Ninety-four of the potentially eligible 600 schoolchildren were excluded: 1 due to the presence of an orthodontic appliance, 83 because they did not attend school on the days of examination, and 10 who did not present the eruption of any first permanent molars when the oral evaluation was performed. Thus, 506 schoolchildren were included in the study. The study was approved by the Ethics Committee of the Faculty of Dentistry at the National Autonomous University of Mexico (Protocol 20180515).
The research was conducted in full accordance with the World Medical Association Declaration of Helsinki.
The variables included in the study were: age (in years); sex (boy/girl); toothbrushing frequency (number of times a day); and, the Simplified Oral Hygiene Index (OHI-S) dichotomized into poor (OHI-S>2 score) and good hygiene (OHI-S<2 score). Dental caries were evaluated by applying ICDAS II criteria, forming the categories ICDAS II=0, ICDAS II= 1-3, and ICDAS II= 4-6. MIH was evaluated using the criteria of the European Academy of Paediatric Dentistry (EAPD) and was classified in terms of presence/absence and severity of the lesion and in three categories: mild, moderate and severe18. The MIH level in each child was individually defined according to the first permanent molar or permanent incisor most severely affected by MIH.
Clinical oral examination
The evaluation of MIH included the inspection of permanent occlusal /incisal buccal and palatal surfaces of all erupted molars and incisors, which were classified according to the criteria for EAPD19. This index classified MIH based on visual clinical presentation, the extension of the surface affected by the lesion (I - less than one third of the affected tooth, II - at least one third but less than two surfaces, and III - post-eruptive presence of structure loss) and the color of the lesion (white or creamy opacities and yellow or brown opacities). Based on the index, the following MIH severity categories/criteria were constructed:
Severity criteria
Mild: One white or creamy demarcated opacity with a diameter >1 mm and affecting less than one third of the tooth surface.
Moderate: One yellow or brown demarcated opacity with a diameter >1 mm and affecting less than one third of the tooth surface; two or more white or creamy demarcated opacities >1 mm affecting at least one third but less than two thirds of the tooth surface, on which rough enamel is frequently found; post-eruptive enamel breakdown <2 mm; and, atypical restorations involving at least one third but less than two thirds of the affected tooth surface. Severe: Two or more yellow or brown demarcated opacities with a diameter>1 mm affecting at least one third or more of the tooth surface; two or more white or creamy demarcated opacities with a diameter >1 mm, affecting at least two thirds of the tooth surface; post-eruptive enamel breakdown >2 mm; and, atypical restoration involving more than two thirds of the affected tooth surface.
The assessment of dental caries was performed by applying the ICDAS II criteria, which include the identification of incipient lesions (white spots and microcavities on the enamel) and cavitated carious lesions, including in the highest category the destruction of more than half of the tooth surface. This index classified caries with scores ranging from 0 to 6, with higher values indicating greater severity of the carious lesions20.
Clinical oral evaluations were conducted by one dentist using dental mirrors (# 5), WHO probe and type artificial light, with the teeth brushed prior to the procedure. The measurements taken by this dentist had previously been standardized with gold standard, with Cohen's kappa coefficient for intraexaminer calibration of 0.81 and 0.84 for MIH and dental caries, respectively. Infection control standards for the examination of the children's oral cavity were followed.
Statistical analysis
Comparisons were made for age, sex, toothbrushing, oral hygiene (OHI-S) and MIH between schoolchildren with and without caries, using the Pearson Xi square test for categorical variables and the Kruskal-Wallis test for continuous variables. The association between the independent MIH variable was classified as mild, moderate or severe at subject level, while the dependent caries variable for incipient lesions (ICDAS II = 0 and ICDAS II = 1-3) and cavitated lesions (ICDAS II >4) was assessed via multinomial logistic regression models, adjusting for the covariates age, sex, toothbrushing and oral hygiene. Logistic regression analysis was also performed to determine the association between MIH and cavitated caries lesions (ICDAS II >4) at tooth level. The construction of the logistic regression models considered the correlation between teeth within each individual via the cluster option. The Odds Ratio (OR) and a 95% confidence interval (95%) were obtained. Values of p < 0.05 were considered statistically significant. Theoretically plausible interactions, such as oral hygiene and MIH and age and MIH, were also explored. The analysis was performed using the Stata 14 program (Stata Corp, College Station, TX, USA).
RESULTS
A total 506 schoolchildren were included in the study, with mean age 9.74 (± 1.36) years. The percentage of girls and boys examined was 49.4% and 50.6%, respectively. It was ascertained that 61.1% brushed their teeth twice a day or more frequently, and 38.9% less than twice a day, with 98.9% using toothpaste and, according to the OHI-S evaluation, 44.9% of schoolchildren having good oral hygiene and 55.1% having poor oral hygiene. By sex, a higher proportion of girls reported that they brushed their teeth twice a day or more frequently, which was more frequent compared to the boys (54.0% vs. 45.9%, p = 0.009).
