











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Similars in
SciELO
Similars in
SciELO 
 Permalink
Permalink
INTRODUCTION
Root canal morphology and its anatomical variations pose a great challenge to endodontists 1 . Although success rates for endodontic treatments are generally high, cases of failure have been attributed to lack of knowledge of root canal internal anatomy 2 , the understanding of which is essential for performing effective endodontic treatments and ensuring proper cleaning and disinfection. Some of the most common teeth requiring endodontic treatment are mandibular first molars because emerge at about six years of age in the oral cavity and are more exposed to endodontic treatment 3 . They present diverse anatomy and configuration, with the mesial root being particularly complex due to the presence of isthmuses 4 . Isthmuses are anatomical variations found in roots with two canals, primarily in the mesial roots of mandibular and maxillary first molars. The incidence of isthmuses is particularly high in mesial roots of mandibular molars 5 . Larger isthmuses, especially in mandibular molars, may harbor necrotic debris, pulp remnants, or organic matter that promotes microbial growth. This may interfere with proper cleaning and disinfection of the root canal system 6 and lead to endodontic treatment failure 7 .
Accurate morphological mapping of the root canal system is essential to achieve the best possible outcome during endodontic therapy. Micro-CT has been used for in vitro and ex vivo morphological evaluations based on qualitative and quantitative three-dimensional images, and is considered the gold standard in endodontics 8, 9 . It is an advanced method that reveals the internal anatomy of root canal systems through high-resolution images 10 . Numerous studies have been performed to classify the morphology of mesial root canals. A classic study that has undergone modifications over the years is Vertucci’s classification 11-15 . The classification of isthmuses was established by Fan et al. 5 , who identified different shapes such as foliar, separated, mixed, and cannular. In addition, a ribbon-shaped isthmus was described as an oval junction formed between two merging and then dividing root canals, with its own isthmus roof and floor 16. The current study adopted Fan’s classification for isthmuses.
The aim ofthis ex vivo study was to analyze the three-dimensional (3D) morphological characteristics of isthmuses in mesial root canals of mandibular molars using micro-CT. This approach enabled us to make both qualitative and quantitative assessments of the isthmus structures.
MATERIALS AND METHOD
This project was approved by the local research ethics committee (Igua^u University Research Ethics Committee’s approval N° 3.422.230). Six hundred extracted mandibular first molars with straight or curved mesial roots were selected from the Igua^u University’s institutional tooth bank. Criteria were met in 317 teeth that had two single mesial canals with isthmuses present between them and complete root formation. Isthmus morphology was determined in 3D longitudinal images. Root length, volume and total area of the root canal, as well as of the apical and coronal level, volume and area of the isthmus, and structural model index (SMI) were analyzed.
Morphometric analysis
Samples were scanned using a micro-scanner CT (Skyscan 1174v2; Bruker micro-CT, Kontich, Belgium), and reconstructed for 3D evaluation of the area, volume, and surface of the root canals using the software CTan V.1.14.4.1 (Bruker micro-CT, Kontich, Belgium) for qualitative evaluation of the canal configuration analyses. The first assessment is the isthmus morphology according Fan’s 5 classification, in which the Type I, is the sheet connection: narrow sheet and complete connection existing between 2 canals from the top to bottom of the isthmus. In some cases, 1 or more small dentin fusions were discerned in the isthmus area. Type II, separate is the narrow but incomplete connection existing between 2 canals from the top to bottom of the isthmus. Type III, mixed: incomplete isthmus existing above and/or below a complete isthmus. Type IV, cannular connection: narrow cannular communication between 2 canals 5 .
The specimens were analyzed through the longitudinal aspect using the CTan V.1.14.4.1 sotware (Bruker micro-CT) to assess the following aspects of the mesial roots: root length, apical level, coronal level, volume and total area of the pulp cavity, volume and area of the isthmus, and structural model index (SMI) analysis.
On the longitudinal sections, the measure tool option was used to measure from the cervical and apical portions to determine root length, distance from the isthmus to the apex of the mesial roots and also to determine the distance from the isthmus (mm) to the cervical part of the mesial roots, and also to identify the presence of an isthmus.
Volume and total area of the pulp cavity and isthmus
With the top and bottom root dimensions already determined, the volume and total area of the pulp cavity were evaluated using the Region of Interest tool (ROI). Then, the binary selection tool was used to preview the selected area, observing the histogram bar to obtain two colors: white for solid parts and black for empty parts. Then, the Morphometry tool was used to perform a 3D analysis. The Data were calculated, and the values were automatically obtained by the software.
