











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Similars in
SciELO
Similars in
SciELO 
 Permalink
PermalinkINTRODUCTION
Tooth loss causes sequential morphological changes in hard and soft tissues of the alveolar ridge, especially during the first 8 weeks after tooth extraction. Without intervention, there is great loss of volume due to bone resorption 1 , 2 . Conservative guided bone regeneration (GBR) procedures seek to maintain the alveolar bone structure for subsequent rehabilitation with dental implants 1 . GBR techniques have evolved based on the use of biomaterials, making procedures less traumatic, safer, and cost-effective, re-establishing function and aesthetics in a stable, satisfactory manner 2 , 3 .
Platelet-rich fibrin (PRF), which is a platelet concentrate of leukocytes, platelets and fibrin, was developed in the search for new GBR alternatives 4 . The cellular elements interspersed in a fibrin mesh potentiate the formation of new blood vessels, minimize immunological action because they are from an autologous biological source, promote antibacterial action and secretion of cytokines by leukocytes, and activate mechanisms of tissue repair through of multiple growth factors released gradually 4 , 5 . PRF has been used since the 2000s and, especially in recent years, experimental protocols and clinical research reports have increased exponentially 5 . The use of PRF has been documented for alveolar preservation, sinus lift, and treatment of intrabony defects or furcation defects 4 . The combination of PRF, cells and different bone substitutes could be a promising alternative in bone regeneration proposals 6 . In addition to its biological benefits, the easy acquisition and affordability of PRF make it attractive for use in GBR 3-5 .
Although natural bone grafts of autogenous, allogeneic or xenogeneic origin are good biological alternatives in dentistry 3 , 7 8 , alloplastic materials have gained greater acceptance among professionals and patients, whether due to the fact that there is less morbidity at the surgical site or due to absence of moral and religious issues such as stigmatization of the cadaveric or animal source 3 , 9 . Biphasic calcium phosphate (BCP) is a synthetic ceramic consisting of hydroxyapatite (HA) and beta tricalcium phosphate (P-TCP) which has been used for decades in GBR, demonstrating biocompatibility, biodegradability and great clinical interest 9 . Few papers have evaluated bone formation at the histological level of BCP compared to other classes of biomaterials 3 , 9 . However, bone regeneration in human fresh alveolar sites with PRF is as yet incipient, as the literature offers in situ descriptive analyses and lacks more robust quantitative results, which could impair its therapeutic predictability 10 . The same applies to its association with BCP, which has not yet been described in the literature 11-13 . The proposal of this study therefore has scientific originality.
The aim of this study was to perform a histomorphometric evaluation of human extraction sockets treated with either autologous PRF, an association between PRF and BCP, or only alloplastic BCP.
MATERIALS AND METHODS
This research adopted the ethical principles of respect for people, non-maleficence, beneficence, and justice described in the Belmont Report (1978) and the Brazilian guidelines of the Resolution of the National Health Council No. 466 (2012), which establishes the basic requirements for research involving human beings in the country. This research was assessed and approved by the local Ethics Committee of the Universidade Estadual Vale do Acarau via Plataforma Brasil (register CAAE #91602218.0.0000.5053 and approval protocol #2.806.761) before data collection started. Participants’ consent was registered through a Free and Informed Consent Form (FICF), which provided information in appropriate language about the purpose of the research, as well as ensuring the confidentiality of identities.
Type of study
This was a clinical study with quasi-experimental design and a quantitative, structured approach. The target population consisted of patients recruited in a public university dental care service.
Sample
This study was conducted at a public university dental care service in the city of Sobral, Ceara, Brazil. For a good clinical experimental planning, sample size was calculated using the statistical formula for finite population: N. p.q.(Za/2)2=n.(p.q. (Za/2) 2 +(N-1).E 2 ), where N: requested population; n: representative sample; p: % inside of research subject; q: % outside of research subject; Za/2: degree of confidence; E: margin of error 14 .
Clinical evaluation is an important step in the calculation of the probabilistic sample, considering the profile of the public served between August 2018 and April 2019. Inclusion criteria were systemically healthy patients, of both sexes, young adults in the age group 20 to 45 years, with indication of elective single extractions, unilateral or bilateral, of upper premolars, without active periodontal problems, non-smokers, without the presence of known psychological disorders, good oral hygiene status and without any functions that could compromise occlusion. Exclusion criteria were patients who did not consent to participate in the study, did not agree to undergo laboratory and imaging exams (periapical X-ray, panoramic and tomography) prior to the surgeries for appropriate planning of the cases, or did not sign the FICF. The minimum probabilistic sample calculated for the study was 10 patients.
