











 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkINTRODUCTION
Regardless several criteria have been described, the differential diagnosis between orthodromic reentrant tachycardia (ORT) through an occult accessory pathway (AP) and atypical intranodal reentrant tachycardia (ANRT) can be challenging. 1-15 The usefulness of these techniques usually depends on certain factors, such as sustained tachycardia and the distance from the stimulation site to the tachycardia circuit, as well as on certain conditions, as an adequate bundle of His recording or capture, and that the tachycardia is not interrupted by stimulation maneuvers or post- stimulation interval correction due to atrioventricular (AV) nodal delay caused after entrainment from the right ventricle (RV).
Conceptually, these techniques are based on localization, size and distance of the circuit to certain structures as the His bundle, the apex, or basal portions of the RV, and have not been focused on the electrophysiological components of each circuit. ORT and ANRT use AV nodal tissue as antegrade limb of the tachycardia circuit. However, this is not the case for the retrograde limb. Although retrograde conduction runs by an AP in ORT, it travels through a slower pathway of the AV node in ANRT (both in the slow-slow as in the fast-slow forms). Therefore, retrograde conduction properties are different in ORT, typically independent of heart rate (HR), from typically decremental or dependent on HR in ANRT.
The abrupt change in HR that occurs at tachycardia onset causes changes in the conduction properties and refractoriness of the involved tissues. Our hypothesis is that this difference in retrograde conduction between ORT and ANRT can be better evidenced during tachycardia induction, in terms of greater retrograde conduction time variability in the first beats of ANRT than in those of ORT. The objectives of the study were to systematically analyze and compare retrograde conduction time variability at the start of ANRT and ORT, and find a cut-off value that constitutes a new diagnostic tool to differentiate between these two arrhythmias. Additionally, we included a few patients with ORT mediated via a decremental conduction AP and a group of patients with typical NRT (tNRT). The analysis of tNRT was not carried out for diagnostic purposes, but with the objective of performing a pathophysiological description of retrograde conduction behavior in different types of paroxysmal supraventricular tachycardia (SVT).
METHODS
Study population
Patients with SVT referred for electrophysiological study were included in the analysis. Irregular tachycardia, preexcitation during sinus rhythm, atrial tachycardia, two coexistent mechanisms of arrythmia (e.g. ANRT with AP) and previous ablation were considered exclusion criteria. Since bundle branch block prolongs the ventriculoatrial (VA) in ORTs that use an ipsilateral AP, patients with transient bundle branch block after induction were also excluded. No patient had structural heart disease. The study was approved by the Ethics and Research Committees of the participating centers.
Electrophysiological study
After obtaining the informed consent, an electrophysiological study was performed in fasting patients under local anesthesia, without sedation. All antiarrhythmic drugs were discontinued for at least 5 half-lives before the study. Surface and intracavitary electrophysiological tracings were recorded in a digital polygraph, and blindly electronically analyzed at 200 mm/s by two electrophysiologists. In these conditions, the expected measurement margin of error of intracardiac intervals is considered to be ±5 ms at 100 mm/s and less at greater speeds (±1 ms at 400 mm/s). 16
The diagnosis of NRT and ORT was performed according to standard electrophysiological criteria, 2,5-15,17-19 and the ablation outcome. A fast-slow ANRT was considered when the AH interval was <180 ms and the AH/HA ratio <1 during tachycardia. 20-22 The criteria for a successful ablation were: no tachycardia inducibility, elimination of AP conduction in ORT and exclusion of sustained conduction via the slow pathway in ANRT. Supraventricular tachycardia was induced through programmed atrial or ventricular stimulation. Isoproterenol was administered if tachycardia was non-inducible or not sustained.
Variability of retrograde conduction time was measured to evaluate the VA intervals of the first beats after tachycardia induction, until this interval was stabilized. A stable VA interval was assumed when its duration was not modified for 3 consecutive beats and was equal to the VA interval of the established tachycardia. The VA interval was measured from the beginning of the QRS interval in a surface lead to a bipolar septal atrial electrogram (usually proximal coronary sinus). We preferred coronary sinus recordings since the ventricular electrogram is far field and low voltage, and the coronary sinus recording allows a clear identification of atrial electrogram onset and its stable position. Maximum and minimum VA interval (VAmax and VAmin) were identified and ∆VA was calculated for each type of tachycardia (∆VA=VAmax - VAmin), independently of the stable VA interval. The number of beats necessary for VA interval stabilization was also assessed.
