











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Similars in
SciELO
Similars in
SciELO 
 Permalink
PermalinkINTRODUCTION
The disease caused by SARS-CoV-2 (COVID-19) spread rapidly worldwide and has become a sig nificant public health issue. The first case was reported in 2019. This led to an unprecedented increase in the number of patients requiring pro longed stays in the Intensive Care Unit (ICU) due to respiratory complications caused by COVID-19. 5 % of these patients required endotracheal in tubation and mechanical ventilation for acute hypoxemic respiratory failure.1,2
While orotracheal intubation (OTI) is an es sential tool for the management of patients in the intensive care unit, one of the complications it can generate is tracheal stenosis. Although the incidence is low at present, thanks to applied new technologies, it still exists. These advances began to be used after research conducted by Grillo and Cooper in 1966,3 where they determined the physiopathology of tracheal stenosis. The rate of laryngotracheal stenosis postintubation (LSPI) in non-COVID-19 patients is between 10 and 22 %.4,5 Although the rate of LSPI related to COVID-19 is still unknown, it is believed that this complica tion is even more common.6 This could possibly be due to the debate regarding the timing of the tracheostomy that took place at the beginning of the pandemic (due to the risk of virus aerosoliza tion), leading to many cases being performed late.7
We present the experience in managing a series of consecutive patients who underwent surgical treatment.
MATERIALS AND METHODS
An analytical, prospective, observational study was con ducted. A database was created, including the patients who underwent tracheal resection with primary anastomosis at the Sanatorio Allende, New Córdoba and Cerro branches (Córdoba city, capital of the Province of Córdoba, Argentina) between August 2021 and September 2022.
All patients signed an informed consent prior to surgery.
The study was reviewed and approved by the Ethics Committee of the Sanatorio Allende.
Inclusion criteria
• Patients of both sexes, aged 16 and older, diagnosed with complex central airway stenosis following prolonged intubation with mechanical respiratory support as a treatment for COVID-19.
Exclusion criteria
• Patients with tracheal stenosis greater than 5 centime ters and/or with general contraindications for surgical treatment.
All the patients had a standard evaluation. They un derwent axial, coronal and sagittal computed tomography scans (CT) and flexible fiberoptic bronchoscopy (FFB). With the CT and FFB results, both the length and location of the stenosis were determined.
A complex tracheal stenosis is considered to be one exce eding 1 cm in length and with involvement of the tracheal wall. Cases were classified according to the Myer-Cotton classification.8
In patients where the stenosis affected the cricoid carti lage, laryngotracheal resection was considered.
The surgical technique is similar to that described by Mathisen9 with a few modifications.
To the patient with tracheoesophageal fistula, closure of the opening on the anterior face of the esophagus was per formed using 3.0 silk sutures on the mucosa and muscular layers separately. Regarding anesthesia, all patients recei ved either inhalation gas or total intravenous anesthesia. In patients with severe tracheal stenosis, tracheal dilation was performed prior to the placement of the orotracheal tube. At the end of the surgery, the patients were extubated.
To assess ventilation and phonation, patients were eva luated at 7 days, 15 days, and 30 days post-surgery.
Ventilation was assessed basing on the presence or ab sence of stridor in the postoperative period.
Phonation was assessed basing on the presence or abs ence of dysphonia in the postoperative period.
The Clavien and Dindo classification was used to grade postoperative complications, with follow-up extended up to 60 days.
A new FFB was conducted on all patients after 30 days to evaluate the status of the anastomosis.
Statistical analysis
All the variables in research were expressed in percentages, maximum, minimum, and median.
The Wilcoxon test was used to compare the presence or absence of stridor on days 7, 14, and 30 after surgery in patients who presented stridor as initial symptom, consi dering a p-value < 0.05 as statistically significant.
The Wilcoxon test was also applied to compare preopera tive and postoperative fiberoptic bronchoscopy, taking into account whether the postoperative fiberoptic bronchoscopy showed a preserved tracheal lumen diameter or not; the statistically significant value was p < 0.05.