At first, a higher number of patients was included than the proposed goal, with 15 patients eligible for the study, 6 male and 9 female, totalling 16 surgical beds, with 1 patient indicated for bilateral surgery. After the first surgeries, 5 patients dropped out, which maintained the minimum number of 10 patients and 11 surgical beds for this clinical research. For all groups, a single post-extraction region per quadrant in the upper dental arch was always considered for each type of treatment proposed.
Human socket grafting
Surgical planning involved two general steps for all groups: tooth removal followed by grafting (time 0), and bone biopsy and dental implant (8 months after the initial procedure). Preoperative care included pre-emptive medication (2 tablets of dexamethasone 4 mg 1h before) and mouthwash with Periogard™ (Colgate, Brazil), 0.12% chlorhexidine for 1 minute.
Infiltrative anaesthesia was performed with Articaine 100™ (DFL, Brazil), 4% articaine and 1:100,000 epinephrine. Relaxing incision without much extension to the bottom of the vestibule facilitated detachment of the mucoperiosteal flap, surgical access, dislocation and removal of the premolar, biomaterial grafting in the dental socket and suturing the region with 4.0 nylon thread (Tecnew, Brazil).
A trained, qualified team (an oral surgeon, a dental assistant, and a nursing assistant) collected PRF in the dental office. The protocol for obtaining an autologous PRF was based on Resolution No. 158/2015 of the Federal Council of Dentistry in Brazil, which regulates the use of platelet aggregates in dental procedures in the country. The method of obtaining PRF enables acquisition of 4 types of conformation ofthe biomaterial: PRF clot, PRF plug, PRF membrane and Liquid PRF, where sticky bone represents an association of PRF clot and liquid PRF, as previously described 4 . For this reason, there were two blood samples per venepuncture in patients in the PRF group: before (8 tubes) and after (2 tubes) tooth extraction. The centrifugation step adopted the protocol described by Oliveira et al. 5 , using Spin Plus™ equipment (Spinlab, China), with an angle of 45 degrees, 78 mm radius, time 10 minutes and 1500 rpm, resulting in a centrifugal force of 196g to obtain PRF clot and its derivates, plugs or membranes according to manual processing of the surgeon. To obtain liquid fibrin, immersion solution of PRF clot to generate the mixture of i-PRF, centrifugation without additives was performed for 3 minutes at 2700 rpm 15 .
The experimental groups and final number of patients were divided into: PRF plug covered with PRF membrane (G1, n=4 patients, or 5 surgical beds); sticky bone or PRF associated with Boneceramic™ (Straumann, Switzerland), a BCP constituted of 60% HA and 40% P-TCP, covered by collagen membrane Lumina coat® (Critéria, Brazil) (G2, n=3 patients, or surgical beds); and Boneceramic™ graft covered by Lumina coat® (Control, n=3 patients, or surgical beds). Postoperative care included prescription of analgesic medication and use of mouthwashes. Clinical evaluations were performed at seven and thirty days, following the presence of some area of contamination, inflammation or dehiscence of the wound or loss of graft material. Visits after 90 days were scheduled for further evaluation of the procedures. Figs. 1, 2 and 3 summarize the sequence of clinical, tomographic, and surgical evaluations and protocols conducted in the different groups.
