










Servicios Personalizados
Revista

Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO
Links relacionados
-
 Similares en
SciELO
Similares en
SciELO
Compartir

 Permalink
PermalinkArchivos argentinos de pediatría
versión impresa ISSN 0325-0075versión On-line ISSN 1668-3501
Arch. argent. pediatr. vol.114 no.3 Buenos Aires jun. 2016
http://dx.doi.org/10.5546/aap.2016.248
BRIEF REPORT
http://dx.doi.org/10.5546/aap.2016.eng.248
Osteogenesis imperfecta: Level of independence and of social, recreational and sports participation among adolescents and youth
Mercedes Rodríguez Celin M.D.a and Virginia Fano M.D.a
a. Department of Growth and Development, Skeletal Dysplasia Office, Hospital de Pediatría "Prof. Dr. Juan P. Garrahan", Buenos Aires, Argentina.
E-mail address: Mercedes Rodríguez Celin, M.D.: mercedesrodriguezcelin@gmail.com
Funding: None.
Conflict of interest: None.
Received: 11-03-2015
Accepted: 01-11-2016
ABSTRACT
Introduction. Osteogenesis imperfecta is a group of hereditary connective tissue disorders that cause bone fragility, with a wide clinical variability resulting in varying degrees of motor disability.
Objectives. To describe the level of independence and of social, recreational and sports participation among adolescents with osteogenesis imperfecta.
Population and methods. Descriptive, analytical and crosssectional study conducted in patients with osteogenesis imperfecta older than 15 years old attending the Skeletal Dysplasia Office of Hospital "Prof. Dr. Juan P. Garrahan" (May 2013 through December 2014). Self-administered survey. Short stature was an outcome measure that indicated severity.
Results. There were 18 patients; age: 19.17 (±3.4 sDE); 83% had moderate-severe forms of OI; median height: -7.9 sDE; 50% used a wheelchair.
Average education years: 12.2; 56% participated in sporting activities; and 78% were involved in recreational and social activities. A high level of independence was observed.
We found a correlation between short stature and use of wheelchair (r: -0.77) and between short stature and participation in sporting activities (r: 0.66). No correlation was observed with years of education (r: -0.15), participation in social activities (r: -0.22) or recreational activities (r: 0.35).
Key words: Osteogenesis imperfecta; Adolescent; Social participation; Recreational activities.
INTRODUCTION
Osteogenesis imperfecta (OI) is a group of hereditary connective tissue disorders that cause bone fragility.1 According to its etiology, this disease is directly or indirectly related to type I collagen,2 and has a prevalence of 1 in every 12 000-15 000 newborn infants (NBIs).3
It has a wide clinical variability. The original classification made by Sillence in 1979 into type I, II, III and IV was modified by Dijk and Sillence in 2014 based on the clinical severity of OI into mild, moderate, severe and extremely severe.1 The severe forms usually show multiple fractures observed before birth and lead to skeletal deformities and complications. Other common signs include variable degrees of short stature, dental alterations and hearing loss. OI is not associated with intellectual disability.4
There is no single therapeutic scheme for OI; management should be adapted to each individual and agreed among the multidisciplinary medical team, the patient and his/her family.3,5
A study conducted in 2011 at the Shriners Hospital for Children Canada that caters for patients with OI conducted a survey to assess the level of independence and of social, recreational and sports participation among 24 adolescent and young adult patients with OI.4
We believe that having a broader picture of these aspects regarding our group of patients with OI may help us improve treatment strategies.
OBJECTIVE
To describe the level of independence and of social, recreational and sports participation among youth with OI.
POPULATION AND METHODS
This was a descriptive, analytical, crosssectional study.
All patients with OI, older than 15 years old and attending the Skeletal Dysplasia Office of Hospital "Prof. Dr. Juan P. Garrahan" (May 2013 through December 2014) were assessed. The following clinical outcome measures were evaluated: age, sex, type of OI, zH. The latest classification published by van Dijk1 was used. All patients were invited to complete a self-administered survey, which had been translated from the version prepared by the Shriners Hospital for Children Canada.4 The translation was done by one of the authors and then tested in three patients for comprehension, after which minimal grammar corrections were made. Before the survey was completed, patients gave their verbal consent to participate.