Molar incisor hypomineralization
The prevalence of MIH was 42.4% (215/506), distributed by sex as 51.6% boys and 48.4% girls (p=0.390). Of the schoolchildren who presented MIH; 29.5% presented sensitivity and 8.7% pain.
When only children with four erupted permanent first molars (PFMs) were considered (n=496), the prevalence of MIH was 42.9%, comprising 40.9% in boys and 45.1% in girls (p=0.359). The results, according to the MIH followed by showed that 57.5% of the schoolchildren did not present enamel defects; 21.7% presented mild, 7.7 % moderate and 13.0% severe enamel defects.
While the frequency of toothbrushing reported by the children was not associated with MIH (61.9% MIH vs. 60.5% non-MIH, p=0.753), poor oral hygiene (OHI-S>2) was not associated with the presence of MIH in children with and without MIH, 58.6% and 52.6%, respectively (p=0.178).
Dental caries
The prevalence of caries (ICDAS II 1-6) was 95.6%, which, by category (ICDAS II 1-3 and ICDAS II >4) translated as 61.6% and 34.0%, respectively. The mean number of carious lesions was 3.80 (±3.53) for ICDAS II 1-3 and 1.53 (±2.72) for ICDAS II >4. Six point six percent (6.6%) of schoolchildren had restorations in permanent teeth and 7.4% had pit and fissure sealants.
Dental caries and MIH
The prevalence of caries in primary dentition (ICDAS II >4) was higher in schoolchildren with MIH compared to children without MIH (56.3% vs. 46.0%, p=0.023). In the logistic regression model an association was found between MIH and caries (ICDAS II >4) in primary dentition [OR=1.60 (1.092.34; p=0.015)].
The prevalence of caries in permanent dentition (ICDAS II >4) was higher in schoolchildren with MIH compared to children without MIH (44.7% vs. 26.1%, p<0.001). Teeth with MIH showed a higher percentage of cavitated carious lesions compared to teeth without MIH. Table 1 presents the distribution of MIH severity scores by ICDAS index and the association observed between these conditions, demonstrating that most of the children with severe forms of MIH showed cavitated caries lesions (p< 0.001).
In the multinomial logistic regression model undertaken at subject level for incipient caries lesions (ICDAS II= 1-3) and MIH, controlling for age, sex, toothbrushing frequency and oral hygiene, no significant association was found between MIH and initial caries lesions in the mild [OR=0.63 (CI95% 0.19 - 2.09) p=0.457], or moderate/severe categories [OR=1.11 (CI95% 0.34 - 3.55) p=0.854 (Table 2). On the other hand, for cavitated caries lesions (ICDAS II >4), the schoolchildren with presence of moderate/severe MIH were more likely to have lesions, ICDAS II >4 lesions [OR=3.28 (CI95% 1.01 - 10.6); p=0.048], compared to the group without MIH. In the category of mild MIH and cavitated lesions, no significant association was found (p=0.131). Poor oral hygiene was associated with cavitated caries lesions (ICDAS II >4) in schoolchildren with MIH (OR=3.62 (CI95% 1.36 -9.61); p=0.010) (Table 2).
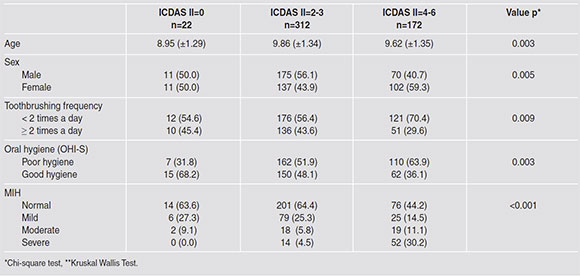
Table 1 Characteristics in schoolchildren aged 8 to 12 years with and without caries from the State of Mexico.

Table 2 Adjusted odds ratios from the multinomial logistic regression model for dental caries and Molar Incisor Hypomineralization (MIH) in schoolchildren 8 -12 years of age.
The results of the regression model for dental caries and the number of permanent first molars affected (Table 3) showed a significant association with the number of teeth with MIH-associated cavitated carious lesions (ICDAS II >4). Children presenting three or four permanent first molars with MIH were more likely (OR=4.30; CI95% 1.17 - 15.8, p=0.028) to present cavitated caries lesions (ICDAS II >4), while for one or two molars with MIH, the association was OR=3.69 [(CI95% 1.00 - 13.5), p=0.048] compared to non-MIH children. Finally, an association between enamel hypomineralization and dental caries in PFMs was detected when individual teeth were considered as the units of analysis (Table 4). The PFMs with MIH were more likely to have cavitated lesions (ICDAS II >4) compared to molars without MIH (OR=2.24; CI95% 1.52 - 3.28, p<0.001). No interaction was identified in the models.

Table 3 Adjusted odds ratios from the multinomial logistic regression model for the association between enamel hypomineralization and dental caries in permanent first molars in schoolchildren 8 -12 years of age.