RESULTS
Out of the 19 initially evaluated patients, 8 were excluded, resulting in a final sample size of 11 participants. (Figure 1)

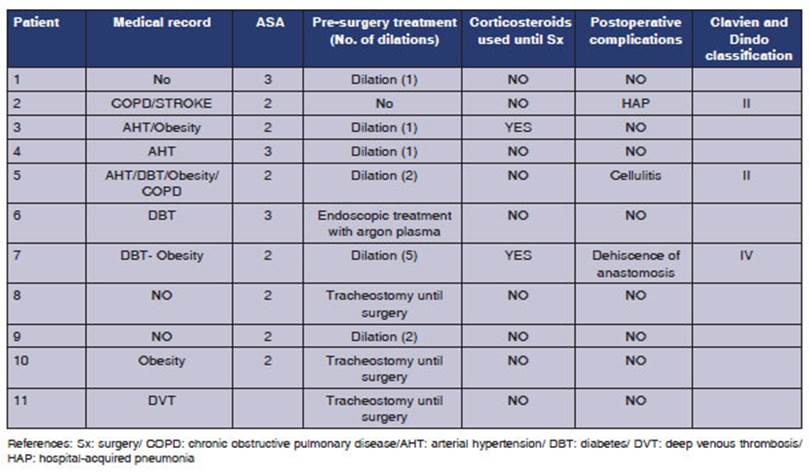
Of the included patients, 9 (81.8 %) were male, with a mean age of 52 years (MAX: 72 MIN: 32 MEDIAN: 47). Table 2 shows the medical record, surgical risk (ASA score), pre-surgery treatment, history of corticosteroid use, and postoperative complications (Clavien Dindo classification). 27.2 % of the patients had postoperative complications.

Only one patient was diagnosed with COVID-19 in the year 2020; the rest were diagnosed in 2021.
All the patients had OTI, with an average of 13 days (MAX: 21 MIN: 8 MEDIAN: 12). 5 patients (45.4 %) underwent a tracheostomy. The average of days between the OTI and the tracheostomy was 13 (MAX: 20 MIN: 9); and 3 patients (27.2 %) remained with the tracheostomy until surgery; 2 of them due to total laryngotracheal occlusion and the rest due to tracheoesophageal fistula.
The presenting symptoms and reasons for consultation were as follows: stridor and dyspnea (36.3 %), stridor only (27.2 %), aphasia (18.1 %), stridor, dyspnea, and dysphonia (9 %), and bron choaspiration (9 %). The results observed in the neck CT and FFB are detailed in Table 3.
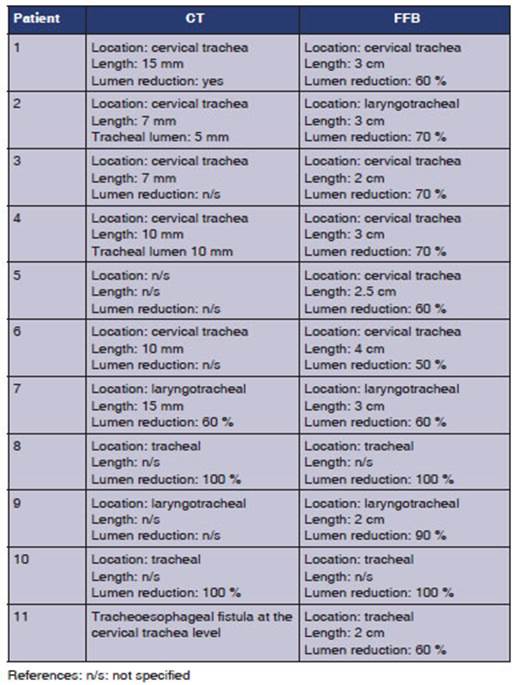
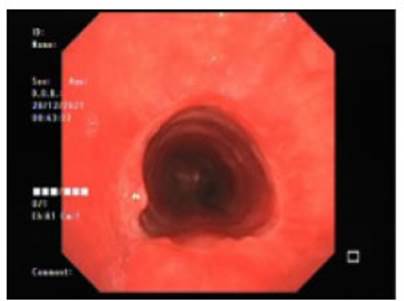
Figure 3 FFB 30 days after surgery. Description: The diameter of the tracheal lumen is observed to be preserved

Figure 4 FFB of tracheoesophageal fistula. Description: Com munication between the airway (above) and the esophagus (below) is observed
References: n/s: not specified
According to the Myer-Cotton classification, 8 patients were grade 2; 2 patients were grade 4, and 1 patient was grade 3.
