











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Similars in
SciELO
Similars in
SciELO 
 Permalink
PermalinkINTRODUCTION
The shortage of deceased donor kidneys for transplantation has forced the re-evaluation of the limits on donor age acceptability. Thus, marginal donors such as elderly donors have been progressively increasing in recent years for organ transplantation around the world.1-2 Many studies show that elderly donors more frequently present risk factors for the development of chronic allograft nephropathy (CAN): have a higher incidence of delayed renal function, susceptibility to calcineurin caused nephrotoxicity, arterial hypertension and loss of functional renal reserve. All these factors above, associated with the elderly age of the donors contribute worse long-term outcome.(2-6)
Here in this study, we evaluated of both deceased and living donor kidney transplantation outcomes of 55 years old and older donors. It was aimed to contribute to the elimination of question marks about using elderly donors for kidney transplantation.
MATERIAL AND METHODS
Patients and evaluation process
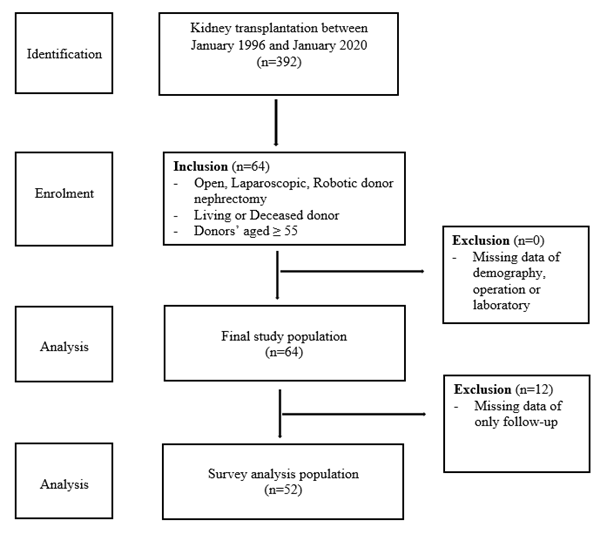
In this retrospective cohort study, prospectively recorded data of patients who underwent kidney transplantation between January 1996 and January 2020 were evaluated. Donor nephrectomies were performed by a group of transplantation surgeons in the same unit. The inclusion criteria for the study were; deceased or living donor, donor age 55 years and older. Exclusion criteria were; failure to reach data of demography, operation or laboratory. (Figure 1)
Screening of our potential living kidney donors has been described thoroughly.(7)Absolute contraindications for donation are body mass index >35 kg/m2, GFR <80 ml/min, hypertension with end‐organ damage, history of invasive malignancies, diabetes mellitus, pregnancy, intravenous drug abuse, major cardio respiratory disease, human immunodeficiency virus positivity, hepatitis B or C infection, psychiatric disorders, and systemic disease. But living kidney donor age itself has never been a contraindication for donation. In our center deceased donor kidneys are accepted only from heart beating donors. Depends on deceased donor medical history, pre-transplantation graft kidney biopsy can be performed.
The immunosuppressive protocol consisted of induction therapy; (Simulect 20 mg postoperative day 0 and 4) and triple immunosuppressive (calcineurin inhibitors, mycophenolic acid (MMF) and steroids). Standard immunosuppression was prednisone, cyclosporine (CsA), and MMF until 2003. After 2003, Tacrolimus became available in the Turkey and been introduced as substitute for cyclosporine therefore it was changed to tacrolimus. In deceased donors, Anti-Thymocyte Globulin (ATG) was used when delayed functioning graft (DGF) occurred. It was used until the serum creatinine decreased to 3 mg/dL.
The demographics (age and gender), donor type (living or deceased), the relationship between the recipient and donor in living donors, causes of death and medical history in deceaseddonors, surgical approach (open, laparoscopic or robotic donor nephrectomy), surgical complications according to Clavien-Dindo Classification,(8) warm ischemia time (WIT), cold ischemia time (CIT), HLA mismatch, length of stay, length of stay in intensive care unit for deceased donors, follow-up time, preoperative (last 24 hours), postoperative (first 24 hours) and on the day of discharge serum creatinine levels and mortality were recorded.
Statistical Analysis
All data were transferred to computer environment and SPSS 20.0 software (SPSS Inc., Chicago, IL, USA) was used for statistical analysis. Categorical measurements were given as number and percentage, while continuous measurements were given as mean ± standard deviation, median and range. Relevant variables were analyzed using descriptive statistics. Non-parametric Kaplan-Meier survival estimator was used for survey analysis.
Ethics Committee Approval
All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee and the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. This study was approved by the local ethical committee (reference no:13.07.2020/461).