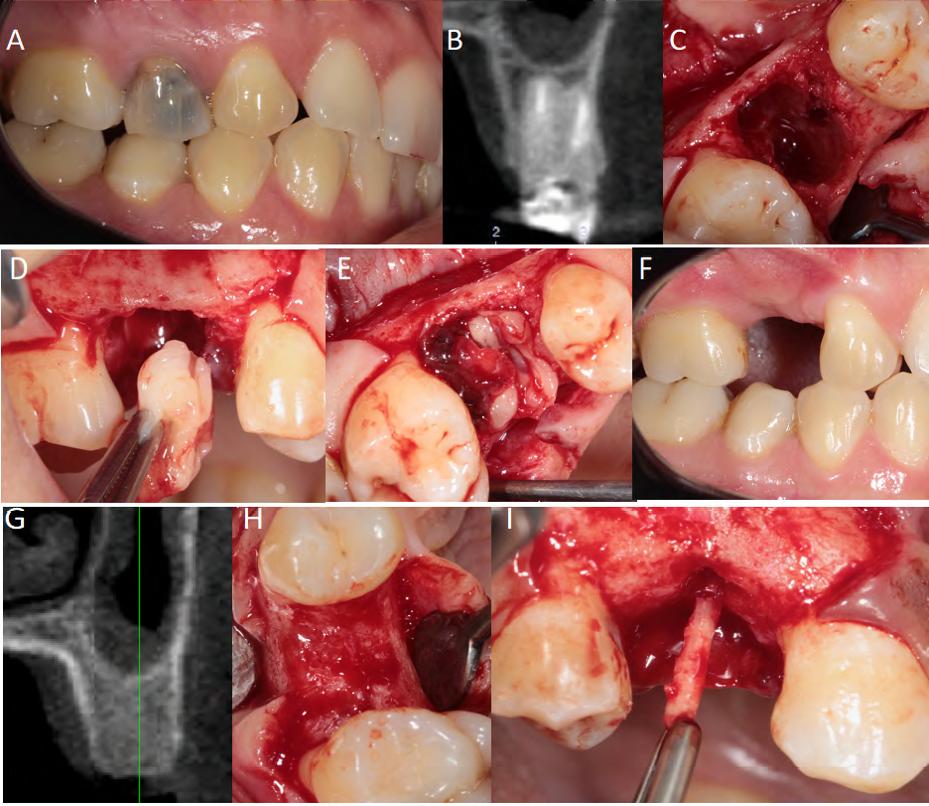
Fig. 1 Pre-, trans- and post-surgical sequence in G1 (PRF). (A) Tooth for removal, (B) initial tomography, (C) fresh socket, (D) insertion of PRF, (E)fiUing of the socket, (F) repair after 8 months, (G) final tomography, (H) repaired bone and (I) bone biopsy.
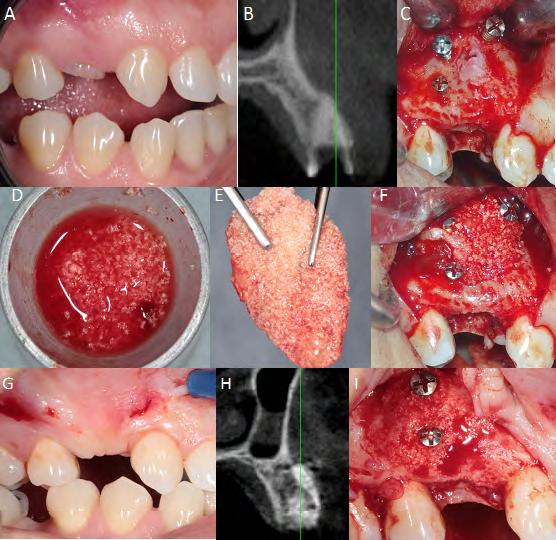
Fig. 2 Pre-, trans- andpost-surgical sequence in G2 (sticky bone). (A) Tooth for removal, (B) initial tomography, (C)fresh socket andpreparation of the surgical bed, (D) mixture of PRF and bioceramics, (E) sticky bone, (F) filling in the socket, (G) appearance after 8 months, (H) final tomography and (I) repaired bone.
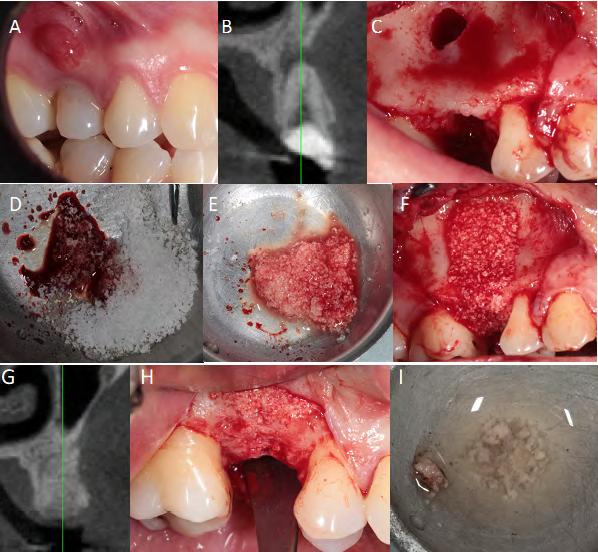
Fig. 3 Pre-, trans- andpost-surgical sequence in control (BCP). (A) Tooth for removal, (B) initial tomography, (C) fresh alveolus with periapical fenestration, (D) bioceramics with blood, (E) ready mix, (F) insertion of bioceramics, (G) final tomography, (H) repaired bone after 8 months and (I) bone biopsy.