Statistical analysis
Discrete variables were expressed as percentages and continuous variables as mean ± standard deviation or median and interquartile range (IQR 25-75) according to their distribution. The chi-square test or Fisher’s exact test was used for discrete variables and the Mann-Whitney U test for continuous variables. Sensitivity, specificity, and positive and negative predictive values (PPV, NPV) were calculated using the electrophysiological study diagnosis as gold standard. The area under the ROC curve (AUC) for ∆VA and the number of beats needed for VA stabilization variables was calculated to differentiate between ORT and ANRT. Youden’s J statistic was considered to find the best cut-off point for these variables. 23 A p value <0.05 was considered as statistically significant. IBMSPSS v.26 (Armonk, NY, USA) was used to perform the analyses.
RESULTS
A total of 156 patients (73 men) with median age 46 (29-65) years were included in the study. Among them, 37 patients were diagnosed with ANRT and 64 had ORT via a classical occult fast conduction AP (Kent bundle), with septal (n=33), left lateral (n=30) or right lateral (n=1) localization. Six patients were also included with ORT via a decremental conduction AP (Coumel type) which were separately analyzed. The remaining 49 cases formed the group with tNRT.
ANRT analysis
All ANRTs had some degree of variability in the time of retrograde conduction, i.e. no ANRT exhibited a fixed VA interval. Median ∆VA was 40 (21-55) ms and the VA interval stabilized in 5 (4-7) beats (Figure 1).
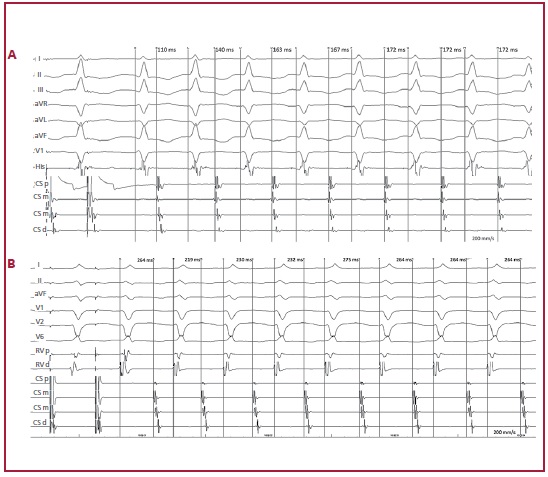
Fig. 1 ANRT induction in 2 different patients. A: Induction by programmed atrial stimulation. The VA interval stabilizes in the 5th beat and ∆VA is 62 ms (maximum VA interval: 172 ms; minimum VA interval: 110 ms). The VA interval was measured from the beginning of the QRS complex in V1 to the atrial electrogram in the proximal coronary sinus. The intracavitary recordings are bundle of His and proximal (p), medial (m) and distal (d) coronary sinus (CS). B: Induction by programmed atrial stimulation. The VA interval stabilizes in the 6th beat and ∆VA is 56 ms (maximum VA interval: 275 ms; minimum VA interval: 219 ms). The VA interval was measured from the beginning of the QRS complex in V2 to the atrial electrogram in the medial coronary sinus. The intracavitary recordings were proximal (p) and distal right ventricle (RV) and proximal (p), medial (m) and distal (d) coronary sinus (CS).
Comparison with ORT
Thirty-two (50%) ORTs displayed no variability in the VA interval (Figure 2), exhibiting a ∆VA interval of 0 (0-5) ms, significantly lower than in ANRT (p<0.001). The VA interval stabilized in 1.5 (1-3) beats, significantly before than in ANRT (p<0.001) (Table 1). These findings were similar in septal and free wall APs.
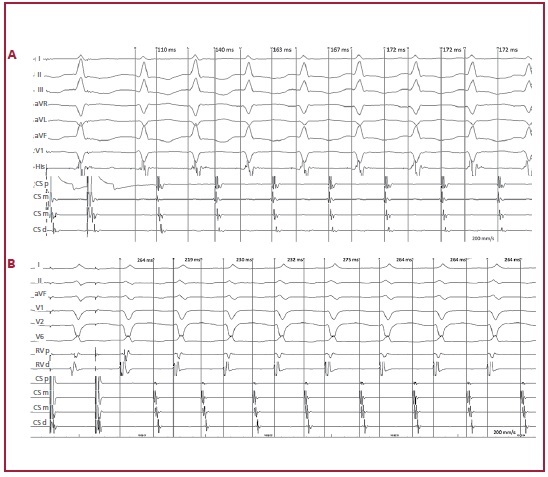
Fig. 2 ORT induction using a septal accessory pathway in 2 different patients. A: Induction by atrial extra stimulus over sensed rhythm. Tachycardia has a fixed VA interval from the first beat. ∆VA is 0 ms. The VA interval was measured from the beginning of the V2 complex to the atrial electrogram in the proximal coronary sinus. Intracavitary recordings are proximal (p), medial (m) and distal (d) coronary sinus (CS) and proximal (p) and distal (d) His bundle. B: Induction by programmed atrial stimulation. Tachycardia has a fixed VA interval from the first beat. ∆VA is 0 ms. The VA interval was measured from the beginning of the V2 complex to the atrial electrogram in the proximal coronary sinus. Intracavitary recordings are His bundle and proximal (p), medial (m) and distal (d) coronary sinus (CS).
