Casuística
Primary Membranous Nephropathy With Extremely High Levels Of Ca-125
Nefropatía Membranosa Primaria Con Niveles Extremadamente Altos De Ca-125
1Department of Nephrology, Yenimahalle Research and Training Hospital, YıldırımBeyazit University, Ankara, Turkey
Abstract
Membranous nephropathy is a glomerular disease that causes nephrotic syndrome. Absent phospholipase A2 receptor antibodies and absent staining with IgG4 may be linked to malignancy-associated MN. Here we present a case that defies that suggestion.
A 42-year-old female presented with anasarca. Kidney biopsy revealed membranous nephropathy, stained positive for IgG but negative for IgG4. Absent phospholipase A2 receptor antibodies was negative. Abdominal tomography revealed a partial thrombosis of the left ovarian vein which raised suspicion for ovarian cancer. Even though her ovaries did not uptake FDG on PET scan, a carbohydrate antigen-125 was ordered. She had extremely high levels of carbohydrate antigen-125 which was unexpected in the course of benign events.
Thorax CT, endoscopy, colonoscopy, mammography, and positron emission tomography were clear in terms of malignancy. Samples from both pleural effusion and ascites were consistent with transudate. Tuberculosis tests were negative. Cytology samples were negative for malign cells. Exploratory surgery was planned but rejected by the patient.
She was treated as primary disease with cyclosporine and methylprednisolone. Rituximab was off-limits due to insurance rules. She had prompt and excellent response. Steroids were tapered and stopped at sixth month and cyclosporine at twelfth month. In her 36 months of drug-free follow up there has been no disease recurrence or a sign of cancer.
Even when all odds are towards malignancy-associated membranous nephropathy, primary disease is still a possibility. We need better markers for malignancy-associated membranous nephropathy.A very high level of CA-125 does not necessarily mean cancer.
Keywords: membranous nephropathy; membranous glomerulopathy; phospholipaseA2 receptor antibodies; anti-PLA2R; malignancy; carbohydrate antigen; cancer
Resumen
La nefropatía membranosa es una enfermedad glomerular que causa el síndrome nefrótico. La ausencia de anticuerpos contra el receptor de fosfolipasa A2 y de tinción para IgG4 puede deberse a una nefropatía membranosa asociada a cáncer. A continuación, se presenta un caso que desafía esta sugerencia.
Una paciente de 42 años realizó una consulta por anasarca. A partir de la biopsia de riñón, se diagnosticó nefropatía membranosa con tinción positiva para IgG, pero negativa para IgG4. No se detectó la presencia de anticuerpos contra el receptor de fosfolipasa A2. La tomografía abdominal reveló una trombosis parcial en la vena ovárica izquierda, lo cual generó sospecha de cáncer de ovario. Si bien los ovarios no mostraron absorción de FDG en la tomografía por emisión de positrones, se solicitó una prueba de antígeno carbohidrato 125. Se le detectaron niveles elevados del antígeno carbohidrato 125, lo cual no es esperable en casos de eventos benignos.
La tomografía computarizada de tórax, endoscopía, colonoscopía, mamografía y tomografía por emisión de positrones no mostraron tumores. Las muestras de derrame pleural y de ascitis fueron indicativas de trasudado. Las pruebas de tuberculosisarrojaron resultados negativos. El examen citológico fue negativo para células malignas. Se sugirió una cirugía exploradora, pero la paciente no aceptó. Se la trató con ciclosporina y metilprednisolona por enfermedad primaria. No se utilizó rituximab por reglas de su cobertura médica. La paciente tuvo una excelente respuesta al tratamiento de forma rápida. Los esteroides se disminuyeron de forma progresiva y se suspendieron a los seis meses, y la ciclosporina, a los doce meses. Durante los 36 meses de seguimiento sin medicación no ha habido recidiva ni signos de cáncer.
Incluso cuando existen grandes probabilidades de que se trate de una nefropatía membranosa asociada a cáncer, aún es posible que se trate de una enfermedad primaria. Es necesario contar con mejores marcadores de nefropatía membranosa asociada a cáncer. Un nivel elevado de CA-125 no necesariamente es indicador de cáncer.
Palabras Clave: nefropatía membranosa; glomerulopatía membranosa; anticuerpos del receptor de fosfolipasa A2; anti-PLA2R; malignidad; antígeno de carbohidrato; cáncer
Introduction
Membranous nephropathy (MN) is a primary glomerular disease that causes nephrotic syndrome in adults. Its association with certain malign disorders is well known and much feared.1 World of nephrology is in pursuit of a clinical, laboratoryor pathological marker to define patients with a high risk of malignancy for decades. Recent reports suggest absent phospholipase A2 receptor antibodies (anti-PLA2R) and absent staining for IgG subclass -IgG4- are linked to malignancy-associated MN.(2-3) Here we present a case that defies that suggestion. Her serum was negative for anti-PLA2R. Her biopsy stained positive for IgG but negative for IgG4 and she had very high levels of carbohydrate antigen (CA-125), yet her disease turned out to be primary MN with an excellent response to immunosuppression.