Data collection
The second surgical access was performed after 8 months. Bone biopsies were performed with a 2mm diameter trephine drill (Maximus, Minas Gerais, Brazil) at a depth of 5mm. Then the metal implants were positioned as indicated by the manufacturer and suture performed on the mucosa. All patients continued to undergo clinical-prosthetic procedures in the following months to manufacture single implant-supported dental prostheses, which were not the subject of this study.
The bone biopsies collected were fixed in 10% formalin v/v (Allkimia, Brazil) buffered with phosphate buffer at pH 7.2 for 48h, washed in running water for 1h, decalcified in acid rapid bone demineralization solution (Allkimia, Brazil) for 36h, washed in running water for 1h, dehydrated in concentrations of 70%, 80%, 90% and 100% ethanol (Dinámica, Brazil) for 1h each, clarified in 3 xylol baths (Dinámica, Brazil) for 1h each, embedded in 3 baths of liquid paraffin at 60°C (Synth, Brazil) for 1h each. Blocks were prepared preserving the alveolar longitudinal topography or axial vertical axis of each biological sample. Paraffin blocks were sectioned in a rotating microtome (Leica RM2125 RTS, Germany), obtaining 3 histological slides per block. Sections had an individual thickness of 5gm and a 50pm distance between them to avoid overlapping counts. Slides were Haematoxylin-Eosin (HE) stained. Photomicrographs were taken using an optical microscope (FWL-1000; Feldman Wild Leitz, Manaus, Brazil). All images were qualitatively and quantitatively analyzed by an experienced pathologist and a previously trained researcher.
Histological and histomorphometric analysis
All histological slides were evaluated qualitatively for the presence of new bone, connective tissue, and remaining biomaterial in the different groups. The extension of the histological sections was evaluated, and images representative of the aforementioned biological criteria were selected.
For the histomorphometric analysis, 10 fields per section were evaluated in contiguous non-overlapping fields, at 800x magnification. Considering the biological samples collected from the 11 surgical beds of the patients and 3 stained slides for each paraffin block, a total 330 photomicrographs were taken and evaluated.
Images were segmented using the ImageJ 1.8.0 software (National Institutes of Health, USA), standardized for counting with an automatic grid of 140 points digitally superimposed on each photomicrograph, calibrated in micrometres/ pixel. The parameters evaluated by quantitative analysis were new bone (NB), connective tissue (CT), biomaterial (BCP) and other structures (OS) ( Fig. 4 ). From the number of absolute points, the percentage of volume density of each parameter was determined using Equation: %vd = (p/P)*100, where %vd represents the percentage of volume density; p the number of points of the parameter; and P the total number of points.
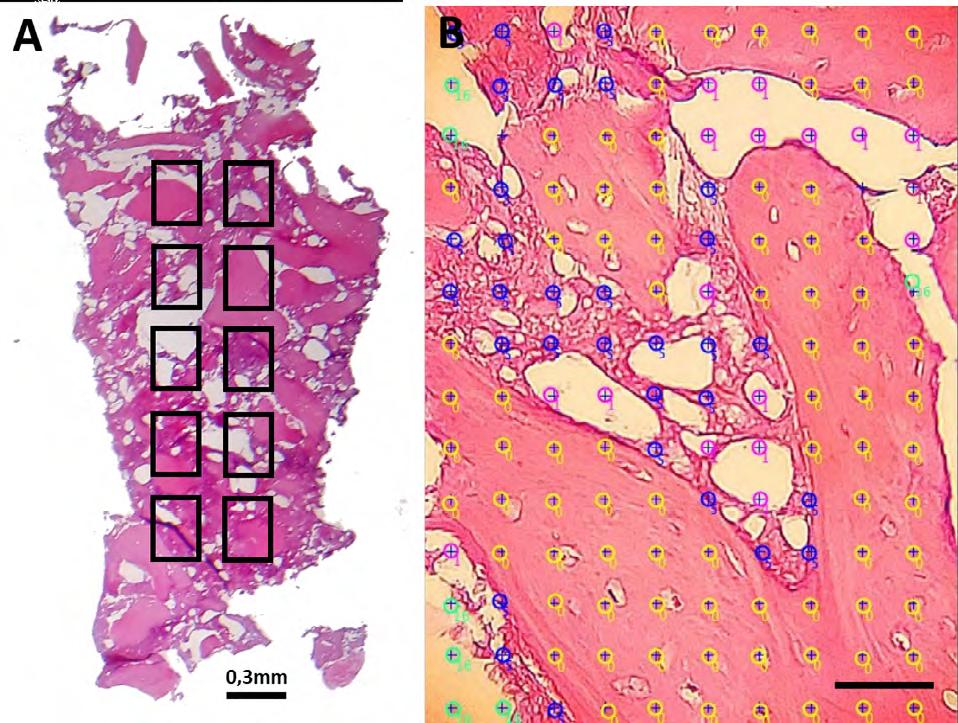
Fig. 4 Diagram of (A) stained slide of bone biopsy of G2 treat-ment and (B) histomorphometric counting of morphological criteria: new bone (yellow), connective tissue (dark blue), bio-material (purple) and other unrelated structures (green), scale bar: 50^m.