SMI analysis
The SMI indicates the relative prevalence of regions of trabecular bone and plaques in a 3D model. Total volume and area as well as the volume and area of the isthmuses were obtained from 3D analyses. These measurements were made separately by two calibrated evaluators. 5 Any cases in which measurements differed between evaluators were analyzed by a third evaluator. At the end of the evaluation, the kappa coefficient (k) was used to analyze the agreement between them.
RESULTS
The morphological analysis data of mesial roots in first mandibular first molars showed that root mean root length was 9.1±0.5 mm. The volume and area, of all root canal system, were 41.8±40.1 mm3 and 63.6±24.2 mm2 respectively. The isthmi volume and area alone were 11,0.6±9,03 mm3 and 30,02±11,02 mm2 (Table 1).
Table 1 Morphometric analysis of mesial roots of mandibular first molars in the study.
| Parameter | Mean ± SD | Range |
|---|---|---|
| Total Root Length | 9.1±0.5 | 14.3-5.3 |
| Total Volume of Pulp Cavity | 41.8±40.1 | 74.9-20.7 |
| Total Area of Pulp Cavity | 63.6±24.2 | 141-35.7 |
| Isthmus Volume | 11.6±9.3 | 17.3-0.96 |
| Isthmus Area | 30.2±11.2 | 124-2.7 |
| Canal SMI | 1.7±0.7 | 2.9-1.55 |
| Isthmus SMI | 2.2±0.8 | 2.8-0.3 |
Micro-CT analysis of the 317 cases identified isthmuses showed higher prevalence in the apical third, especially between 3 and 5 mm from the apex. The distribution of isthmus types and their respective prevalence rates were as follows: Type I - 17%, Type II - 32%, Type III - 29%, and Type IV - 22%, showing separate type and mixed types (Figs. 1 and 2).
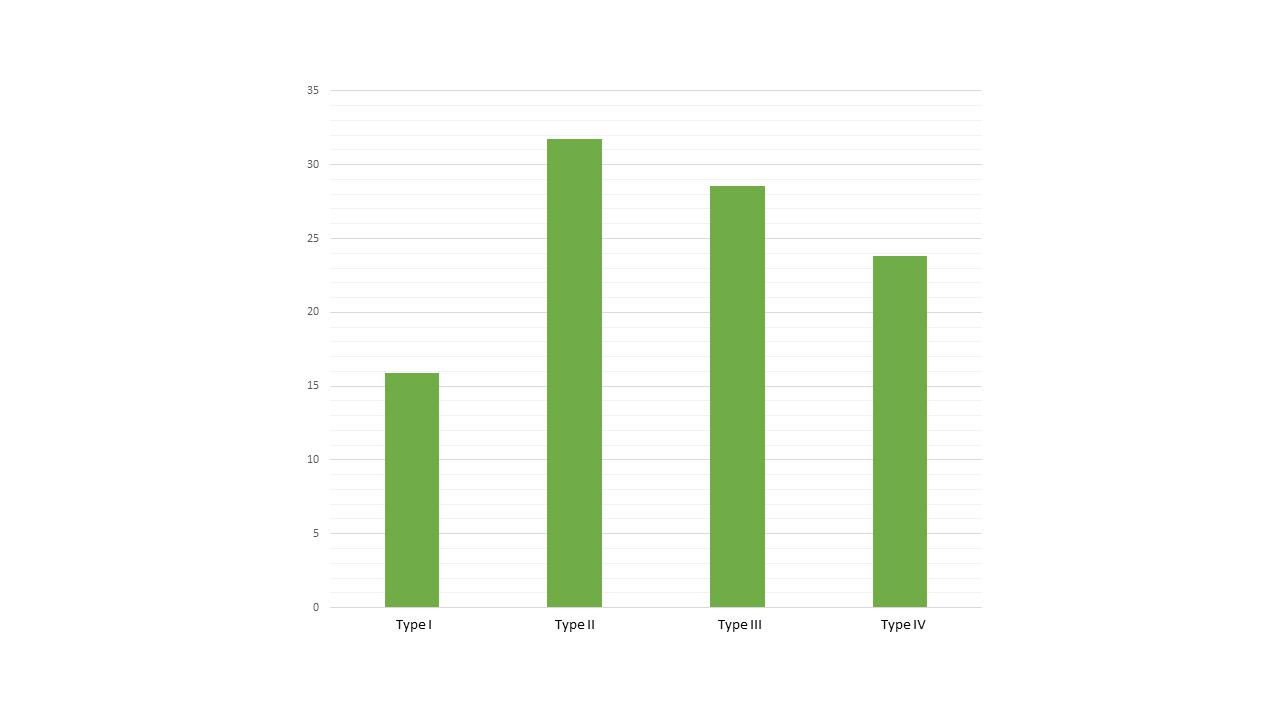
Fig. 1 Isthmus prevalence found in mesial roots of mandibular molars according to Fan et al. 5 classification.

