











 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkRight-sided infective endocarditis is a rare but potentially fatal disease. It comprises 5-10% of the to tal number of infective endocarditis events. It is most frequently associated with intravenous drug use, and occurs less frequently in patients with venous access, intravascular devices or underlying congenital heart disease, and exceptionally in non-addict patients or in patients without cardiac malformations. 1
We report the case of a 58-year-old male patient with hypertension, dyslipidemia, and a history of aortic valve replacement with mechanical prosthesis due to aortic stenosis in 2019.
He is admitted to the general ward for febrile syn drome under study. Cardiac physical examination reveals neither changes in heart sounds nor signs of congestive heart failure. ECG shows sinus tachycardia and first-degree atrioventricular block (PR inter val 220 msec).
Blood screening on admission shows white blood cells 31 840/mm3 (neutrophils 96%, lymphocytes 1.7%), C-reactive protein 58.9 mg/L (normal range 0-5), pro calcitonin 4.55 ng/mL (normal range 0-0.1), total bili rubin 1.33 mg/dL, indirect bilirubin 0.83 mg/dL, and direct bilirubin 0.50 mg/dL.
During hospitalization, methicillin-susceptible Staphylococcus aureus is detected in blood cultures. Due to suspicion of infective endocarditis, a transesophageal echocardiogram is performed, that detects no vegetations, and normal mechanical valve func tion. On the fourth day of antibiotics, further blood cultures detect no bacterial growth; on the tenth day, transesophageal echocardiography shows no vegeta tions in the heart valves, ruling out infective endocarditis. After receiving intravenous antibiotics during 14 days, patient is discharged.
A week later, he is readmitted for fever and general malaise; ECG reveals further PR interval prolongation (270 msec) (Figure 1A). Blood screening shows white blood cells 11 870/mm3 (neutrophils 87%, lymphocytes 4.7%), C-reactive protein 25.6 mg/L, procalcitonin 0.19 ng/mL, erythrocyte sedimentation rate 32 mm/h. Methicillin-susceptible Staphylococcus aureus is isolated in follow-up blood cultures. Transthoracic echocardiography reveas a 0.6 cm x 0.6 cm mobile image at the tricuspid valve level. Transesophageal echocardiogra phy (TEE) confirms 0.9 x 0.6 cm vegetation at the level of the septal leaflet, mild tricuspid regurgitation, and normal prosthetic valve function (Figure 2).
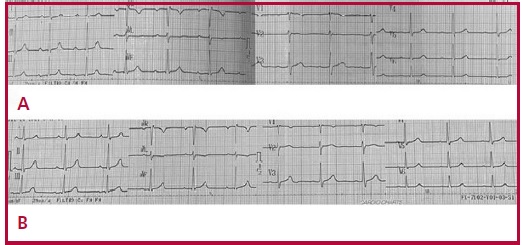

A conservative approach with intravenous cefazolin for 6 weeks is followed. First-degree AV block im proves by the fifth week of antibiotic treatment (Fig ure 1B). Follow-up transthoracic echocardiograms on the second and sixth weeks of treatment show no evidence of tricuspid vegetation.
Outpatient positron-emission tomography/computed tomography (PET/CT) for suspected prosthetic valve involvement reveals moderate diffuse radio tracer uptake at the level of the replaced aortic valve, suggesting the absence of an active infectious process, given the absence of a dominant focus with increased concentration of the contrast material and SUVmax 3.5 (Figure 3).
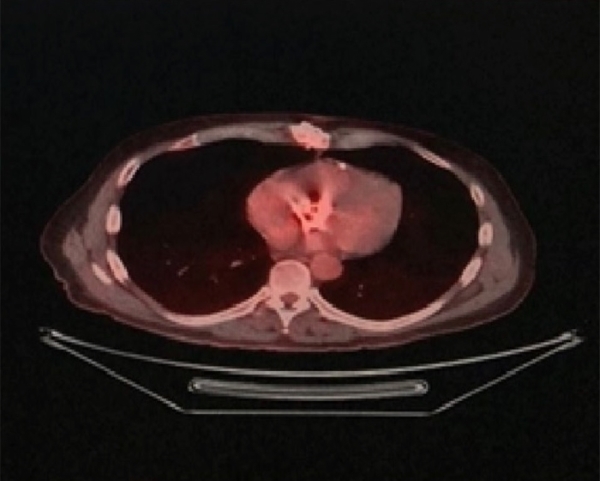
Fig. 3 PET/CT with fluorine-18 deoxyglucose: transverse projection. Diffuse uptake in the aortic prosthesis is observed.
Right-sided infective endocarditis is common in injecting drug addicts and in patients with cardiac malformations; it is a potentially serious condition, with a mortality rate between 23 and 31%. Simultaneous left and right-sided endocarditis comprises 13% of the cases, whereas right-sided endocarditis alone affects 10%. (1, 2)
Isolated native tricuspid valve endocarditis (NTVE) usually occurs spontaneously, without evident history of dental or surgical procedures; however, the skin is usually the most common portal of entry (particularly in the case of S. Aureus). In this clinical case, the predisposing factor could not be identified. Staphylococcus aureus is the most commonly isolated infectious agent (70% of cases), followed by Streptococcus and Enterococcus. 3
The clinical presentation invariably consists of persistent fever associated to pulmonary events, anemia and microscopic hematuria (tricuspid syndrome of Nandakumar and Raju). The absence of peripheral stigmata of endocarditis or relevant murmurs in most cases is noteworthy. 4
If fever is persistent (if it remains after a 2-week course of antibiotics) it is usually associated with perivalvular extension of infection, new septic emboli or superimposed nosocomial infection. The clinical pic ture, positive findings on blood culture and echocardiography are the main diagnostic tools in NTVE. 4
The usefulness of PET/CT is significantly greater for prosthetic valve endocarditis than for native valve infective endocarditis and is an excellent alternative in case of negative or doubtful ultrasound scans. In tegrating PET/CT as a diagnostic tool in endocarditis allows for reclassification of 76% of patients with prosthetic-valve infective endocarditis from "possible" to "definite". 5
Eighty percent of isolated NTVE patients are successfully treated with medical therapy. However, surgery is recommended in uncontrolled infection or right heart failure with tricuspid regurgitation refractory to treatment. Surgical treatment repairs the valve dysfunction and eliminates the infectious focus, thus contributing to reduce mortality associated with heart failure. 6
Regarding prognosis, a high success rate is achieved with medical treatment (antibiotics), the development of heart failure is uncommon, and only 25% of cases require valve replacement or surgery. 1 Mortality associated with isolated NTVE is lower than that reported for endocarditis with a predisposing condition. 6
This case suggests the need to consider isolated NTVE, its clinical presentation, treatment, and prognosis, as well as the usefulness of PET/CT to confirm prosthetic valve involvement.