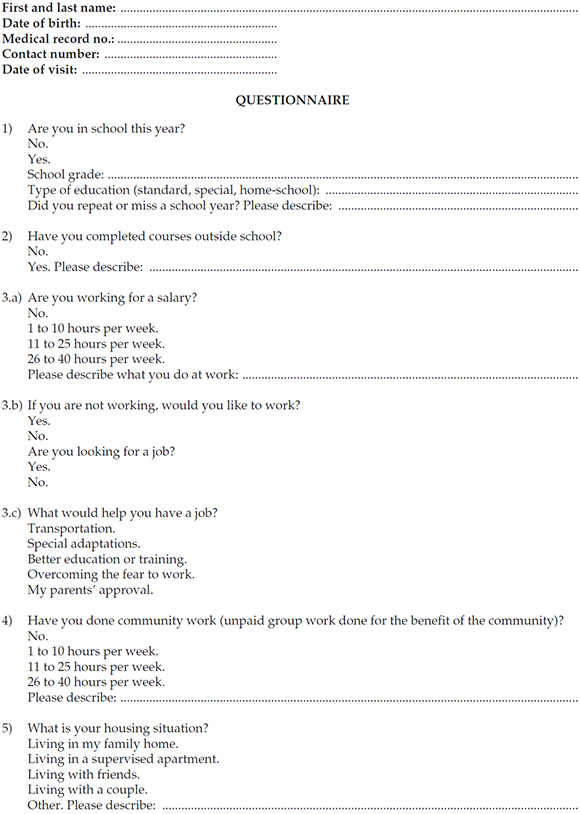
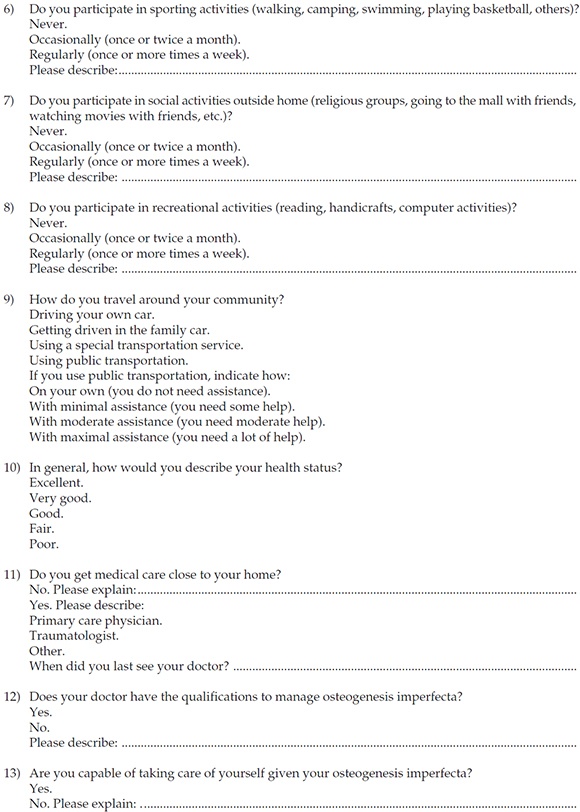
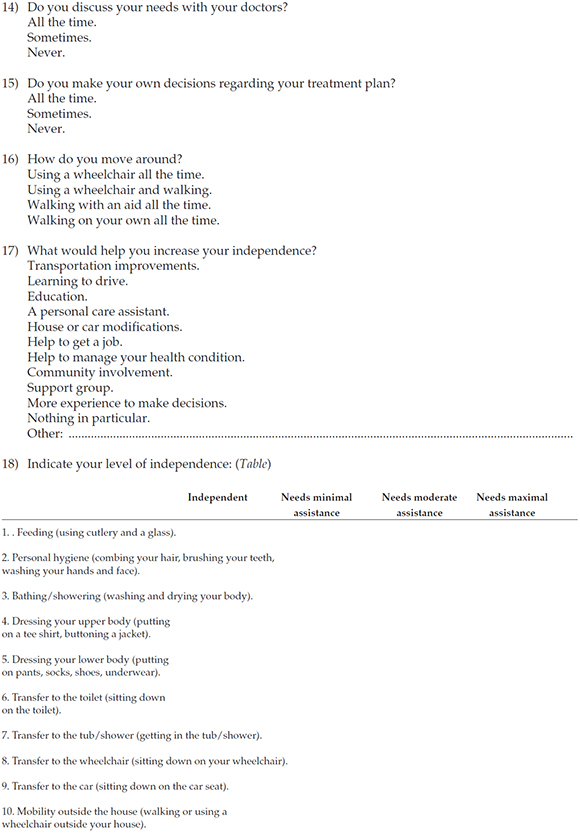
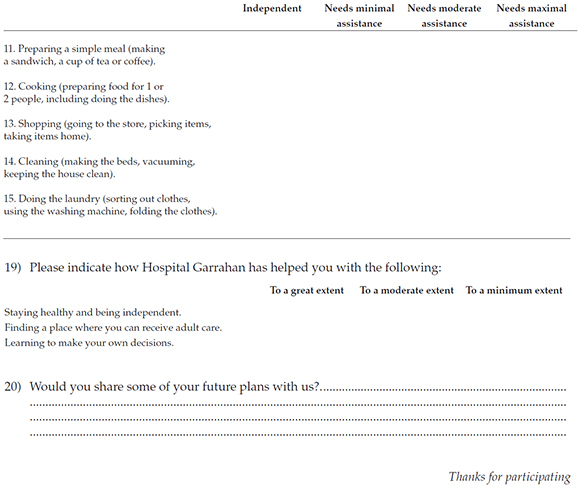
The survey included 20 questions. Questions 1-17 and 19 asked about education and work achievements, housing, transportation, relationship with the hospital and social, recreational and sports participation. Questions were close-ended, with single or multiple choice answers, depending on the question. Question 18 assessed 15 items regarding mobility, self-care and activities of daily living. These items were scored using a four-point scale (from requiring maximal assistance to being independent) and were selected from two different instruments: the Functional Independence Measure (FIM) and the Instrumental Activities Measure (IAM).6 The FIM assesses physical and cognitive impairment. The IAM was developed as a supplement to the FIM to obtain information on the level of independence. Question 20 was open-ended and asked about future plans. A copy of the questionnaire is attached in the Annex.