No ORT had ∆VA10 ms. As shown in Figure 3, ∆VA <10 ms differentiated ORT from ANRT with 100% sensitivity, specificity, PPV and NPV. Stabilization of the VA interval in less than 3 beats identified ORT with 64.1% sensitivity, 94.6% specificity, 95.3% PPV, 60.3% NPV and AUC of 0.895 (Table 2).
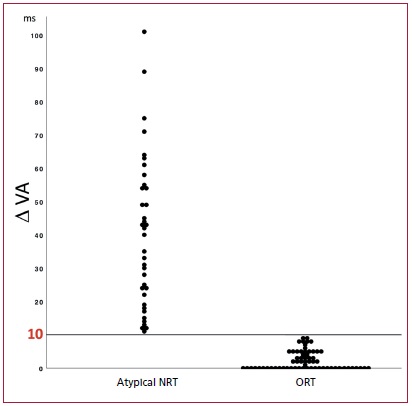
Fig 3. The scatter diagram shows individual ∆VA in ANRT and ORT. The 10 ms line represents the cut-off value to differentiate between these two arrhythmia mechanisms.
The comparison between ANRT and ORT via septal AP (n=33) presented similar results. A ∆VA <10 ms identified ORT with 100% sensitivity, specificity, PPV and NPV. Stabilization of the VA interval in less than 3 beats predicted ORT with 54.5% sensitivity, 94.6% specificity, 90% PPV, 70% NPV and AUC of 0.857 (Table 2).
Subgroup of patients with decremental conduction AP
In the six patients with decremental conduction AP, ∆VA was significantly lower (15 [5-20] ms; p=0.006) than in patients with ANRT, but the VA interval was stabilized in a similar number of beats (4 [3-7]; p=0.481). A ∆VA <20 ms identified these patients with 83.3% sensitivity, 74.2% specificity, 38.5% PPV, 95.8% NPV and AUC of 0.844. The ORTs via decremental pathways were compared with fast-slow ANRT, as they present with SVT with long RP. A ∆VA<20 ms predicted ORT mediated by decremental conduction pathways with 83.3% sensitivity, 73.3% specificity, 55.6% PPV, 91.7% NPV and AUC of 0.856.
Subgroup of patients with typical NRT
Forty-nine patients with typical NRT were included with the purpose of analyzing the characteristics of retrograde conduction via a fast pathway. All these patients showed some degree of variability in retrograde conduction time. ∆VA was 10 (6-16) ms and the VA interval was stabilized in 4 (3-4.5) beats. This represents an intermediate behavior of retrograde conduction. The variability of the VA interval (both in ∆VA as in the number of beats needed for its stabilization) was significantly lower than in ANRT and higher than in ORT (p<0.001 for both comparisons). Globally, the variability of the VA interval did not evidence an incremental or decremental behavior. On the contrary, the VA interval showed an unpredictable beat to beat prolongation or shortening until a stable duration was reached. Isoproterenol infusion was used to induce tachycardia in 15% of patients whose tachycardia was faster than in those without isoproterenol (cycle length of 306 ms vs. 354 ms; p <0.001), but ∆VA and the necessary number of beats for VA interval stabilization were not significantly different. The VA interval variability was similar in tachycardia induced by programmed atrial or ventricular stimulation.
DISCUSSION
Our study findings show that ORTs have minimum or null variability in the first VA intervals after tachycardia induction. Conversely, all ANRTs evidenced some degree of VA interval variability. This higher variability was manifested as a greater difference between the longest and shortest VA interval (∆VA), as well as in a higher number of beats needed to attain VA interval stabilization. A ∆VA <10 ms differentiated ORT from ANRT with 100% sensitivity, specificity, PPV and NPV. This is a highly relevant finding, mainly in cases of occult septal APs where the ablation strategies of the reentrant circuit differ substantially from those employed in ANRT.
