











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Similars in
SciELO
Similars in
SciELO 
 Permalink
PermalinkINTRODUCTION
Type 2 Diabetes mellitus (DM) is a highly prevalent disease around the globe, and it has also been defined as a major cause of terminal kidney failure(1).
DNP is a common complication seen in type 2 DM patients. Alongside DNP, glomerulopathy and tubulopathy can also be observed. The early diagnosis of these pathologies has a positive effect on the patient’s prognosis. DNP leads to terminal renal failure; however, early diagnosis of the pathologies mentioned improves the chances of a cure or positive treatment response(2).
Renal biopsy is the golden standard for the diagnosis of renal pathologies. In diabetic patients, renal biopsies performed with the correct indications can detect NDNP. Several studies have detected that less diabetes duration, renal impairment, degree of proteinuria, presence of microhematuria, and the absence of DR are risk factors of NDNP(3,4). Studies have shown that diabetes patients with NDNP have better prognosis than the patients with DNP(5,6).
In this study we aimed to detect the incidences of DNP and NDNP in type 2 DM patients by analyzing their renal biopsies. The correlations between the clinical and laboratory findings were analyzed.
MATERIAL AND METHODS
We retrospectively reviewed the medical records of 495 patients that underwent renal biopsy from July 2020 to August 2022 at the nephrology clinic of Hospital Umraniye. 140 patients who had type 2 DM diagnosis were enrolled into our study. Cases with inadequate renal biopsy, history of renal transplant or second/follow up biopsies were excluded.
DM was defined by the American Diabetes Association criteria(7). (People with fasting plasma glucose values of ≥ 7.0 mmol/L (126 mg/dl), 2-h post-load plasma glucose ≥ 11.1 mmol/L (200 mg/dl), glycated hemoglobin (HbA1c) ≥ 6.5% (48 mmol/mol); or a random blood glucose ≥ 11.1 mmol/L (200 mg/ dl) in the presence of signs and symptoms are considered to have diabetes)
The indications of renal biopsy in diabetic patients included the following.
1. Nephrotic range proteinuria (>3500mg /24 hours urine)
2. Non nephrotic range proteinuria (>300-3500mg/24 hours urine)
3. Proteinuria (>300mg/24 hours) and unexplained microscopic hematuria (more than 5 red blood cells per high power field in a centrifuged urine sample)
4. Proteinuria and reduction in kidney function (increase in the serum creatinine value)
5. Proteinuria, microscopic hematuria, and reduction in kidney function
6. Reduction in kidney function
7. Unexplained microscopic hematuria
Renal biopsy was guided by an ultrasound device and performed using an automatic biopsy instrument with a hollow probe guide, needle 16G. Two kidney biopsy specimens were obtained; one sample for light microscopy, and the other was taken for immunofluorescence microscopy.
The biopsy samples were processed for light microscopy and immunofluorescence. DNP was diagnosed and classified by the presence of mesangial expansion and diffuse inter-capillary glomerulosclerosis, with or without the nodular Kimmelstiel-Wilson formation, basement membrane thickening, fibrin caps or capsular drops(8). Electron microscopy examination was not possible due to the accessibility of the equipment.
DNP was histopathologically classified according to Renal Pathology Society(9).
Class I - Isolated glomerular basement membrane thickening. There is no evidence of mesangial expansion, increased mesangial matrix, or global glomerulosclerosis involving >50 percent of glomeruli.
Class II - Mild (Class IIa) or severe (Class IIb) mesangial expansion. A lesion is considered severe if areas of expansion larger than the mean area of a capillary lumen are present in >25 percent of the total mesangium.
Class III - At least one Kimmelstiel-Wilson lesion (nodular intercapillary glomerulosclerosis) is observed on biopsy, and there is <50 percent global glomerulosclerosis.
Class IV - Advanced diabetic glomerulosclerosis. There is >50 percent global glomerulosclerosis.
Patients were grouped as:
1.DNP
2. NDNP
The patients with NDNP were also divided into 2 subgroups according to the presence of diabetic nephropathic lesions in their biopsies.
Clinical details including age, gender, duration of diabetes (cut off 5 years), presence of hypertension, presence of DR, indications of renal biopsy were obtained from the records. The laboratory profile included blood urea nitrogen, serum creatinine, albumin, HbA1c, urinalysis, proteinuria by 24 -hours urine collection, rheumatological tests (Antinuclear antibody (ANA), complement C3 and C4 levels, anti-double stranded DNA (anti dsDNA), and anti-neutrophil cytoplasmic antibodies (ANCA), viral serology (HBV, HCV, HIV).