The data were tabulated and expressed through the mean ± standard deviation for each treatment. The results were displayed in graphs using the Graphpad Prism 7.0 software (Graphpad Software, USA), for comparing the intergroup biological response.
The parametric data of the mean density for each parameter were subjected to a one-way analysis of variance (ANOVA), and for the intergroup analyses, the Tukey post-test was applied comparing the difference between the means of the experimental groups considering significant differences with values of P<0.05. The Jarque-Bera test verified the normality of the research data of the 3 groups (P>0.05).
RESULTS
Fig. 5 shows the microscopio images of the experimental groups. In G1, there were large areas of new trabecular bone with osteocytes, and sometimes lamellar bone with Harversian canals, interspersed with connective tissue, without inflammatory infiltrate, fibrous capsule, or sign of the remaining PRF. In G2, bioceramic granules were present in varying sizes and in aggregates, surrounded by loose connective tissue or in close contact with new bone with osteocytes, proving their osteoconduction. In the control, the presence of connective tissue was greater, with little presence of new bone with osteocytes and some areas containing bioceramic granules, slightly more dispersed than in G2, which could be explained by the lack of agglutination due to absence of PRF.
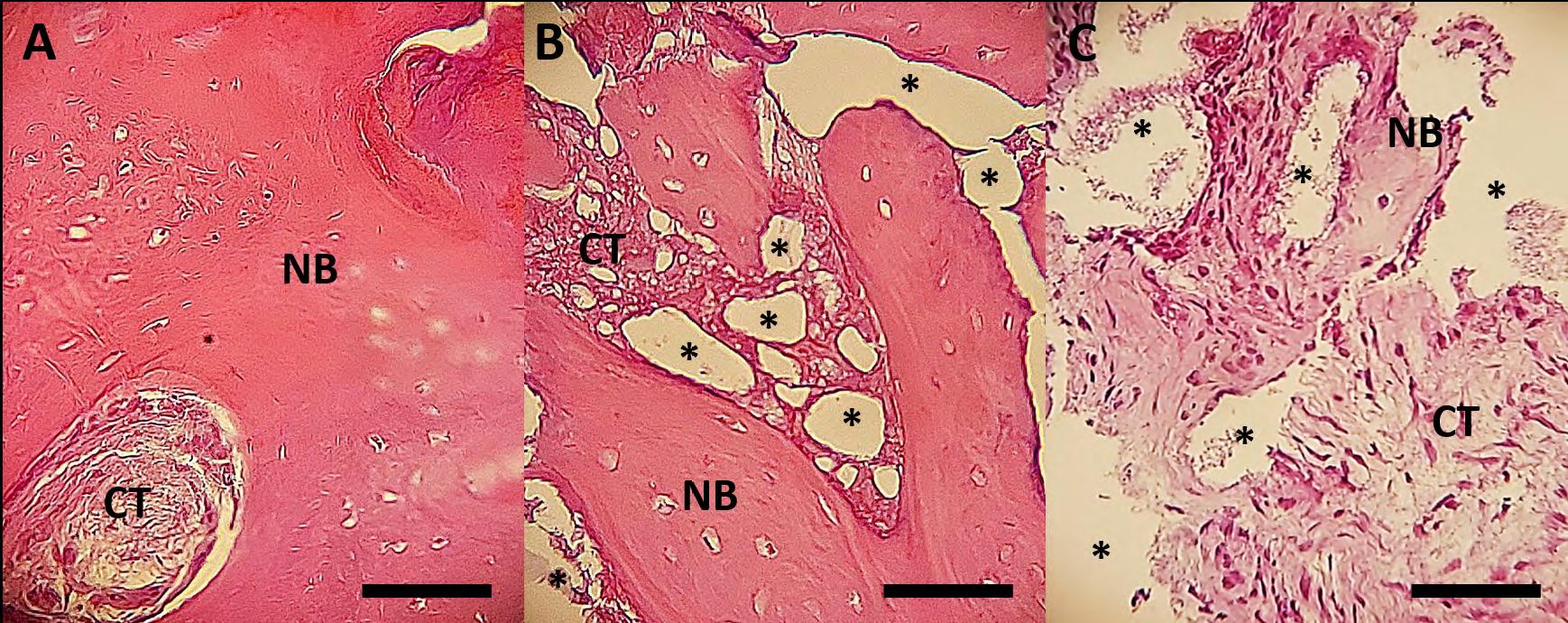
Fig. 5 Histological appearance of the experimental groups. (A) G1 (PRF), (B) G2 (sticky bone) and (C) Control (BCP). New bone (NB), connective tissue (CT) and biomaterial (*). Scale bar: 50 ¡xm.
