











 Español (pdf)
Español (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkINTRODUCTION
Hyponatremia is the most frequent hydroelectrolytic disorder in clinical practice -(1,2,11,310). It is defined as a serum sodium concentration less than 135 mmol/L -(1,2,11,310). It is present in 15-20% of emergency room and critical care patients -(1,2,11,310). The principal adverse events associated with hyponatremia are increased morbidity, hospital stay and mortality -(1,2,12,39,11). It has multiple causes and requires a systematic approach that includes classifying the patient's serum osmolality and volemia (3,7,9,10). Euvolemic hypotonic hyponatremia is the commonest form of presentation and the Syndrome of Inappropriate Antidiuretic Hormone Secretion (SIADH) its principal cause (3,7,9,10,13). This diagnosis requires to rule out other causes of hyponatremia including hypothyroidism and adrenal insufficiency -(3,710,13). In spite of this consideration, cortisol is not always measured during the study of euvolemic hyponatremia, underestimating the frequency of adrenal insufficiency as a cause of SIADH; misleading patients' therapy with potential adverse consequences-(25,79,1315). The authors present here a case series of hyponatremia associated with secondary adrenal insufficiency.
MATERIALS AND METHODS
This study was a retrospective analysis of clinical records of all the patients admitted with hyponatremia and secondary adrenal insufficiency to the ESE Hospital Universitario San Jorge from
Pereira, Colombia between January 2015 to September 2017. This case series was approved by the Ethics Committee of the Universidad Tecnológica de Pereira who waived the need for informed consent of the subjects, given that this was a historical review of patients records and no intervention was made, being classified as an investigation without risk according to national and international guidelines. The data collection was made following the good clinical practice and declaration of Helsinki recommendations.
Continuous variables were described with medians and interquartile ranges (IQR). Categorical variables were described as proportions. The presence of adrenal insufficiency manifestations defined as hypotension and hypoglycemia was actively searched among these patients. Hypotension was defined as a diastolic arterial blood pressure of 60 mm Hg or less, a systolic arterial blood pressure of 90 mm Hg or less, or a mean arterial blood pressure of 65 mm Hg or less. Hypertension was defined as a diastolic arterial blood pressure of 90 mm Hg or more, a systolic arterial blood pressure of 140 mm Hg or more, or a mean arterial blood pressure of 90 mm Hg or more. Hypoglycemia was defined as a serum blood glucose level of 45 mg/dL or less. Severity of hyponatremia was classified as mild (plasma sodium > 130 mmol/L), moderate (plasma sodium 125129 mmol/L), and severe (plasma sodium <125 mmol/L). Hypotonia was defined as a calculated serum osmolality of less than 280 mOsm/Kg of effective plasma osmolality, calculated by the formula Osm = [2 x serum sodium] + [glycemia/18] using the first values of serum sodium and glycemia after the patient's admission. Euvolemia was defined as the absence of hypervolemia manifestations (peripheral edema, jugular vein ingurgitation, ascites, pleural effusion) and absence of hypovolemia manifestations (dry mucose membranes, dry skin, collapsed jugular veins and BUN/Creatinine ratio more than 20) according to clinical record registries at admission. Data were analyzed using Microsoft Excel software.
RESULTS
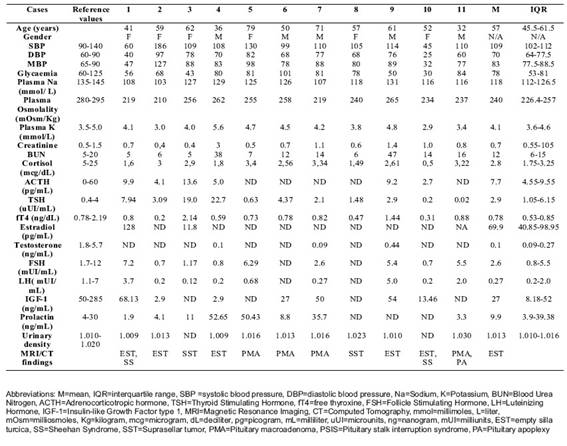
11 cases of hyponatremia due to secondary adrenal insufficiency were analyzed. 54.5% of the patients were women with a median age of 57 years (IQR 45.5-61.5 years). Table I shows the results of the diagnostic tests made to these patients. Cortisol measurements where taken between 8 and 9 am according to guideline recommendations except in 4 patients: case 1 before 8 am and cases 2, 5 and 7 after 9 am. In case 1, hemodynamic instability led to measurement outside the recommended time, whilst in the other 3 cases no reason was registered for the extemporaneous sampling.
