











 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkKEY POINTS
Current knowledge
• Lower limb peripheral artery disease (PAD) is associated with an increase in morbidity and mortality in the general population. However, women have been underrepre sented in the different studies, with scarce evidence regarding the prognosis of this gender on PAD.
Article contribution
• Women with symptomatic PAD undergoing lower limb revascularization are older and present a more advanced disease with wor se prognosis than men in terms of all-cause mortality and re-hospitalizations for chro nic limb-threatening ischemia rates. There fore, it is essential to achieve an adequate control of cardiovascular risk factors, as well as to optimize medical treatment in female patients.
Introduction
Lower limb peripheral artery disease (PAD) is characterized by stenosis or occlusion of one or more arteries from the aortic-iliac segment to the foot, with clinical manifestation of intermittent claudication (IC), chronic limb-threatening ischemia (CLTI) or acute limb ischemia (ALI)1. Although numerous etiologies may explain PAD, atherosclerosis stands out as its main cause2,3.
Despite the growing understanding of PAD as an important cause of cardiovascular morbidity and mortality, it has been less studied than cor onary or cerebrovascular diseases4. Effectively, the global prevalence of PAD has increased by 45% from the year 2000 to 2015, with a greater impact in underdeveloped countries (58% vs. 18%, respectively)5.
Women are frequently underrepresented in scientific studies concerning the efficacy and safety of symptomatic lower limb PAD revas cularization. In addition, there are few studies of cohorts evaluating PAD differences between genders. This is mainly due to its oligo symp tomatic course or with atypical symptoms in women, favoring underdiagnosis6. In this sense, the American Heart Association (AHA) has pos tulated strategies to improve the knowledge of basic and clinical vascular biology as a function of gender for a correct PAD diagnosis and treat ment7.
Additionally, the fact that PAD is a disease whose incidence increases with age and that the female gender prevails in a predominantly older population represents an opportunity to better understand the prognosis of women undergoing symptomatic PAD interventions8.
The purpose of this study was thus to deter mine the prognosis and outcome of women un dergoing a symptomatic PAD revascularization procedure.
Materials and methods
Study population and design
This was a retrospective cohort study including pa tients over 18 years of age with symptomatic lower limb PAD requiring percutaneous or surgical revascularization carried out at a university hospital of the Autonomous City of Buenos Aires from 2014 to 2020.
Symptomatic PAD was defined as the presence of pain during exertion or at rest and/or trophic lesion of the lower limbs associated with angiographic documentation of hemodynamically significant lesion9. The clinical pre sentation of symptomatic PAD was classified as IC, CLTI or ALI. IC was described as lower limb fatigue, discomfort or pain manifested during activity and relieved by rest10. CLTI was considered as the presence of pain at rest and/or cutaneous lesions (ulcer or gangrene) of more than 2-week evolution11. ALI was defined as the sudden de crease of perfusion of less than 2-week evolution, typical ly characterized by pain, paresis or paralysis, paresthesia, pulselessness, lower temperature and/or pallor, threaten ing limb viability12.
Cases of lower limb revascularization secondary to iat rogenic, inflammatory or traumatic causes were excluded from the study, as atherosclerosis was the main focus of the analysis.
Endpoints of the study
The primary endpoint was the comparison of all-cause mortality between men and women undergoing symptomatic lower limb PAD revascularization. The sec ondary endpoints considered were: re-hospitalization for CLTI, major amputation (defined as supra-malleolar amputation)13, non-fatal stroke (both ischemic-classified as cerebral ischemia due to thrombosis, embolism or hypo-perfusion- and hemorrhagic due to non-fatal in tracranial bleeding or subarachnoid hemorrhage)14, non-fatal acute myocardial infarction (AMI) (described as acute myocardial injury with elevated biomarkers and evidence of nonfatal myocardial ischemia)15 and MACE (composite endpoint of death, nonfatal AMI and nonfa tal stroke).
Data were collected from the electronic medical re cords of our center.
Statistical analysis
The Kolmogorov-Smirnov test was used to analyze Gaussian distribution of the variables. Continuous vari ables were expressed as mean ± standard deviation or as median and interquartile range (IQR), as appropriate, and compared using Student’s t test in the former case and the Man Whitney test in the latter.
Categorical variables were presented as absolute value and percentage, and were compared using the chi-square test or Fisher´s exact test, as appropriate. A bivariate lo gistic regression analysis was performed to assess the independent association between different variables and the endpoint of interest. Variables presenting p < 0.1 or considered as potential confounders were included in the multivariate logistic regression. Likelihood-ratio test was performed to compare multivariate analysis models. Sur vival was expressed using the Kaplan-Meier curve and the Log-Rank test. Hazard Ratio was estimated by mul tiple Cox regression, also adjusting by the same variables. Statistical significance was considered for p < 0.05. SPSS 25 (IBM, Armonk, NY, USA) was used for the statistical analyses.
Ethical considerations
The present study complies with the principles de scribed in the Declaration of Helsinki16. This study was approved by the Hospital Italiano Institutional Review Board (protocol number 6792 and PRIISA registration code 10354). The informed consent was waived considering the retrospective nature of the study.
Results
A total of 309 patients were included in the study with median follow-up of 1.9 years (IQR 25-75%: 0.3-3.7 years). In 35.3% of cases (N = 109) patients belonged to the female gender. The gen eral population characteristics are described in Table 1. Women were older compared with men (75.6 ± 11.2 years vs. 69.8±10.6 years, p < 0.01). Conversely, women presented lower prevalence of smoking (48.6% vs. 67.5%, p < 0.01), diabetes (18.3% vs. 37.2%, p < 0.01), chronic kidney dis ease (8.3% vs. 25.8%, p < 0.01) and myocardial infarction (11% vs. 28.4%, p < 0.01) than men. Medical treatment prior to lower limb revascu larization showed no statistically significant dif ferences in the use of antiplatelet agents (aspi rin: 76.4% vs. 67.9%, p = 0.11; clopidogrel: 54.6% vs. 51.4%, p = 0.59) or statins (77.9% vs. 70.6%, p = 0.16). Neither were there differences in the form of clinical presentation (Table 2) and type of revascularization procedure (percutaneous or surgical) (Table 3) between both genders.