The duration of disease was defined as the period between age of onset and age at performing renal biopsy. Hypertension was defined as systolic blood pressure more than 140 mmHg, and diastolic blood pressure more than 90 mmHg(10). DR was diagnosed on a fundoscopy by an ophthalmologist.
Our study was carried out in accordance with the Helsinki Declaration.
Statistical Analysis
Statistical Package for Social Science (IBM SPSS Statistics New York, USA) version 20.0 was used to perform statistical analyses. Descriptive statistics are reported as means ± SDs for continuous variables and as number and frequencies for binary and categorical variables. The comparison of these variables was conducted with Mann-Whitney U test for continuous variables, as the data distribution was non-parametric. Chi-square test was used for categorical variables. Variables were entered into a univariate (UV) logistic regression model. In addition, parameters that we thought would be significant such as age, gender, disease duration, retinopathy, hbA1c, proteinuria and hematuria were included in the model. A multivariate (MV) logistic regression model was then constructed using an enter procedure among those candidate variables with the significance level p. p<0,05 was set as statistical significance.
RESULTS
Over all 140 patients (mean age 55,10±11,10 years, 49 % female) were included in the study. 55,7 % had DNP. The most common pathological diagnosis in patients with NDNP (44,3%) was tubulointerstitial nephritis (20%), followed by focal segmental glomerulosclerosis (FSGS) and nonspecific results (18,3%, 13,3%). 42,1% of the patients exhibited DR. According to the pathological classification of DNP, 3 patients were identified as class 1, 8 patients as class 2a, 4 patients as class 2b, 32 patients as class 3 and 19 patients as class 4.
The incidence of DR was higher in the DNP group than the NDNP group. (60%, 11%, p<0,001). Nevertheless, there was not any significant difference between classes of DN in terms of DR (p:0,180). There was a statistically significant difference between the DNP and NDNP groups in terms of the duration of diabetes (11,23 ± 5,74 years, p:0,002). There was no statistically significant difference between the two groups in terms of hypertension incidence (p:0,907).
There was a statistically significant difference between two groups’ renal biopsy indications (p<0,001). DNP group patients underwent renal biopsy mostly due to nephrotic proteinuria (40%), meanwhile NDNP patients’ renal biopsy indication was mostly renal dysfunction (40%). Acute kidney injury (ACI) frequency was increased in patients diagnosed NDNP compared to patients with DNP (p:0,027).
The degree of proteinuria in the 24-hour urine and frequency of proteinuria of the patients in the DNP group were significantly higher than those in the NDNP group (p:<0,001, p:0,009). Lower degree of proteinuria was detected in class 1 and 2 of DNP than class 3and 4. There was significant difference between histopathological classes of DNP in terms of 24 hours urine proteinuria levels (p:<0,001). In addition, there was significantly statistically difference in favor of NDNP in terms of hematuria, HbA1c and serum albumin levels (p:0,043, p:<0,001, p:0,002). Statistically, more hematuria, lower HbA1c and higher albumin levels were detected in NDPN. Although the frequency of microhematuria is increased in classes 3 and 4 of DN more than classes 1 and 2, there wasn’t any statistically significant difference between classes of DNP in terms of hematuria. (p:0,701)
Biopsies diagnosed NDNP but also include lesions similar DN accounted 34,2% of biopsies accepted as NDNP. 32% of these mixed biopsies were diagnosed as TIN and ATN (acute tubular necrosis), 20% as nonspecific glomerular pathology and 28% as other primary glomerulonephritis. Patients diagnosed NDNP but also have diabetic lesions in their biopsies had increased level of proteinuria than patients with pure NDNP. However, we did not find any statistically significant difference in terms of degree of proteinuria between these patients (p:0,137).
Table1and2are showcasing the demographic, clinical and laboratory data of patients with DNP and NDNP.