In all cases hyponatremia was hypotonic and euvolemic with a median plasma sodium of 118 mmol/L (IQR 112-126.5 mmol/L). Hyponatremia was classified as severe in 6 cases, moderate in 4 cases and mild in 1 case. The median urinary density was 1.013 (IQR 1.010-1.016). All the patients had clinical characteristics of SIADH (euvolemic hypotonic hyponatremia with a urinary density above 1.003).
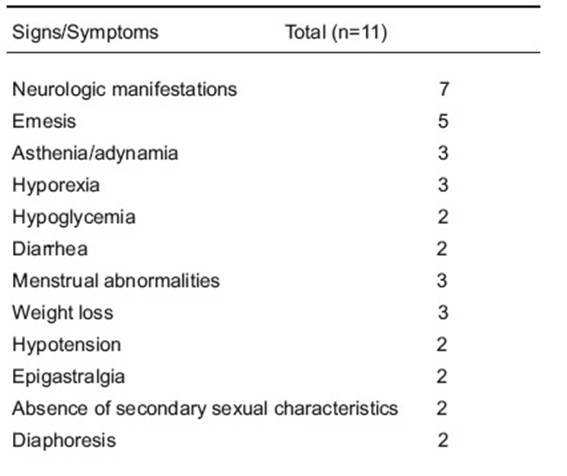
The main clinical manifestations were neurologic symptoms (disorientation, confusion, cognitive decline, and somnolence) in 63.6% of the cases followed by emesis in 45.5%. 2 cases had seizures as their initial manifestation (table II). Glucocorticoid deficiency manifestations were present in 2 cases as hypotension and another 2 cases as hypoglycemia, all of them with severe hyponatremia. Surprisingly 1 case had hyperkalemia that was explained in this case by acute kidney injury secondary to a worsening congenital obstructive uropathy.
All the patients had thyroid stimulating hormone (TSH), free thyroxine (FT4), and serum cortisol levels measured. Adrenocorticotropic hormone (ACTH) was measured in 63.6% of cases. The median cortisol concentration was 2.8 mcg/dL (IQR 1.75-3.25 mcg/dL) and the median ACTH concentration was 7.7 pg/nL (IQR 4.5-9.5 pg/nL). 54.5% of the cases had cortisol levels < 3 mcg/dL. In 4 cases without ACTH levels, the absence of other manifestations of adrenal insufficiency (hyperkalemia, hypotension, and hypoglycemia) that are more common in primary adrenal insufficiency, and the improvement in sodium levels with glucocorticoid replacement therapy, allowed the diagnosis of secondary adrenal insufficiency. No confirmatory test was made in these cases given the lack of synthetic ACTH for the stimulation test. Insulinic hypoglycemic test was deemed unsafe in two cases (cases 5 and 8) since they were over 70 years of age and deemed unnecessary in all cases since interruption of glucocorticoids for these tests was considered unsafe.
After the interpretation of thyroid function tests 5 cases were classified as having central hypothyroidism, 2 cases as subclinical hypothyroidism, 2 cases as primary hypothyroidism, and 2 cases as euthyroid. Gonadotropins were measured in 9 cases (FSH or LH) and 5 patients also had levels of free testosterone or estradiol. In 54.5% of this cases hypogonatropic hypogonadism was present. The most frequent finding in Magnetic Resonance Imaging (MRI) of sella turcica was empty sella syndrome (6 cases), followed by pituitary neoplasms (5 cases). 2 of the 6 women had empty sella syndrome with a history that suggested Sheehan syndrome as its etiology.