The measured height Z score (zH) was used as an outcome measure that indicated severity (a shorter stature meant a worse severity). The independent outcome measure used for correlations was zH. A correlation with the following selected outcome measures from the survey was sought: use of wheelchair, participation in social activities (involvement in religious groups, going to the mall or watching movies with friends, etc. ), sporting activities (walking, swimming, playing basketball, etc. ), recreational activities (reading, handicrafts, computer activities, etc. ), and number of completed school years (completed years of mandatory education: as of 5 years old).
Statistical analysis
Data were summarized using central tendency and dispersion, as applicable. Spearman's correlation coefficient for nonparametric outcome measures was used to correlate zH to the different selected outcome measures.
RESULTS
General characteristics of the sample
All patients agreed to complete the questionnaire, which was self-administered by all except one patient who required help due to his motor disability.
Eighteen patients with osteogenesis imperfecta older than 15 years old were included (11 boys); their mean age was 19.17 (±3.4 sDE).
Of them, 83% had moderate-severe OI and 17%, mild OI. Median zH was -7.9 sDE (-14.68/+1.5 sDE).
Questionnaire analysis
To move around, 50% of patients used a wheelchair all the time, 17% combined a wheelchair with a walking aid, and 33% walked on their own.
In relation to education level, work, housing and transportation, the average number of completed school years was 12.2, and 78% were in school. Among patients older than 18 years old (11 patients), 36% were working, 69% would like to work, and 24% believed that they required adaptations. Also, 89% lived in their family house, and 78% used public transportation, but only 29% did so in an independent manner. Only one patient drove his own car. Fifty percent got driven the family car.
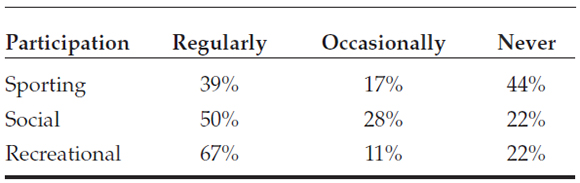
Participation in social, recreational and sporting activities is described in Table 1.
Table 1. Participation in sporting, social and recreational activities among adolescents with osteogenesis imperfecta (N: 18)
In relation to the perception of their own health status, their ability to manage OI and communication with the medical team, as well as their interaction with the health system outside our hospital, 55% of patients indicated that they had an excellent health status; 39%, that it was good; and only 1 patient, that it was fair. Sixty-six percent of patients received care close to their home, and 50% referred that their doctor had qualifications to manage OI. Also, 94% of patients felt capable of managing their condition, but 61% discussed their medical needs with their doctors only sometimes and 43% were always involved in making treatment decisions.
When asked to what extent our hospital had helped them feel healthy and independent, 95% of assessed patients indicated that it did to a great extent. In addition, 61% of patients indicated that the hospital helped them to make their own decisions to a great extent, but only 46% referred that it helped them to a great extent to find a hospital where they could receive adult care.
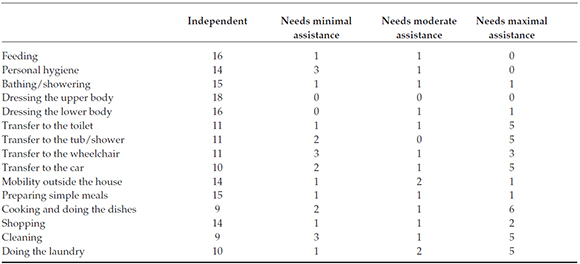
The level of independence in relation to mobility, self-care and activities of daily living is described in Table 2.