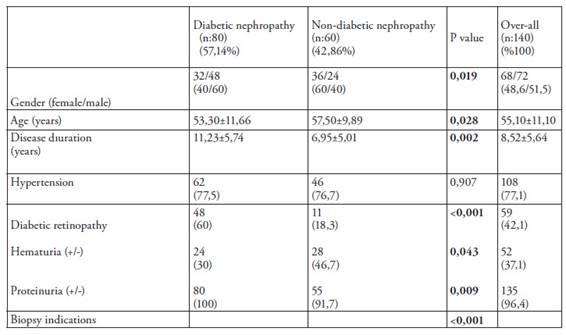
Table 1: Demographic and clinical features
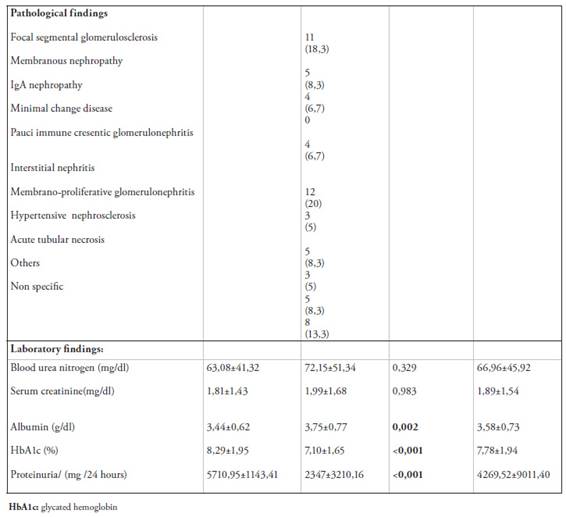
Table 2: Pathological findings and laboratory data
Table 3is showcasing the logistic regression analysis made to predict DNP in diabetic patients. The results show that DR and HbA1c value more than 7% have increased the risk of DNP incidence 4, 482 and 4,591-fold (p:0,021, p:0,024).
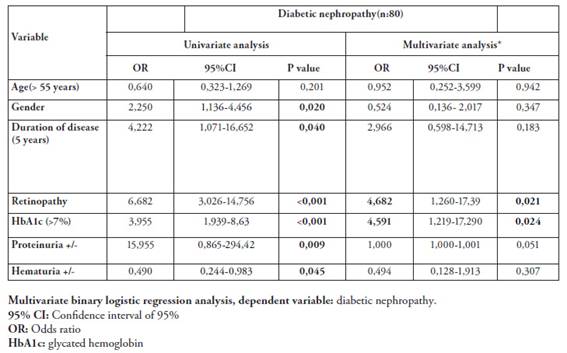
Table 3: Prediction of DNP in diabetic patients
DISCUSSION
In this study 140 diabetic patients’ kidney biopsy results were examined retrospectively. 57,14 % of biopsies were reported as DNP. TIN was the most common pathological diagnosis in the group of NDNP. DR was significantly increased in patients with DNP. There was not any significant difference between classes of DN in terms of DR. Also, duration of disease was significantly longer in the group of DNP. The degree of proteinuria in the 24-hour urine and frequency of proteinuria of the patients in the DNP group were significantly higher than those in the NDNP group. Also, there was significant difference between histopathological classes of DNP according to proteinuria levels. Most detected biopsy indication of the patients in group DNP was nephrotic range proteinuria, while reduction of kidney function was the most common kidney biopsy indication in the group NDNP. The results of our study showed that HbA1c >7 % and having DR increased the risk of DNP.
Diabetic patients may also have different renal pathologies other than DNP. These glomerular or tubular pathologies can be treated, and as a result, progression to end-stage kidney disease can be prevented. Several studies showed different proportion of NDNP pathologies(11,12). According to Artan et al FSGS was the most common diagnosis (29,5%), like the study of Heybeli et al(13,14). In our study TIN was found to be the most common NDNP in diabetic patients. The most common biopsy indication in patients with NDNP was deterioration of renal functions, which may explain TIN as the most common pathology in these group. Nevertheless, these patients still had different levels of proteinuria so we couldn’t detect nonproteinuric diabetic kidney disease in our study. These differences in the results of studies can be explained by the fact that the population and number of patients participating were different in each study.
Renal biopsy in diabetic patients is performed in the presence of progressive increases in the amount of proteinuria, deterioration in renal functions, presence of hematuria, and additional systemic findings suggesting NDNP. In the studies, nephrotic range proteinuria, presence of microhematuria, impaired renal function, raised proteinuria without DR were frequently detected indications for renal biopsy(15,16). Similarly, in our study, the most common renal biopsy indication was nephrotic range proteinuria, followed by non-nephrotic range proteinuria and deterioration in renal functions.
The correlation of DR with the development of DNP in diabetic patients has been demonstrated in various studies(12,17). Zhang et al showed in a study of 250 patients with type 2 DM that DR was an independent risk factor for renal outcomes in patients with DNP(18). According to Garcia martin et al the absence of retinopathy and the presence of microhematuria are highly suggestive of NDRD(19). However, Prakash et al claimed that there was no significant correlation between DR and histopathological findings of DNP(20). In our study we found significant correlation between DNP and DR like most of the studies. We also found that DR was an indicator that raised DNP frequency in diabetic patients. The frequency of DR in patients with severe diabetic histopathological lesions was increased although not statistically significant.