Histomorphometric analysis showed a higher percentage of new bone in G1 (68.83%±4.95) than the control (16.28%±13.90) and G2 (35.69%±7.86). There are no differences between G2 and control. Connective tissue in the control group (61.56%±11.85) was greater than in G1 (13.95%±3.48) but without statistical differences for G2 (32.67%±13.69). The percentage of remaining biomaterial was higher in G2 (15.75%±11.63) than in G1 (undetectable PRF) but did not differ statistically from the control (8.43%±3.10). There were no statistically significant differences between groups regarding the presence of other structures (G1: 17.21%±5.53, G2: 13.73%±4.78 and control: 15.88%±7.06) ( Fig. 6 ).
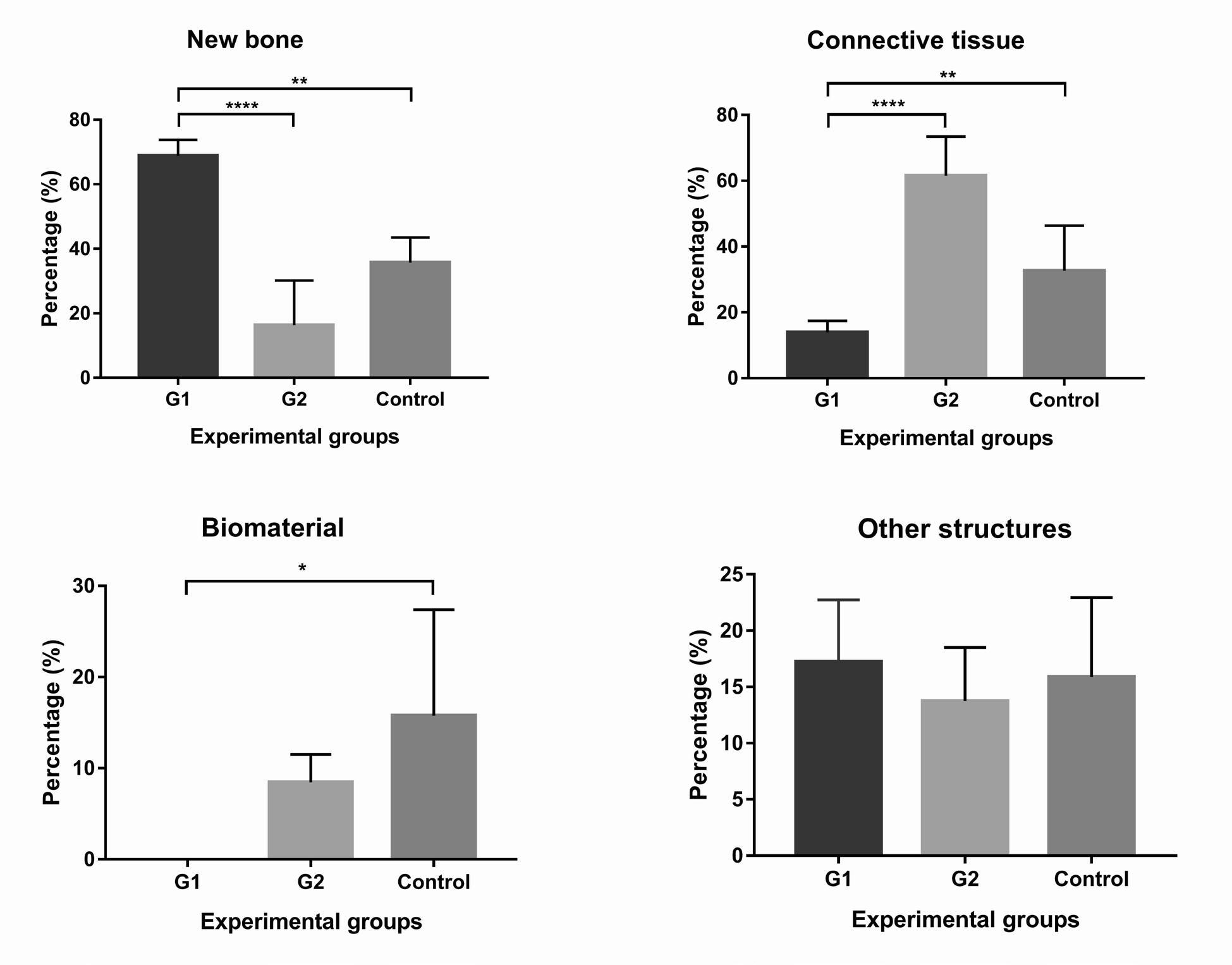
Fig. 6 Percentage of (A) new bone, (B) connective tissue, (C) graft remaining and (D) other unrelated structures in Gl, G2 and control after 8-month follow up. Means (± standard deviation) analyzed by the parametric ANOVA test and Tukey post-test. Signifi-cantdifferences between groupsfor new bone: P <0.01 (**) andP <0.0001 (****); connective tissue: P <0.01 (**) andP <0.0001 (****); and implanted biomaterial: P <0.05 (*).
DISCUSSION
For maintaining and potentially repairing alveolar bone structure, minimally invasive surgery is recommended that could provide a total flap to preserve periosteal vascularization and avoid reduction in the volume of the alveolus, the height of the bone crest and the keratinized gingival margin 16-18 . However, in the present study, a mucoperiosteal flap was performed for better surgical access in the use of PRF, and no negative influence on the clinical parameters was observed after 8 months. A study by Mendoza-Azpur et al. corroborated this option, reporting that dental alveoli treated with PRF and mucous covering after total flap and two diagonal relaxants presented the entire surgical site hermetically protected, promoting healing 19 . In addition, i-PRF generates more elasticity and better adaptation to defects, accelerating bone healing in the dental socket, preventing fibrogenesis and isolating the socket from the