Table 2. Level of independence in relation to mobility, self-care and activities of daily living among patients with osteogenesis imperfecta (N: 18)
Participants were invited to share their plans for the future, and all but one wrote about them. The most common plans for the future included a wish to start or complete a university degree, work and have their own family.
Correlation between short stature and the different outcome measures
A short stature measured as Z score was used as a severity outcome measure. A negative correlation was observed between zH and wheelchair requirement (r: 0.77). The group with the higher level of participation in sporting activities was the one less affected by short stature (r: 0.66). No correlation was observed between zH and years of education (r: 0.15), participation in social activities (r: -0.22) or recreational activities (r: 0.35).
DISCUSSION
Weaknesses of our work include that the survey was not transculturally adapted and that the sample size was not large; however, given that OI is a rare disease, we believe that the resulting data may be useful.
It was observed that, to varying degrees, 78% of patients participated in social and recreational activities and no correlation was found between zH and the frequency of such participation. Data published by Montpetit4 are similar to our results: no differences were observed in social and recreational involvement among the different types of OI. Compared to those activities, sports were practiced to a lower extent, consistent with Montpetit's reports, who observed that patients with severe forms of OI practiced fewer sporting activities.4
The levels of independence as described by mobility, self-care and activities of daily living are high. Difficulties are consistent with those observed among patients with type III OI in the referenced publication.4
Cole8 suggested that, although OI is associated with a normal intelligence, it may have an impact on academic performance given its major physical involvement, pain and motor disability. In our group of patients, no correlation was observed between the number of completed school years and severity, consistent with the high level of academic achievement observed in other populations with OI as reported by Montpetit4 and Widmann.9
The review conducted by Thompson10 among adults with skeletal dysplasia described varying degrees of social isolation and its influence on the level of education attained. Attention should be paid to this aspect given that, in our study, 22% of patients referred that they never participated in social activities.
Future studies should focus on establishing how the level of independence and participation may affect the quality of life of patients with OI.11,12
Acknowledgments
We would like to thank Mariana del Pino, M.D. , for making a critical review of the article and her contributions.
ANNEX
1. Van Dijk FS, Sillence DO. Osteogenesis imperfecta: clinical diagnosis, nomenclature and severity assessment. Am J Med Genet A 2014;164A(6):1470-81. [ Links ]
2. Marini JC, Blissett AR. New genes in bone development: what's new in osteogenesis imperfecta. J Clin Endocrinol Metab 2013;98(8):3095-103. [ Links ]
3. Glorieux F. Guide to Osteogenesis Imperfecta for pediatricians and family practice physicians. Berhesda: National Institute of Health; 2007. [ Links ]
4. Montpetit K, Dahan-Oliel N, Ruck-Gibis J, Fassier F, et al. Activities and participation in young adults with osteogenesis imperfecta. J Ped Rehabil Med 2011;4(1):13-22. [ Links ]
5. Fano V, Rodriguez Celin M, del Pino M, Buceta S, et al. Osteogénesis imperfecta. Evaluación clínica, funcional y multidisciplinaria de 65 pacientes. An Pediatr (Barc) 2010;72(5):324-30. [ Links ]
6. Grimby G, Andrén E, Holmgren E, Wright B, et al. Structure of a combination of Functional Independence Measure and Instrumental Activity Measure Items in community-living persons: a study of individuals with cerebral palsy and spina bifida. Arch Phys Med Rehabil 1996;77(11):1109-14. [ Links ]
7. Ben Amor IM, Glorieux FH, Rauch F. Genotype-phenotype correlations in autosomal dominant osteogenesis imperfecta. J Osteoporos 2011;2011:540178. [ Links ]
8. Cole DE. Psychosocial aspects of osteogenesis imperfecta: an update. Am J Med Genet 1993;45(2):207-11. [ Links ]
9. Widmann RF, Laplaza FJ, Bitan FD, Brooks CE, et al. Quality of life in osteogenesis imperfecta. Int Orthop 2002;26(1):3-6. [ Links ]
10. Thompson S, Shakespeare T, Wright MJ. Medical and social aspects of the life course for adults with a skeletal dysplasia: a review of current knowledge. Disabil Rehabil 2008;30(1):1-12. [ Links ]
11. Fano V, Del Pino M, Rodríguez Celin M, Buceta S, et al. Osteogénesis imperfecta: estudio de la calidad de vida en los niños. Arch Argent Pediatr 2013;111(4):328-31. [ Links ]
12. Hill CL, Baird WO, Walters SJ. Quality of life in children and adolescents with Osteogenesis Imperfecta: a qualitative interview based study. Health Qual Life Outcomes 2014;12:54. [ Links ]