The average number of months between the diagnosis of COVID-19 and tracheal resection surgery was 7 (MAX: 25 MIN: 2).
54.4 % of the patients required at least one tracheal dilation prior to surgery. One of the patients underwent endoscopic treatment using argon plasma without the expected results before surgery.
Laryngotracheal resection was performed on 36.3 % of the patients, and tracheal resection on 63.6 %.
The average duration of surgery, measured in minutes, was 191 (MAX: 240 MIN: 120). The aver age hospital stay was 6 days (MAX: 7 MIN: 5). Only one patient required surgical reintervention due to dehiscence of the anastomotic suture 47 days after surgery.
The average resection length (measured in cm) was 2.9 (MIN: 1.5 MAX: 5).
There was no mortality at 60 days.
In the assessments at 7 and 14 days post-sur gery, 5 patients showed dysphonia.
At the 30-day assessment, 4 patients experi enced dysphonia.
In the postoperative period, endoscopic treat ment with argon plasma was performed in only 1 patient for granulomas at the anastomotic level.
Statistical analysis
Regarding the assessment of preoperative stridor compared to the control at 7 days, no patients showed stridor; and the same was observed at 14 days. Only one patient exhibited stridor at 30 days. In this comparison, 8 patients were included, as 3 patients maintained the trache ostomy until surgery, making the symptom unassessable.
The result of the comparison between preopera tive stridor and the assessment of the presence of this symptom at 7, 14, and 30 days was statistically significant in all cases (p < 0.05) (Table 4).

In the comparison between the initial FFB and that of 30 days post-surgery, only one patient ex hibited a decrease in the diameter of the tracheal lumen. The result was statistically significant (p > 0.05) (Table 5).

DISCUSSION
The approach to treat benign tracheal stenosis is very complex, so it should be carried out in highly experienced centers. It requires a trained team to do a proper evaluation and determine the best treatment option, with tracheal resection and pri mary anastomosis being one of the choices.
There are very few studies in the literature that show the results of tracheal surgery for benign stenosis, and if we specifically focus on tracheal or laryngotracheal resection for stenosis secondary to intubation from COVID-19, we find only two studies, with the rest being case reports.
Regarding our results, the most prevalent symp tom in the postoperative period was dysphonia, but it was mild in all the cases, and it didn’t prevent the patients from carrying out their daily activities normally. Only one patient required endoscopic treatment related to dysphonia, specifically due to granulomas on the vocal cords.
27.7 % of the patients showed postoperative complications, with two being classified as mild (Clavien Dindo II) and one more severe: dehiscence of the anastomotic suture (Clavien Dindo IV), which required emergency tracheostomy and was a late complication, occurring 47 days post-surgery. This case was the patient whose FFB showed a de crease in the tracheal lumen 30 days post-surgery. Upon analyzing the complications, it is observed that all three patients were classified as ASA 3, and the patient with the most severe complication continued using corticosteroids until the surgery and had undergone 5 previous dilations. These are known risk factors for tracheal resection surgery.10
The most common presenting symptom was stridor, which was taken into account when assess ing ventilation in the postoperative period. When comparing the preoperative period with control at days 7, 14, and 30 after surgery, the difference in the absence of stridor was always statistically significant (p < 0.05), indicating the positive out comes of the surgery. The same trend was observed when comparing the preoperative FFB with the one performed 30 days after surgery. The result was also statistically significant (p < 0.05) for the preserved tracheal lumen diameter in the postoperative period, which correlates with the absence of stridor and underscores the success of the surgical treatment.