oral biofilm 19 , 20 . Centrifugation can interfere with the quality ofblood concentrates and generate heterogeneous results in bone healing 21 . Our protocol for obtaining PRF clot used a greater angle, radius and rotations per minute and shorter time, approaching half the angular speed of 408g used by Canellas et al. 21 , with centrifuge angled at 33 degrees, radius of 50 mm, 2700 rpm and action of 12 min. Choukroun et al. 22 evaluated the reduction in g-force in three protocols and concluded that low-speed centrifugation selectively precipitates leukocytes, platelets and growth factors, enriching the biological properties of PRF in tissue repair 22 , 23 . Centrifugation at 1400 rpm for 8 min could promote higher platelet concentration and antimicrobial activity and at 3500 rpm a denser fibrin network in PRF membranes in healthy adult patients 24 . Other studies also obtained larger PRF membranes using long spin time but reported no significant differences in PRF membrane sizes between patients aged 21-80 years 25 or dual presence of loose and dense fibrin networks in patients aged 21-60 years 26 , which confirms the methodology and sample used in this study.
The time for bone access and collection for histology corroborated the literature. Tooth removal promotes a process of intense bone remodelling in the dental socket from 3 months to 6 months after surgery 20 , 27 . Several surgical models for GBR have been proposed and the surgical reopening times in general ranged from 3 to 4 months, with few cases with 6, 8 or 9 months10-12,19,21,28. The option for the 8-month timing was also determined by the time to resorption of the alloplastic biomaterial, since studies report the presence of biomaterial at less than 8 months 13 . These data contribute significantly to the information available, which is scarce in long-term histomorphometric observations.