RESULTS
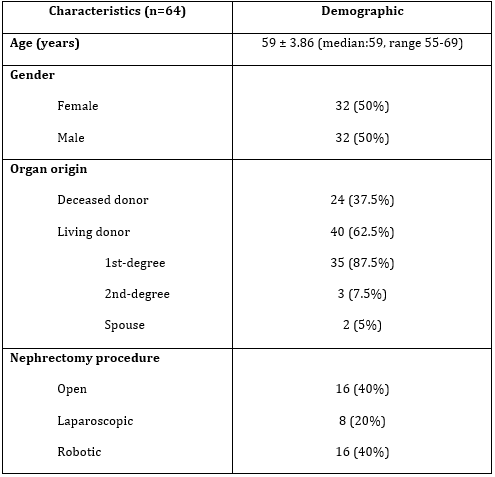
Of the total 392 kidney transplantation, 64 donors (16.3%) met the study criteria. The mean age of the donors was 59 ± 3.86 years (median 59 years, range 55-69 years). Of these 64 donors, 32 (50%) were female and 32 (50%) were male. The living donors were 40 (87.5%) and the deceased donors were 24 (12.5%). When the relationship between living donors of the recipients was evaluated, 35 (87.5%) donors were first-degree family members of the recipients (mother, father, sibling), 3 (7.5%) donors were second-degree family members of the recipients (aunt, uncle, grandparent), 2 (5%) donors were spouse, respectively. In living donors, 16 (40%) of the donor nephrectomies performed open, 8 (20%) were laparoscopic, and 16 (40%) were robotic surgery.(Table 1)
Mean WIT for living donor nephrectomy was 2.7 ± 1.1 minutes (median 2,3 minutes, range 2-5.1 minutes). Mean CIT for living related and deceased donors were 72 ± 27 minutes (median 65 minutes, range 60-180 minutes) and 772 ± 457 minutes (median 960 minutes, range 35-1200 minutes), respectively. The mean HLA mismatch was 2.9 ± 0.93 (median 3, range 1-6). Twelve recipients were on CsA (1996-2004) and the rest of recipients were on Tacrolimus based triple immunosuppression regimen. The mean length of stay donor nephrectomy for living donors were 7.2 ± 1.3 days (median 7 days, range 3-14 days). The mean length of intensive care unit stay for deceased donors were 4.2 ± 1.2 days (median 4.1, days, range 3-15). The mean follow-up for patient and graft were 80.25 ± 54,6 months (median 73 months, range 1-171 months) and 78,63 ± 53,6 months (median 72 months, range 1-171 months), respectively. The mean serum creatinine levels of the living donors preoperative, postoperative, and at discharge were 0.93 ± 1,19, 0.96 ± 0,2 and 1,04 ± 0,15 mg/dL, respectively. In the study, the number of patients who developed surgical complications were 3 (4.6%). Subcutaneous seroma (n=1) and hematoma (n=1) occurred in Küstner incision after donor surgery. One patient required re-operation (laparoscopic appendectomy) due to appendicitis related prolonged ileus on postoperative seventh day. Twenty-one (87.5%) out of 24 deceased donors and 1 (2.5%) living related recipients presented DGF. Although DGF, graft outcome did not affect. There was no mortality in the living donors. Causes of death for and medical history of deceased donors were given in Table 2.
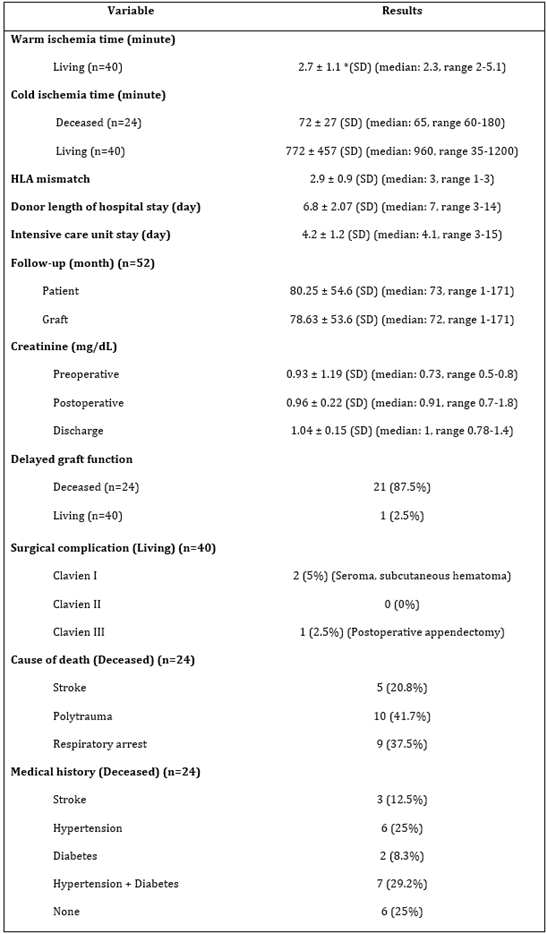
There was no follow-up data in 12 (18.8%) donors and recipients. These 12 patients’ surgeries were done between 1996-2004. Therefore, survey analysis was performed with 52 donors (and recipients) after year 2004. All survey analysis was done for Tacrolimus based triple immunosuppression regimen for the recipients. Overall, 1, 5, 10 years of recipient and graft survivals for this study were91%-88%, 81% and 84%, 82%-75%, respectively. Same rateswere observedfor living donor 96% - 96%, 96% and 90%, 88%-80%, respectively, and for deceased donorthey were81%, 74%, 70%, and 78%, 74%, 67%, respectively.
