











 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
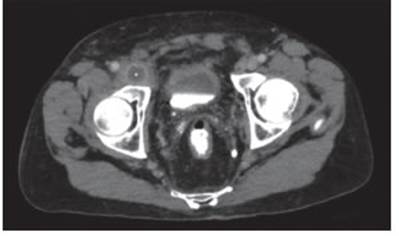
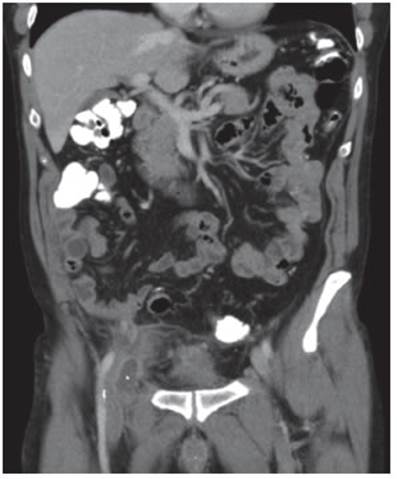
PermalinkA 68-year-old patient with a history of laparoscopic radical prostatectomy consulted the emergency depart ment for groin pain and fever of 48 hours of evolution. Physical examination revealed an irreducible and pain ful tumor on palpation at the right inguinocrural level. An abdominal-pelvic CT was performed, which showed a mass with liquid content and signs of inflammation at the level of the subinguinal space, medial to the femo ral vein (Figure 1-2). The main differential diagnoses pro posed were complicated crural hernia and abscessed adenopathy of the proximal deep inguinal node [Cloquet’s node or Rosenmuller’s node]. In view of the diagnostic doubt and the regular condition of the patient, it was decided to perform an exploratory laparoscopy where the presence of a complicated crural hernia was ruled out. Subsequently, ultrasound of the inguinocrural region and puncture of the hypoechoic image in the right crural re gion were performed, extracting 15 ml of pus which was sent for culture and cytology. The patient evolved favor ably and was discharged on the second postoperative day.
Cloquet’s lymph node lymphadenopathy should be considered among the multiple differential diagnoses of an inguinocrural mass in the emergency. Exploratory laparoscopy is a minimally invasive method that allows us to rule out the presence of complicated hernia when there is diagnostic doubt, prioritizing patient safety.

