











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Similars in
SciELO
Similars in
SciELO 
 Permalink
PermalinkINTRODUCTION
The SARS-CoV 2 pandemic challenged the major ity of the healthcare systems worldwide, with a high utilization rate of critical care and not enough qualified human resources. This situation gener ated the need to meet the demand by employing personnel without the necessary expertise or by increasing the workload of the staff in those areas. In this context, new publications emerge daily on the stress experienced by the healthcare system and personnel.1
Patients who suffered from severe COVID-19 experienced prolonged stays in the ICU, prolonged use of analgosedative and neuromuscular blocking agents, the need for mechanical ventilatory assis tance (MVA), and extended prone positioning cycles. The simultaneous large number of critical patients exceeded the capacity of the personnel to provide adequate care, and this caused potential complica tions related to the stress of healthcare workers.1,2
Heterotopic ossification (HO) consists in the formation of bone tissue in areas of extraskeletal soft tissue where there is usually no bone.3
There are two typical presentations of HO: he reditary and acquired. The latter is more prevalent and is primarily observed in patients with pro longed immobilization following musculoskeletal traumatic injuries, neurological injuries, major burns, ARDS, or major surgeries.4
Prolonged immobilization is a common factor among patients with traumatic brain injury, spinal cord injury, ARDS from other causes, and severe COVID-19.5
Tissue injury results in the invasion of inflam matory cells, causing an alteration in cells with mesenchymal origin. This impairment can lead to an osteogenic or osteochondrogenic program as mesenchymal cells differentiate into osteoblasts.6 The systemic inflammation, altered calcium me tabolism, and local myositis seen in patients with COVID-19 could potentially trigger this effect.7
Recently, HO has been reported as a complica tion associated with severe COVID-19 patients who underwent extended periods of MVA and prolonged hospital stay.7 In the vast majority of cases, heterotopic ossification was identified after hospital discharge, with pain, limited range of motion, and joint stiffness as the symptoms that triggered suspicion. Subsequently, the diagnosis was confirmed through imaging studies.5,8,9
CASE REPORT 1
A 43-year-old male patient was admitted to the ICU for severe COVID-19 pneumonia, after two days of hospitalization in a general ward, where hypoxemia persisted despite receiving high concen trations of oxygen. The only comorbidity presented by the patient was Class I obesity. Upon admission to the ICU, the patient required MVA and met the criteria for severe ARDS.
During the initial 10 days in the ICU, the patient underwent four alternating prolonged prone po sitioning cycles, totaling 192 hours in that period and in that position. Until day 23 in the ICU, the patient received deep sedation and neuromuscular blocking agents. Complications included infectious events, a sacral pressure ulcer, and intensive care unit-acquired weakness (ICUAW). After discon tinuing neuromuscular blockade and maintaining a superficial level of sedation, the patient’s muscle strength, assessed using the MRC scale, scored 38/60. This score fell below the cutoff point of 48/60. [10]. The patient was weaned from MVA on day 31 of ICU stay, and was discharged from the hospital on day 52 since admission, without requir ing supplementary oxygen and with a MRC score of 50/60. Throughout the hospital stay, the individual had an average daily intake of 1044 mg of calcium, 728.6 mg of phosphorus, and 737.6 IU of vitamin D. The average daily intake of corticosteroids was 9.29 mg (0.093 mg/kg/day) of dexamethasone.
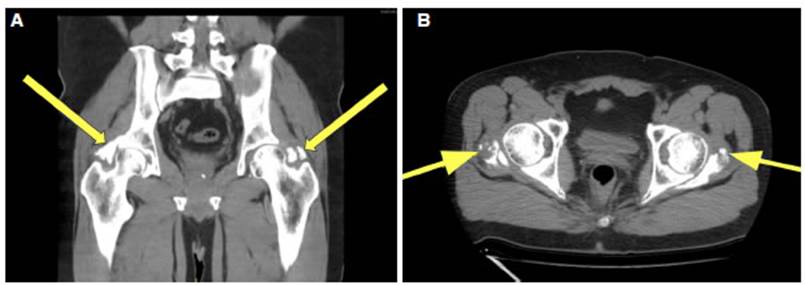
Six months after discharge, the patient pre sented with pain and limited external rotation movement, and inability to abduct both hips. A pelvic and hip CT scan was requested, revealing bilateral HO of the hip (Fig. 1A and 1B).
