Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkA 39-year-old male patient was admitted to the ICU with acute respiratory failure and required mechanical ventilation. He had a history of severe immunosuppres sion due to chronic myeloid leukemia treated with nilo tinib, as well as a prolonged postoperative hospitalization after a deceased-donor kidney transplant for membra noproliferative glomerulonephritis. To address humoral rejection, he received multiple pulses of methylpredniso lone and thymoglobulin. Chest computed tomography revealed hazy opacities in both upper lobes and small nodules with a centrilobular distribution, indicating an inflammatory/infectious process.
A video-bronchoscopy and a bronchoalveolar lavage (BAL) was performed. During the exploration of the air way, grouped vesicles on an erythematous base were ob served in the lower third of the trachea, extending into the right main bronchus and the right upper lobe. Ad ditionally, a shallow ulceration was noted in the apical segment (B1) of the right upper lobe. The remaining sec tions of the bronchial tree appeared unaffected (Fig. 1 and Video).

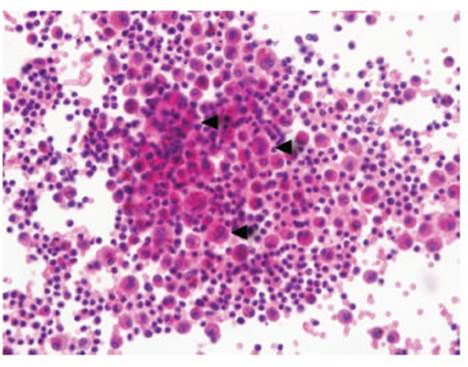
Real-time polymerase chain reaction of BAL fluid de tected the presence of Human Herpesvirus 6 DNA. BAL cytology revealed inflammatory smears with polymor phonuclear cells (76%), lymphocytes (14%) and macro phages (10%), isolated cells with nuclear clearance and no evidence of multi-nucleation or classic cytopathic vi ral inclusions (Fig. 2).