DISCUSSION
In this study, the presence of MIH was associated with cavitated carious lesions assessed using ICDAS II. Furthermore, the severity of MIH showed an impact on dental caries, with schoolchildren with moderate/severe categories of MIH being more likely to have cavitated lesions compared to schoolchildren without MIH. The association found between cavitated carious lesions and MIH is consistent with the results of studies conducted in other population groups14, 21, 22. Children in Thailand with MIH were 4.6 times as likely to have caries in permanent teeth than children without MIH6. Similarly, an association between MIH and caries experience was found in 6 to 12-year-old Brazilian schoolchildren23. It is likely that the association between MIH and dental caries is easier to recognize in groups with high risk of caries and high severity of MIH.
The association between MIH and caries could be explained by the morphological changes observed in teeth with MIH because the hypomineralized enamel microstructure is disorganized, with the interprismatic spaces being less compact than in healthy enamel24. Moreover, mechanical properties such as hardness, elasticity and chemical composition are deteriorated, compared to healthy enamel3. As the enamel in teeth presenting MIH becomes brittle, it is clinically possible to detect loss of continuity, fractures or even loss of tooth structure, which favor the accumulation of biofilm on the porous enamel and the exposed dentin. Accordingly, children with MIH showed a greater level of biofilm accumulation. Biofilm accumulation is favored by the porous surface of the affected teeth, leading to penetration by cariogenic bacteria, which destroys hypomineralized enamel more quickly than sound enamel14. Additionally, schoolchildren with teeth affected by MIH may suffer from dentinal sensitivity and are more likely to find it difficult to brush their teeth properly25. While this study revealed an MIH prevalence of 42.4%, Gurrusquieta BJ et al., found that prevalence in Mexican children aged 6 to 12 years was 15.8%, i.e., lower than that found in the present study26. This differences in prevalence of MIH among school children could be due to the differences in etiological factors, lifestyle and genetic characteristics in the populations studied. The percentage of children affected by MIH in the study group was higher than that identified in studies undertaken in populations in India (9.7%) 10 and Thailand (20.0%) 6, but similar to MIH prevalence reported in the study undertaken on schoolchildren in Brazil, (40%)11. It may be difficult to compare MIH prevalence among different studies, considering the different indices used for MIH assessment, the age of the participants and the caries risk for the specific study group, among other factors.
In the Mexican children included in this study, most of the MIH cases detected presented a moderate level of severity. While the MIH index of the European Academy of Pediatric Dentistry is widely used in epidemiological and clinical studies, it does not directly classify MIH severity; nevertheless, it does assess tooth characteristics that facilitate the construction of a severity score.
Advanced carious lesions (ICDAS II 4-6) and incipient carious lesions (ICDAS II 1-3) were evaluated in this study. The small lesions were not associated with the presence or severity of MIH. Ismail et al., in a study conducted on infants and their caregivers in low-income families in Detroit, Michigan, identified that the risk factors for incipient lesions were not necessarily the same as those for cavitated lesions27.
In this study, incipient and cavitated lesions were assessed by applying ICDAS II criteria, which provide a broad perspective on the caries process by considering initial lesions previously excluded by both clinical and epidemiological studies. In this research, incipient lesions (ICDAS II 1-3) were found in more than half of the study group, and cavitated lesions (ICDAS II >4) in approximately one third of the group. Similarly, studies conducted in Spain on 12-year-old children using the same cutoff value (ICDAS II >4) found a 37.7% caries prevalence in permanent dentition28.
Some of the limitations of this study are related to its cross-sectional design, as some teeth affected by MIH were likely not to have been detected due to the presence of restorations that could mask the occurrence of MIH. However, only 6.6% of participants in the study group presented dental fillings in permanent teeth. The extrapolation of the results of the study to other groups from different areas of Mexico has limitations due to the heterogeneity of children in the city; however, the schools featured in this study are located in low income neighborhoods, the type of neighborhood where more than 50% of the families featured in this study live.
The identification of an association between MIH and dental caries is considered important, particularly in children presenting various dental problems, such as poor oral hygiene, hypersensitivity, high caries risk and high treatment needs. The results suggest that when MIH is mild, the dentist may select a conservative approach based on general preventive measures such as brushing with fluoridated toothpaste. However, when MIH is moderate/ severe, a proactive approach is important, as is the use of additional measures for preventing caries, such as the application of glass ionomer sealants. A cohort study showed that it is possible to maintain the tooth structure of the areas with MIH opacities, with the authors of said study recommending a conservative approach in mild MIH cases16.
In conclusion, this study shows that more than one third of the children had MIH, identifying an association between MIH and dental caries evaluated through ICDAS II. It is important that children with MIH are diagnosed early in order that they receive preventive measures and timely treatment to protect the tooth structure affected and prevent the deterioration of oral health and, thereby, quality of life.