Fig. 2 Representative images of Fan ’s isthmus types found in mandibular molars assessed in the present study.
Mean SMI of the studied isthmuses was 1.7 mm, close to 0, which is a flat format. A value of 2.2 mm was determined for canal SMI, indicating a more cylindrical shape (values close to 3 indicate cylindrical) (Table 1)
DISCUSSION
The mandibular first molars assessed in this study show the expected dominance of two mesial and one distal canal, which is consistent with previous reports 4, 17 . The mesial roots were used in this study because of their complexity and frequent connections between canals 7 .
The apical third of the root is a critical area in endodontic treatment because of the presence of ramifications that can serve as bacterial reservoirs 18 . Other complexities along the canal may also exist in this risk area, contributing to treatment failure 19 . Therefore, the aim of this study was to evalúate complexities of the root canal isthmi from mandibular molars, using micro-CT.
Isthmus prevalence ranges from 10% 20 to 100% 21 , and may be age-related, as it seems to be higher in the younger than in elderly age groups 7 . An isthmus may occur anywhere along the root, though they are more common in the middle and apical thirds of the mesial roots of mandibular molars 22-24 . The current study found high incidence of isthmuses along the root canal system, especially in the apical third 4 , which is consistent with a study that found isthmuses within 3-5 mm from the apical foramen of maxillary and mandibular molars 25 .
In line with other studies 5,7, 26 , our findings showed that Type II was slightly more common than other types in mandibular first molars. This highlights the importance of using intracanal medications for disinfection in areas not reached by the instruments. These findings are consistent with studies conducted on Turks 27 and Iranians 28 , but contradicts results reported on Yemenis 29 and Venezuelans 30 .
A systematic review has shown that anatomical variability in mandibular molars can be attributed to population differences, different methods of analysis, inclusion and exclusion criteria, and sample sizes 8 . The most frequently found root canal isthmus configuration is Vertucci type IV 23, 26 , which is described as two independent canals. This configuration is the most common in Egyptians 31 . Many methods such as clearing techniques, micro-CT and CBCT can be employed to assess root canal anatomy 32 . Micro-CT has been used as an advanced research tool to assess the ex vivo anatomy of root canals due to its high-resolution and ability to preserve the specimens 33 . Despite its limited clinical applicability, micro-CT has become established as the reference method for ex vivo studies of root canal anatomy. Its adoption facilitates future comparisons and continuous improvements of the exploration of root canal structures 33.
Regarding morphological analysis of mesial roots in first mandibular first molars, the results showed that root mean root length was 9.1±0.5 mm, similar
to other studies 5,7,23,24, 34 . The volume and area, of
all root canal system, were 41.8±40.1 mm3 and 63.6±24.2 mm2 respectively, in accordance to previous studies 12,13,20, 23 . The isthmi volume and area alone were 11.6±9,.3 mm3 and 30.2±11.2 mm 2 22, 24 (Table 1).
This study identified some limitations, including the lack of information on age and gender of the patients from whom teeth had been extracted, potentially affecting the generalizability of the findings.
In conclusion, this study confirms the presence of isthmuses in the mesial canals of mandibular first molars, with higher frequency in the apical third. Although the present study was conducted ex vivo, its clinical implications highlight the significance of carefully selecting an appropriate root canal disinfection protocol to achieve a higher success rate in the treatment of mandibular first molars. Based on that findings, important to consider their complex anatomy and difficult-to-access areas during endodontic treatment 34, 39-41 .
It has been shown that there is an association between untreated canals and isthmuses and apical periodontitis 34-37 , so, regardless of whether an isthmus is detected, it is recommended to improve the irrigation of all root canal system in these areas as well 36,38,40, 41 . Micro-computed tomography is the gold standard for research of root canal anatomy because it provides nondestructive three-dimensional microscopy data with high spatial resolution that enables accurate assessment of morphological features. Knowledge of anatomical features such as lateral canals and isthmuses is important to guide clinical protocols to ensure adequate disinfection and contribute to the healing of periradicular tissues 34, 38 . However, micro-computed tomography has hardly any clinical value and can only be used for in vitro and ex vivo studies 35-37 .
For clinical practice, preoperative Cone Beam Computed Tomography (CBCT) scanning may play a significant role in revealing complex anatomy 39-41 . CBCT settings include multiple FOVs and voxel sizes that can better address a variety of specific tasks 40, 41 . However, CBCT imaging cannot detect and measure apical isthmus length accurately, even with the highest-resolution settings. This highlights the importance of efficient, rigorous endodontic cleaning, even when such variations are not detected in CBCT exams 39 .