The percentage of new bone varies according to the time of analysis and type of treatment in a dental socket. Without grafting, there is low variation after 3 months: 37% 17 , 39.69%±11.13 21 , 45.4%±7.98 29 to 47.9%±18.1 28 . With grafting, in 3 months it varied from 20% with BioOss™ to 41% with carbonated HA 17 , reaching 51.6%±12.34 with Boneceramic™ 29 . In 4 months, P-TCP graft reached 26.14%±7.49 19 . In 6 months, the association of 30%HA:70%P-TCP to a collagen membrane reached 40.3%±7.8 30 . In 9 months, P-TCP/collagen composite reached 42.4%±14.6 alone and 45.3%±14.5 associated with membrane 11 . PRF graft alone reached an average of 50.7%±13.3 28 and 55.96%±11.97 21 in 3 months and 77.33%±9.8 in 4 months 19 , a percentage close to that found in the current study.
The lower percentage of connective tissue found with sticky bone than BCP alone could be explained by the intrinsic properties of the PRF. Fibrin promotes angiogenesis, increasing oxygenation and nutrition for cell proliferation and formation of extracellular matrix, favouring repair, and reducing inflammatory cell activity 10 .
The presence of biomaterials implanted in dental sockets is highly variable. According to different studies, after 3 months, PRF fragments were undetectable 19 , 21 28 , while carbonated HA had 1% remnants and BioOss™ was present in 22% of the area 17 . In 4 months, P-TCP reached 14.85%±6.4 19 . In 6 months, the association of 30%HA:70%P-TCP with collagen membrane reached 6%±4 30 . A composite of P-TCP/collagen remained at 9.7%±7.3 in 9 months and when associated with the membrane, increased its permanence to 12.5%±6.6 11 . These studies using HA 17 , P-TCP 11 , 19 or HA: P-TCP 30 corroborate the average percentages of BCP in fresh sockets from our findings. According to Mendoza et al. 19 , remaining granules may promote an inflammatory response, fibrogenesis or delay in alveolus osteogenesis. This reinforces the advantage of using BCP such as Boneceramic™, which kept few residual fragments, balancing the rate of resorption with tissue turnover. The promising potential of PRF in relation to bone neoformation is supported by scientific evidence 10 , 19 21 28 31 . The angiogenesis provided by PRF could explain the availability of key elements for the osteogenic microenvironment, including minerals, growth factors (e.g., VEGF, PDGF and TGFP1) and osteogenic cells 32 , 33 . Furthermore, miRNA released from platelet microparticles could play a central role in regulating osteogenic phenotype in vitro 34 . Despite the use of PRF to improve soft tissue healing and reduce pain, bleeding and osteitis, there is no definitive evidence for the impact of using PRF alone on bone regeneration in post-extraction sockets 6 , 35 , making the present results unprecedented and relevant for future studies on this topic. It is important to note that many studies on fibrin in alveoli after extraction do not report quantitative results regarding bone formation
and the presence of connective tissue16,18,20,27,31,36,
which makes histomorphometry a more accurate analysis tool and strengthens scientific evidence. Use of fibrin associated with P-TCP in sinus lift, a different site from the one used in this study, showed bone neoformation with a 6-month percentage of 33.40%±10.43 for P-TCP and 32.03%±6.34 for the P-TCP associated with fibrin, thus confirming that the association of P-TCP with fibrin would not differ substantially from the alloplastic biomaterial alone 37 , as in the present study.
The BCP used in the research shows biocompatibility and osteoconductive potential, favouring the adhesion, proliferation and differentiation of bone cells and the production of mineralized matrix 29 . However, the higher HA content may explain the low bioactivity and slow biodegradation 38 . Still,
BCP present in irregular shapes collaborates with an inflammatory response that acts in the negative immunomodulation for osteoconduction 17 . Thus, the appropriate selection of a biomaterial must consider topography, particle size, crystallinity, composition, and porosity, among other physicochemical characteristics that affect tissue repair 39 .
The present study demonstrated that the autologous PRF is promising for GBR procedures in post-extraction socket. The association of PRF with a BCP proved to be beneficial, but less effective than the isolated form. Future studies with greater clinical samples and an emphasis on morphological quantifications are recommended.