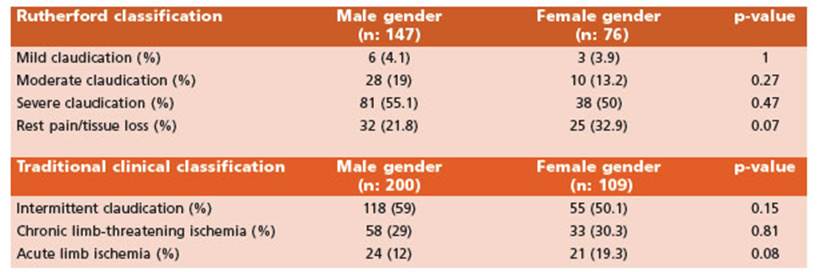
Table 2 Clinical presentation according to Rutherford classification and traditional clinical classification

Regarding the primary endpoint, women presented greater rate of all-cause mortality than men (22% vs. 12%, p = 0.02) (Table 4, Fig. 1). Mortality was significantly higher among women after adjusting for age and chronic kidney disease (OR 2.19 [95% CI: 1.06-4.51], p = 0.03). In addition, in the analysis of time-to-event (all-cause death), female gender ex hibited 93% higher risk of suffering death than men, when adjusting by the above-mentioned relevant clinical variables (HR 1.93 [95% CI: 1.04-3.56], p = 0.04) (Table 5).