DISCUSSION
In the past, the chronological age was considered as a contraindication not only for the organ donation but also for the organ transplantation. The rapid increase in the numbers of patients with end-stage renal failure worldwide, and the limited number of donors, have become encouraging for the use of elderly donors of both living and deceased. The evolution of the donor nephrectomy to the minimally invasive surgery has contributed to the acceptability of the operation for especially living donors as well as the tendency of the living donors for the kidney donation.(9)
There are many studies showing that advanced donor age causes unfavorable outcomes for the patient and graft survival.(2-6,10) The aging process causes changes in kidneys as well as all other organs and tissues. The primary micro-anatomic structural changes consist of increasing nephrosclerosis, decreasing number of the functional glomerulus, and compensatory hypertrophy of nephrons up to some level.(11) Also, the comorbid diseases that the aging process brings such as diabetes or atherosclerosis and drug use contribute the renal damage.
The effect of donor age on graft failure shows difference for living and deceased donors. Living elderly donors have some graft outcome differences from deceased elderly donors owing to shorter ischemia time and lower HLA mismatch.(7) It was found that the risk of graft failure is almost double for deceased donors compared to the transplants from living donors. Although the elderly donor age was defined as a risk factor for the graft survival for both groups, the kidney transplantation from an elderly living donor provides a better graft survival compared to the transplantation from a deceased young donor.(10) In another study, that was determined the negative effects of the transplantations from the deceased donors of the age 50 and up, on both the graft survival and patient survival, there was no similar result for the transplantation from the living donors.(12)We may say that, using of living donors make it possible to prevent ischemic lesions. Therefore, age effect in living donors seems to be less important than in deceased donors.
Gill et al. reported in wide patient population that, the receivers of the transplantation from living donors whom aged 55 and up, have a higher rate of graft and patient survival compared to the transplantation from the deceased donors. Moreover, transplantations made from these elderly living donors were similar in 3-year graft survival with the living donors that are younger than 55 years.(13) In this study we also showed even better overall patient and graft survival results (96%, 96%, 96% and 90%, 88%, 80%). We think that the number of living donors dominating our study group is resulting in higher overall survival ratios as same as in the literature.(13-16) For living kidney donors, 60 years of age or older 1 and 5year graft and patient survival rates were reported as 98% and 95%, and 96% and 87%, respectively.(15) In our study, ratios for over the age of 55 were 96%-96%, and 90% - 88%, respectively. These are significant indicators that elderly donor isan important alternative forchronic kidney disease patients in organ transplantation waitlists.(17-18)
Kidneys from deceased donors over the age of 55 have reduced functional reserve, which has an adverse effect on long-term function. Therefore, it must be elaborated to evaluate functional reserve for the elderly deceased donors before surgery and the age must not be the only factor for the refusal of the potential donor.(2) In our study it was observed that those ratios for 5 and 10 years are 74% and 70%, respectively for the transplantation from deceased donors over 55 and up. Our findings support the deceased donors older than 55 years should be used for transplantation.
It has been widely accepted that occurrence of DGF has a long-term detrimental effect on graft function and survival. There are also some reports showing that DGF is one of the several risk factors of acute rejection and suboptimal function at one year, it is not independently associated with an increased rate of graft loss.(19) The rate of DGF varies between 29.1% and 69.3% in kidney transplants from deceased donors.(5,20) Older age is one of the most important risk factor for DGF in deceased donor transplantations.(5-6,16,20) In our series DGF incidence was 87.5%, although there were higher DGF rates among deceased donors, we did not observe worse graft or patient survival rates in the elderly donors.
Our study has some limitations. One of which, is that it is retrospective and non-comparative. We think that the prospective studies with a wider population of patients will contribute more effectively to this area. Although, it is important that our study presents that the kidney transplantation from elderly donors have no negative effects in the long term. Another limitation is that the effects of different surgical approaches cannot evaluated in elderly donors due to the number of patients. In the study, no evaluation has been made on the donor age-recipient age interaction.
In conclusion, the transplantation from the donors with age 55 and up, might be related to deceased kidney function and graft survival, compared to the transplantations from the standard donors. However, when the long term graft survival and patient survival is observed, the group of elderly donors cannot be subject to exclusion. Besides, it creates an important alternative for recipients who have a living donor candidate. The proper understanding of the results of elderly donors will allow the effective analysis of the relationship between the donor and the recipient as well as the effective choice of the patients.
Ethical approval: This study was approved by the Local Ethical Committee of Gazi University School of Medicine (reference number:13.07.2020/461).
Ethical statement of human rights: All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Data availability: The data may be made available upon reasonable request to the authors.
Conflict of interest: Authors declare no conflict of interest.

