











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Similars in
SciELO
Similars in
SciELO 
 Permalink
PermalinkA 50-year-old man with pain in his left ankle and dif ficulty placing his foot on the ground for two days. He denied diabetes mellitus. He had a left foot painful crisis with 18-year-old without limitation in the mobility, but with pain in other joints. He was treated symptomatical ly until the rheumatoid arthritis diagnosis with 30-year-old, treating with prednisone (one year). For the next ten years, he was treated with painkillers until a new left foot pain crisis, being treated with adalimumab (six months) followed by etanercept (one injection/week) and methotrexate (twelve years), showing improvement since then. Physical examination shows foot deformity, with difficult in walking and pain on palpation - Foot and Ankle Out come Score: 32%. MRI (Fig. 1) showed pantarsal coalition, affecting the joints: talocalcaneal; second metatarsal and intermediate cuneiform; third metatarsal and lateral cuneiform; fourth metatarsal and cuboid; medial, inter mediate, lateral cuneiforms and navicular; talonavicular; calcaneocuboid. He was treated with betamethasone and tramadol, with pain resolution, and follow-up with imag ing tests each four months.
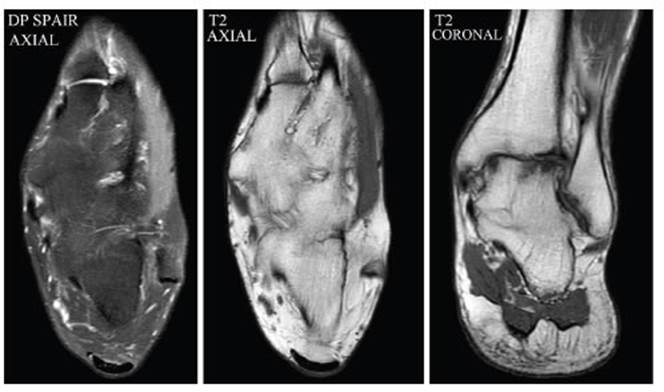
Tarsal coalition has a variable clinical presentation and should be considered in the differential diagnosis of painful foot. Its diagnosis is made by radiographs, but CT scan and MRI are considered the gold-standard for diag nosis.