CASE REPORT 2
A 58-year-old patient, hypertensive and with Class 1 obesity, hospitalized in a general ward and diag nosed with severe COVID-19 pneumonia suffered an ischemic stroke and was transferred to the ICU. The patient’s respiratory condition deteriorated, requiring MVA. The patient received two prone positioning cycles, totaling 60 hours within the first 10 days of ICU stay. He/she experienced infectious complications and a sacral pressure ulcer. Weaning from MVA was achieved after 39 days. The patient remained in the ICU for a total of 45 days and was discharged from the hospital 111 days since initial admission. Throughout the hospital stay, he/she had an average daily intake of 2,359.34 mg of calcium, 1,538.6 mg of phosphorus, and 1,190.8 IU of vitamin D. The average daily intake of corticosteroids was 7.75 mg (0.072 mg/ kg/day) of dexamethasone. Upon discharge, the pa tient did not require oxygen therapy but presented with a moderate right brachio-crural motor deficit, ataxia, visual field impairment, and gastrostomy tube feeding due to swallowing disorder. One year post-discharge, there was functional improve ment, but with evident limitations in movement unrelated to the motor deficit. A pelvic CT scan was performed, revealing heterotopic ossification in both hips. (Fig 2A and 2B).
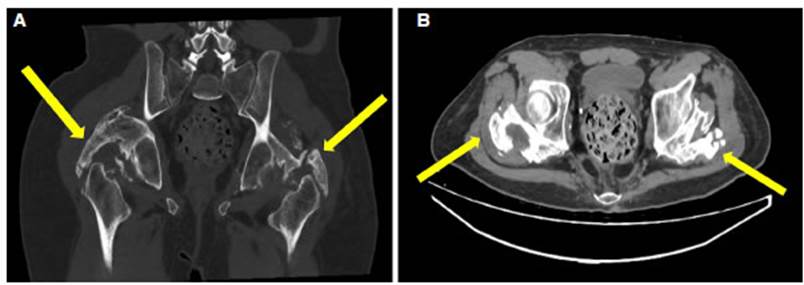
Figure 2 Pelvic and hip CT scan. 2A Coronal plane and 2B Axial plane. In both images, the arrows indicate the presence of het erotopic ossification.
As of the current date, there has been no surgi cal opportunity.
DISCUSSION
The published cases of HO in patients with COV ID-19 occurred in the context of severe forms of the disease, involving prolonged hospitalizations and invasive ventilatory support due to ARDS5-9,11-13. As with any cause of severe ARDS, paralysis and deep sedation were part of the therapeutic approach.14,15
During the stay of the two described patients, the occupancy rate of the ICU exceeded between 66 % and 100% its maximum capacity. That is to say, the occupational rate was 16 6% and 200 %, and the workload of the nursing staff, measured by TISS-28, was 72 points, nearly double the workload manageable by a nurse [own data]. Infectious complications such as mechanical ventilation-associated pneumonia, catheter-asso ciated infections, and pressure ulcers caused by the decubitus position tripled the average value of the service. In this context, motor kinesiotherapy was postponed due to the need to address urgent circumstances, contributing to prolonged periods of immobilization. The reduced bedside times interfered with the proper implementation of ventilatory weaning protocols, resulting in longer periods of MVA and ICU stay. Consequently, there was greater use of neuromuscular blocking agents and sedatives, generating prolonged patient im mobilization.
Some publications addressing the pathogenesis of HO consider immobilization as an associated factor, without specifying the differences between active and passive motion. The work of Stoira et al, shows a four times higher prevalence in COVID-19 distressed patients compared to those with other causes of ARDS.
We do not know the dose values of parathyroid hormone, phosphorus, or vitamin D. However, the intake of calcium, vitamin D, and phosphorus were adequate for baseline needs. Regarding the use of corticosteroids, the doses were very high, and were consistent with what was reported by Stoira et al. While some characteristics specific to SARS-CoV-2 infection are suggested, such as humoral alterations, disturbances in calcium metabolism, inflammatory response, and direct muscle injury, the conclusion is that prolonged immobilization is the only relevant factor in the multivariate analy sis. The recommendation is early passive motion as a preventive method for the development of HO.7
CONCLUSION
Our case report identifies factors that have been mentioned in the literature as possible causes of HO in COVID-19 patients. This includes the prolonged use of sedatives and neuromuscular blockers in patients experiencing intense inflammation. The critical condition and therapeutic strategy result in long periods of immobilization during the ICU stay.
However, the above description does not fully explain the higher prevalence of HO in patients who experienced ARDS due to COVID-19 when compared to patients who suffered ARDS from other causes. Thus, there are no differences regarding the inflam matory processes or the recommendation to use deep analgosedation and neuromuscular blockade.
We interpret that the workload generated by patient care during the pandemic peaks had a sig nificant influence and caused unusual situations in daily practice. This included prioritizing respi ratory kinesiotherapy over motor intervention, difficulty in implementing MVA weaning protocols, and less time spent at the patient’s bedside due to isolation conditions.
As a result, this could have led to more days of sedatives and neuromuscular blocking agents, prolonged mechanical ventilation, and the delay or impossibility of passive and active motion in patients (all circumstances favoring heterotopic ossification).
We believe that the higher prevalence of HO in severe COVID-19 could serve as a stress marker of the healthcare system. We think it is relevant to conduct future research to assess this association.