Duration of diabetes is associated with occurrence of DNP. Several studies confirmed that shorter duration of diabetes is a risk factor of NDNP in diabetic patients(15,21,22). Bermejo et reported a study in110 patients with DM and found significant relation between less duration of diabetes with incidence of NDNP(23). They also found presence of DR and low degree of proteinuria over 24 hours as protective factors against development of NDNP. In our study similarly we found longer duration of diabetes in patients with DNP. However, in our regression analysis we didn’t detect duration of diabetes as an indicator of DNP. Therefore, DNP should not be overlooked in patients with short-term DM.
Bad glycemic control is an important risk factor for progression of renal pathologies. It also related with development of DNP in diabetic patients. Liang et al reported a meta-analysis including 63 studies with 2322 patients and they found low level of HbA1c was a predictor of NDNP(24). We also found that HbA1c more than 7 % was a risk factor for development of DNP. According to this result, we can conclude that we should carefully consider our biopsy indications by predicting that the result of renal biopsy in patients with poor glycemic control is more likely to result in DNP.
The presence of microscopic hematuria has been suggested an indicator of NDNP. Several studies have found a significant correlation between microscopic hematuria and NDNP(25,26). Nevertheless, Serra at al claimed that microscopic hematuria was detected more commonly in DNP patients than NDNP(27). Also, according to Tone et al microscopic hematuria wasn’t a good predictor of NDNP comparing other other parameters(28). We found statistically significant difference between DNP and NDNP group according to presence of microscopic hematuria ın our study. Hematuria detected more in patients with NDNP. However, inspite of this difference hematuria wasn’t detected as an indicator for patients diagnosed DM in our regression analysis.
Reduction in kidney function is an important indication for renal biopsy in diabetic patients. It also may predict NDNP in these patients(23). According to Bermejo et al creatinine was a predictor factor for NDNP(24). In our study serum creatinine levels higher in patients with NDNP but it didn’t show any statistical significance. Therefore, although renal function deterioration is the most common biopsy indication in patients with NDNP, increased serum creatinine should not predict the diagnosis of NDNP.
According to studies, we see that the amount of proteinuria is higher in patients with DNP(25). Also, we know that for progressive increases in proteinuria and proteinuria of nephrotic level, renal biopsy is frequently performed to avoid overlooking NDNP. Detection and prevention of proteinuria is important in these patients since presence of proteinuria and its high degrees have negative effect on patients ‘renal prognosis. According to Artan et al proteinuria was significantly higher in DNP group, but it didn’t increase the risk of DNP(13). Yang et al analyzed 232 patients and showed that non nephrotic range proteinuria indicated NDNP(16). Lin et al reported lower degree of proteinuria in patients with NDNP and they suggested this was a significant factor for indication of renal biopsy(29). On the other hand, Yaqup et al reported patients with DNP had higher level of proteinuria but it didn’t show a statistical significance30. According to our study the degree and incidence of proteinuria were significantly higher in group of DNP. In addition, we found that patients with NDNP but also had diabetic lesions in biopsy had increased level of proteinuria than pure NDNP. Nevertheless, we did not detect proteinuria as a predictive factor for developing DNP. Result of these findings we think that we cannot accept the presence of proteinuria alone as a predictor of DNP, regardless of the level of proteinuria, since the frequency of proteinuria is high in both patient groups.
One limitation of this study is that it was not multi-centered. Though a multi-centered study would be more ideal, our sample size of 140 patients led us to statistically significant findings. Unavailability of certain equipment such as an electron microscope was another limitation that needs to be considered. The absence of EM could’ve led us to miss certain pathological findings. A third limitation is the fact that this study was retrospective, which left us unable to comment on the renal outcomes of the patients. Unlike other studies, we detected high HbAc1 levels as a predictor for DNP. Apart from this, the results of our study were consistent with the previous literature.
CONCLUSION
NDNP was detected in 42.86% of the patients participating in our study. While we found a significant difference between our patient groups in terms of age, gender, proteinuria, hematuria, duration of disease, DR and HbA1c levels, we determined in our analysis that only the presence of DR and a HbA1c level more than 7% are factors in predicting DNP. Overlooking the NDNP, which are frequently seen in diabetic patients, may lead to the inability to treat patients and lead to end-stage renal failure. Renal biopsy in diabetic patients with the right indication without delay is very valuable in terms of the patient's renal prognosis.