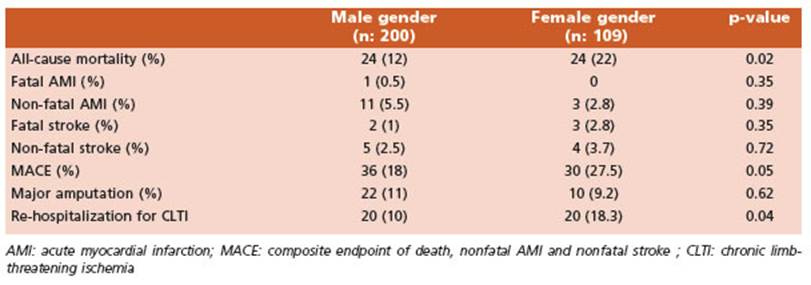

Regarding the secondary endpoints, women evidenced higher rate of re-hospitalization for CLTI (18.3% vs. 10%, p = 0.04), without statistical ly significant differences in the rest of the final endpoints analyzed, such as major amputation, AMI, stroke and MACE (Table 4).
Discussion
The present work analyzed the underlying comorbidities, the different forms of clinical presentation, and the prognosis of lower limb PAD revascularization according to gender. The main findings of our study were: a) women were older but with less comorbid conditions (lower prevalence of smoking, diabetes, chronic kidney disease and myocardial infarction); and b) wom en presented higher rate of all-cause mortality and re-hospitalization for CLTI compared with men. This difference in all-cause mortality was preserved even after adjusting for age and pres ence of chronic kidney disease.
In our study, female gender represented 35.3% of the population, in agreement with pre vious randomized and prospective cohort stud ies of subjects undergoing symptomatic lower limb PAD revascularization, where women represent 32% to 43% of the population7,17. The results of the present study are similar to pre viously published works regarding the clinical characteristics according to gender at the time of revascularization. Women undergoing low er limb revascularization are generally older and have less comorbidities (including diabe tes, smoking and coronary heart disease)8. The manifest relationship between age and female gender in lower limb PAD development is of particular interest. In this sense, evidence suggests that the hormonal factor plays a key role in its etiopathogenesis. Effectively, estrogens act as a protective factor reducing the risk of developing atherosclerosis until menopause, time in which this “protection” is lost and the risk of cardiovascular risk increases18. The fact that women with lower limb PAD who will un dergo revascularization present with older age could be the reason for a more advanced dis ease in this group, explaining in part the great er rates of mortality and re-hospitalization for CLTI observed in our study. Moreover, these results are similar to evidence reported in the literature8,19-21. On the one hand, although we did not find differences between genders in antiplatelet, lipid-lowering and hypertensive treatment, the degree of control of the different cardiovascular risk factors and the compliance with blood pressure and metabolic (such as LDL cholesterol levels) objectives were not ex plored in our study, and there is evidence that women have less probability of attaining these goals19. Because medical treatment in women is less optimal than that in men places the for mer at higher risk of cardiovascular events and death after lower limb revascularization19. An other hypothesis could consist in the factors that delay the time to diagnosis. Since oligosymptomatic PAD manifestation mainly occurs in women, it could justify a later consultation and consequently worse outcomes as a result of disease progression22. However, we have not found differences in terms of presentation symptoms according to the Rutherford classification. On the other hand, symptoms could initially be masked or misinterpreted as arthri tis, osteoporosis, or spinal stenosis, which are more prominent in female gender. In addition, there are differences in the distribution of body fat among men and women: the latter tend to have more fatty deposits in the lower limbs and hips. These sex-related characteristics may lead an erroneous conclusion when examin ing a woman with PAD22. In addition, there is evidence that women with PAD present greater prevalence of depression. The presence of this condition would facilitate the underdiagnosis of peripheral vascular disease in women due to the absence of controls and timely consulta tion, thus delaying diagnosis, as well as favor ing lower adhesion to medical treatment23.
Finally, despite our study has limitations due to its design and variables analyzed (the asso ciated depression, the control of cardiovascular risk factors and the anatomical characteristics of vascular lesions between both genders were not evaluated), we believe that it is relevant, as it allows assessing PAD behavior (less studied compared with coronary and cerebrovascular disease) in a gender underrepresented in most studies.
In conclusion, women with symptomatic PAD undergoing lower limb revascularization are older and present a more advanced disease with worse prognosis than men. It is therefore essen tial to achieve medical treatment optimization in the female gender, since PAD not only has a negative impact on the quality of life, but also on women survival, which is independent of age.