Piazza’s work11 is the only one in the literature showing the results of a case series involving tracheal or laryngotracheal resection secondary to tracheal stenosis caused by COVID-19. The number of patients treated in that study is 14, very similar to our experience. The mean age of the patients and the male-to-female ratio are also similar. In their study, the mean duration of the OTI was 15.2 days, and a tracheostomy was performed on 10 patients. In our work, the mean duration of the OTI was 13 days, and a tracheos tomy was performed on 5 patients. Just like in our work, 3 patients arrived to the surgery with a tracheostomy.
With regard to the location, in both studies, the most frequent location was the cervical trachea. The most commonly performed procedure on patients before surgery was tracheal dilation. In Piazza’s work,11 the mean time of hospitalization was 12.1 days, compared to 6 days in our study. They documented a case of restenosis, whereas we had none in our study.
Another study that shows results of tracheal surgery in patients with stenosis secondary to prolonged intubation is the one from Palacios12. However, it includes various tracheal procedures (tracheal resection, Montgomery T-tube place ment, endoscopic treatment), and in the descrip tion of the results, it does not specify the technique that was used. The most frequently affected site was the cervical trachea. According to the Myer- Cotton grading system, the majority of the cases were grade III; in our work, the majority were grade II.
The remaining articles are related to tracheal surgery for tracheal stenosis but not specifically associated with COVID-19.
Wright’s work,10 evaluates the results of 392 patients operated on at the Massachusetts General Hospital from 1993 to 2017. The mean number of tracheal resections performed per year is 16.3; this figure aligns with the significant number of patients included in our study. The study states that the most common presenting symptoms are stridor, dyspnea, cough, and dysphonia, very simi lar to those observed in our patients. In Wright’s study, 92 % of patients received some form of treatment before surgery, compared to 63.6 % in our patient series. The mean length of tracheal resection was very similar, with 3 cm in Wright’s work and 2.9 cm in ours. The best outcomes were obtained in patients without prior treatment for tracheal stenosis and without prior use of cortico steroids. That is why it is very important not to delay the diagnosis.13
The overall morbidity rate was 33 % in Wright’s study versus 27.7 % in our work. There was dehis cence of anastomosis in 4 % of Wright’s patients compared to 9 % (1 patient) in our series. Similar to our findings, in Wright’s study there were no significant differences between pure tracheal re section and laryngotracheal resection.
The study by Natuta14 reveals the results of 43 patients who underwent tracheal resection between 2007 and 2018, with a mean follow-up of 58 months. Similar to our findings, the study did not report any deaths within the first 30 days. Dyspnea was measured using the visual analogue scale for dyspnea, showing a noticeable improve ment in the postoperative period with statistically significant results. Regarding voice assessment, it was determined that 30 patients experienced mild deterioration.
The results presented in the series of patients who underwent tracheal or laryngotracheal resec tion for benign stenosis unrelated to COVID are similar to those obtained in our study. This sug gests that this condition should not significantly alter the treatment approach.
As for the limitations of the study, it should be noted that the number of cases does not allow for statistical analysis to relate variables studied in our work and compare them with the results of non-COVID-19 patients.
CONCLUSION
The COVID-19 pandemic posed a significant chal lenge for healthcare professionals worldwide. There was a substantial increase in patient admissions to critical care units with the need for OTI. Initially, due to concerns about virus aerosolization, changes in guidelines were implemented, leading to delays in performing tracheostomies. These factors con tributed to an increased rate of tracheal stenosis.
For complex tracheal stenosis, it is crucial to have a team with experience in tracheal surgery. With appropriate indications, tracheal resection with primary anastomosis should be considered the first option. In the hands of experienced surgeons, it is a safe and effective procedure.
The postoperative results in this series of pa tients are similar to those with benign tracheal stenosis unrelated to COVID-19.
A multicenter study should be conducted to increase the number of cases and obtain more significant results.