Case Report
A 42-year-old female presented with anasarca. She had marked swelling of lower extremities and severe ascites. Breath sounds were absent at bases of lungs. Her creatinine was 0.7 mg/dl with proteinuria level of 8300 mg/day; simultaneous albumin was 1.6 mg/dl. Chest X-ray revealed massive pleural effusion. A kidney biopsy revealed MN with negative staining for IgG4 but positive staining for IgG. Anti-PLA2R was not detected in her serum. These findings suggested a secondary cause for MN. Hepatitis B and C serology were negative. Her medication history was unremarkable. She did not have any exposure to heavy metals. The gynecologic examination was normal. Transvaginal sonography revealed a homogenously and slightly enlarged left ovary. Abdominal computed tomography (CT) was negative for any gynecologic mass lesion. However, partial thrombosis of the left ovarian vein was observed. These gynecological findings rose a suspicion of an ovarian tumor. CA-125 was ordered. Her CA-125 level was 2892 IU/mL, which was extremely high (Normal: 0-35). Thorax CT, endoscopy, colonoscopy, mammography, and positron emission tomography were negatives
in terms of malignancy. Samples from both pleural effusion and ascites were consistent with transudate. Tuberculosis (TB) tests were negative. Cytology samples were negative for malign cells. Explorative laparoscopy for an ovarian tumor was planned, but the patient refused the surgery.
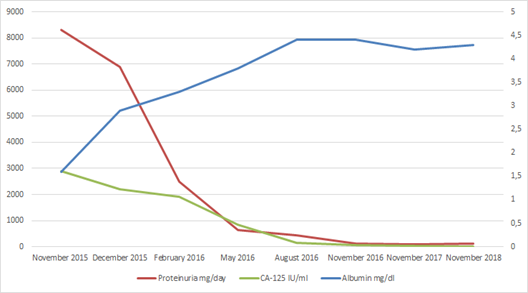
We had to attribute her extremely high CA-125 levels to ascites plus pleural effusion and decided to treat her disease as primary MN since no secondary cause could be established. Dual treatment with methylprednisolone (MPZ) and cyclosporine (CsA) was initiated as per KDIGO guideline recommendations.(4) Heparin and warfarin were used for anticoagulation. Diuretics were used as indicated. She had a prompt and excellent response. She achieved complete remission. MPZ was tapered and stopped at 6th month and CsA at the 12th month. Concurrently with her decreasing proteinuria, serum albumin increased, ascites and effusions disappeared, and CA-125 levels normalized (Figure 1). She is now under 48 months of total and 36 months of drug-free follow-up and has neither experienced a relapse nor shown any sign malignancy.
Discussion
Antibodies directed to phospholipase A2 receptor on podocyte surface are responsible for 70% of primary MN cases.(2) Though initially they were considered exclusive for primary MN, studies have shown they can be positive in secondary MN, especially hepatitis B related disease. Current evidence warrants a vigorous search of malignancy in the absence of anti-PLA2R.(2-3)
Her kidney samples stained strongly positive for IgG but negative for IgG4. Stains for IgG1-3 were not available. Aggressive evaluation for malignancy is advised for patients with such staining pattern.(2-3) However, IgG subclasses may not always differentiate between primary or secondary forms of MN. Co-dominant staining, subclass switch between early and late disease and methodological differences in studies may explain this phenomenon.(5)
Anti-PLA2R test we employed was an immunofluorescence assay (IFA), which has very low false negativity.(2) We did not have access to enzyme-linked immunosorbent assay (ELISA), but most likely, it would also be negative in our case. ELISA testing is vital in subjects when anti-PLA2R is positive. For example, spontaneously decreasing low titers foresee spontaneous remissions whereas very high titers predict poor renal outcomes. Anti-PLA2R ELISA and titer surveillance may also be used in tailoring the treatment.(6-7)
Anti-thrombospondin type 1 domain-containing 7A (THSD7A) antibody-induced MN, is a newer clinical entity. Clinical series suggest anti-THSD7A antibodies are responsible for 3-5 %of MN cases and seem to be associated with cancer, unlike anti-PLA2R.(8) There are reports of tumoral THSD7A positivity and MN. Dual positivity with anti-PLA2R has also been observed. Both antibodies are mostly of IgG4 type and activate complement via mannose-binding-lectin (MBL) aka alternative pathway, which implicates a role of complement inhibition in treatment of MN. Disappointingly, clinical studies have not been able to demonstrate a favorable change in renal outcomes.(9)
As for our case, we were not able to measure anti-THSD7A levels. Since IgG4 stain was negative, we have three acceptable antigens responsible for our patient’s MN: a) a non-IgG4 anti-PLA2R; b) a non-IgG4 anti-THSD7A; c) an undetected/unknown antigen. For the latest, antibodies directed against superoxide dismutase, α-enolase, aldose reductase or other antigens might be the culprits.(10) However, these antibodies have not been standardized for clinical care and remain mostly for research purposes.