Previous studies
Variability in the AV relation during tachycardia has been consistently associated with atrial tachycardia. 24,25 This can occur spontaneously or in response to stimulation aneuvers. Effectively, this criterion has been used to differentiate atrial tachycardia from NRT in which atrial activation is assumed as “associated” to ventricular activation. 1,5,24-26 This assumption has been considered for ORT throughout all publications on SVT.
A recent study showed changes in retrograde conduction time after fast-slow ANRT induction. 27 The authors reported shortening of the first HA interval compared with the HA interval of the established tachycardia. We analyzed all the VA intervals since the start of tachycardia until it attained a stable duration for 3 consecutive beats and included not only fast-slow ANRT but all ANRTs, as well as ORTs. As previously mentioned, VA interval variability in this study did not exhibit a uniform pattern (incremental or decremental).
In an analysis of 411 patients with typical and atypical NRT, Taniguchi et el. reported variations in the P-QRS relation during tachycardia. 28 The authors defined variation of the P-QRS relation during tachycardia as a change in the AH and HA intervals >20 ms, together with a change in the AH/HA ratio. This phenomenon was found in 19 % of cases with ANRT at tachycardia onset (only 3 patients) during a Wenckebach AV or 2:1 block, or at the end of spontaneous or secondary to adenosine administration tachycardia. This study did not include patients with ORT. VA interval variability at tachycardia induction had never been used as a criterion to distinguish ANRT from ORT. We analyzed the VA relation only at tachycardia induction, both in ANRT as in ORT, and found that all ANRTs had some degree of variability compared with only 50% in ORTs. ∆VA was <10 ms in all ORTs and in none of the ANRTs.
This is an easily applicable criterion without the usual limitations of the commonly used electrophysiological maneuvers (e.g. non-sustained tachycardia, termination during entrainment attempts, loss of capture during stimulation, or His bundle inadequate recording or capture). It can be evaluated measuring the initial VA intervals of tachycardia, without additional maneuvers. The only requisite that must be fulfilled is tachycardia induction.
The study of Obeyesekere et al. also focused on tachycardia induction to differentiate ORT from ANRT. They proposed applying during induction criteria that are used after entrainment (post-stimulation interval and stimulus-atrium interval), to manage non-sustained tachycardias. 29 However, the marked variability of the initial VA intervals in our study (VA=40 [21-55] ms in ANRT) may lead to a false diagnosis with this maneuver. Moreover, the criteria postulated by Obeyesekere is limited to tachycardias induced from the ventricle. Our findings were similar in tachycardias induced by atrial and ventricular stimulation. The fact that an adequate diagnosis was performed in a median of 5 beats since tachycardia induction, suggests the potential usefulness of VA interval variability in non-sustained SVT.
The value of ∆VA for ORT diagnosis is independent of AP localization. The usefulness of many diagnostic criteria described is lower in the presence of left lateral AP. 4,30-32
Possible mechanisms
As previously mentioned, the retrograde limb of the tachycardia circuit has different properties in ORT and ANRT. The refractory period is longer in the first tachycardia beat and progressively shortens when this starts. In this scenario, retrograde conduction via a slow nodal pathway can be less uniform and show different conduction times from the one occurring via an AP with all-or-none conduction. 33,34 Another possible explanation for VA interval variability in ANRT is the occult penetration of the extra stimulus that initiates the tachycardia, which results in different conduction times and degrees of refractoriness in the rest of the circuit. Occult conduction between fast and slow pathways was demonstrated in patients with dual AV nodal physiology. 35,36
Lastly, a final common superior pathway could be the seat of retrograde conduction changes. 37,38 Since tNRT had lower VA variability than ANRT, a different behavior of the final common pathway should be assumed in these two situations.
Limitations
Although ∆VA showed excellent diagnostic accuracy, it has some limitations. Irregular tachycardias were not included to avoid the influence of cycle length or antegrade conduction changes on retrograde conduction time. The value of our criterion lies in the identification of small changes in the initial VA intervals of a regular tachycardia. Tachycardias with transient bundle branch block were also excluded. The results of the present study do not apply in these two situations.
In addition, atrial tachycardias were also excluded from the study. Since these tachycardias may have VA interval variation, they must be ruled out by means of other criteria before performing the ANRT diagnosis.
CONCLUSION
Retrograde conduction time after SVT induction is significantly more variable (in terms of ∆VA and the necessary number of beats to reach VA interval stabilization) in ARNT than in ORT. A ∆VA <10 ms distinguished ORT from ANRT with 100% sensitivity and specificity. We present a new method, simple and accurate, which does not require additional maneuvers to tachycardia induction, and that should be employed to perform the differential diagnosis between ANRT and ORT, independently of AP localization.