In addition to multiple diagnostic modalities, the level of CA-125 was obtained as a part of the gynecological workup. CA-125 is a carbohydrate antigen notoriously related to certain cancers, most importantly, ovarian cancer and very high levels defined as > 1000 IU/ml are highly specific for ovarian cancer.(11) Other causes of elevated CA-125 levels include benign lesions of ovaries, peritonitis, peritoneal TB, cirrhosis, ascites of any etiology, pleural effusions, chronic lung disease, heart failure and abdominal surgery.(12) A single case of MN with high CA-125 levels was reported but in that instance patient’s CA-125 was only mildly elevated (278) and like our patient she had a favorable response to immunosuppressive treatment.(13)
In our case, with a lack of identifiable cancer, we had to attribute her CA-125 levels to ascites and pleural effusion. We wish we could employ rituximab in her treatment since chances of success are better in the light of recent publications.(14) Unfortunately insurance rules necessitated we treat her with cyclosporine and methylprednisolone first. Much to our joy she had a prompt and excellent response. After twelve months of treatment ending with a slow taper of cyclosporine. She has not experienced a relapse nor show any sign of malignant disease in 36 months of drug-free follow-up.
Conclusion
Value of negative anti-PLA2R is questionable in predicting secondary MN. Ascites, combined with pleural effusion, may cause very high CA-125 levels. Even when all odds are towards malignancy-associated MN, primary disease is still a possibility.
Bibliography
1 )CattranD, BrenchleyP.Membranous nephropathy: thinking through the therapeutic options. Nephrol Dial Transplant.2017;32(suppl1):i22-i29.
[ Links ]
2 ) De VrieseAS, GlassockRJ, NathKA, SethiS, FervenzaFC.A proposal for a serology-based approach to membranous nephropathy. J Am SocNephrol. 2017;28(2):421-30.
[ Links ]
3 ) QuZ, LiuG, LiJ, WuLH, TanY, ZhengX, et al.Absence of glomerular IgG4 deposition in patients with membranous nephropathy may indicate malignancy. Nephrol Dial Transplant.2012;27(5):1931-7.
[ Links ]
4 ) Kidney Disease: Improving Global Outcomes (KDIGO), Glomerulonephritis Work Group. KDIGO Clinical Practice Guideline for Glomerulonephritis.Kidney Int Suppl. 2012;2(2):139-274.
[ Links ]
5 ) MurtasC, GhiggeriGM.Membranous glomerulonephritis: histological and serological features to differentiate cancer-related and non-related forms.J Nephrol.2016;29(4):469-78.
[ Links ]
6 ) BombackAS, FervenzaFC.Membranous nephropathy: approaches to treatment. Am J Nephrol.2018;47(Suppl1):30-42.
[ Links ]
7 ) CouserWG.Primary membranous nephropathy. ClinJ Am SocNephrol. 2017;12(6):983-997.
[ Links ]
8 ) RenS, WuC, ZhangY, WangAY, LiG, WangL, HongD.An update on clinical significance of use of THSD7A in diagnosing idiopathic membranous nephropathy: a systematic review and meta-analysis of THSD7A in IMN.Ren Fail. 2018;40(1):306-13.
[ Links ]
9 ) CattranDC, BrenchleyPE.Membranous nephropathy: integrating basic science into improved clinical management.Kidney Int.2017;91(3):566-74.
[ Links ]
10 ) SinicoRA, MezzinaN, TrezziB, GhiggeriGM, RadiceA.Immunology ofmembranous nephropathy: from animal models to humans. ClinExpImmunol.2016;183(2):157-65.
[ Links ]
11 ) MossEL, HollingworthJ, ReynoldsTM.The role of CA125 in clinical practice. J ClinPathol.2005;58(3):308-12.
[ Links ]
12 )SikarisKA.CA125--a test with a change of heart. Heart Lung Circ. 2011;20(10):634-40.
[ Links ]
13 ) AltunB, ErdemY, OymakO, YasavulU, TurganC, CağlarS.A case of membranous glomerulonephritis with elevated serum level of CA-125. ClinNephrol.1995;44(4):277-8.
[ Links ]
14 ) FervenzaFC, AppelGB, BarbourSJ, RovinBH, LafayetteRA, AslamN, et al. MENTOR Investigators. Rituximab or Cyclosporine in the Treatment of Membranous Nephropathy. N Engl J Med. 2019 ;381(1):36-46
[ Links ]












 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Similars in
SciELO
Similars in
SciELO 
 Permalink
Permalink