5 patients (cases 3, 4, 7, 8 and 10) of this series had an intercurrent conditions that lead to the manifestation of hyponatremia: 2 begin with symptoms after the start of thyroid hormone supplementation, 3 in the postoperative period of minor surgeries. Of these 5 patients only two had previous diagnosis of hypopituitarism (4 and 10) and failure to adjust dose previous to minor surgeries in both cases, without a clear reason for this, despite instructions from the endocrinologist of how to do it in the clinical record. The other 3 cases were diagnosed as new cases after the intercurrent condition appeared. Of the two patients that had initiation of thyroid hormone supplementation as a triggering factor, both results were initially misinterpreted by the general practitioner as primary hypothyroidism. All patients had compromise of 1 or more hypophyseal axis additional to hypophysis-adrenal axis. Hypogonadotropic hypogonadism and central hypothyroidism were the most common associated hypophyseal deficiencies.
DISCUSSION
Secondary adrenal insufficiency tend to be underdiagnosed as a cause of euvolemic hyponatremia when patients are admitted -(2,4,1416). A retrospective study in Germany of Diederich et al. found the prevalence of euvolemic hyponatremia due to secondary adrenal insufficiency around 20.1% (15). Other studies show that despite 3.8% of patients with euvolemic hyponatremia had evidence of adrenal insufficiency, only a small number of patients had cortisol levels measured (16). Only 21 to 40% of ER patients with hyponatremia are clinically evaluated to determine their volume status which led to appropriate diagnostic evaluation in 31% of the cases (2,4,5). Regardless of the knowledge that secondary adrenal insufficiency is a known etiology of euvolemic hyponatremia and its exclusion is required previous to the SIADH diagnosis, there is little literature about it -(14,15,2128).
In secondary adrenal insufficiency, hyponatremia presents in about 85-90% of the patients (17,18,20,27,29). The pathophysiology of hyponatremia in these cases is owed to the glucocorticoid deficiency that results in an increased hypothalamic secretion of CRH that stimulates ADH secretion leading to SIADH -(1315,22,24,27,29). At the same time the direct inhibitory effect of cortisol on ADH release is lost, contributing to hyponatremia onset -(14,1620). Although this hyponatremia is bioquimically and clinically similar to SIADH, it improves with glucorticoid replacement therapy -(14,1620). The chronic ACTH and glucocorticoid deficiency are responsible for the symptoms of secondary adrenal insufficiency which are unspecific and in 50% of the cases are present a year after diagnosis (14,17,18,20,29). This symptoms include nausea, emesis, abdominal pain and diarrhea or constipation (56-92%); anorexia and weight loss (73-100%); fatigue and malaise (95-100%) (14,17,18,20,29). Its presentation also depends on the hormonal deficit, whether is total or partial, given that partial ACTH deficiency only leads to symptoms during stress situations; while total ACTH and cortisol deficiency can cause severe symptoms as hypotension and shock (28).
Stressful situations such as infections, hypoglycemia, nausea, or emesis are known secretagogues ofADH. These factors when present can worsen hyponatremia and make it symptomatic -(14,15,18,20,24,2730).
Is more frequently reported in elderly patients and has been related with multiple risk factors associated with aging such as increased ADH release, diminished renal handling of sodium, lower sodium intake, and changes in water intake; being the enhanced release of ADH the most important factor (12,24). The case series reported by Diederich et al. and Cuesta et al. also show how secondary adrenal insufficiency is always accompanied by hypopituitarism, with no single case of isolated secondary adrenal insufficiency in neither of the studies, with empty sella being the most common cause of hypopituitarism in these patients and Sheehan's syndrome being the most common cause among women (15,16).
The findings of these case series where consistent about neurologic symptoms as the most common clinical manifestation, followed by emesis, and asthenia/adynamia (14,17,18,20,29). These reflects the similar behavior of secondary adrenal insufficiency between European and Latin-American patients, giving support to follow the same guidelines in the diagnostic process of hyponatremia that have been adapted from other latitudes in Latin-American countries.
The median age at presentation was 50 yo in men and 58 yo in women, in contrast to previous studies. The authors think this difference could be due to the lower median age of Colombian population in contrast to European countries where the published series was conducted (15,16).
An important finding was that only 2 patients had a previous diagnosis of secondary adrenal insufficiency before admission, with a similar rate of that reported by Diederich et al. in a case series of 28 patients (15).
Bearing in mind that at the present there are no local studies in Colombia about secondary adrenal insufficiency prevalence as a cause of hyponatremia, nor case reports of this entity, here is a report of 11 cases detected during the study of euvolemic hyponatremia in a tertiary care hospital during a period of 1.5 years. These should alert local and world medical community to remember the importance of measuring cortisol in a routinary fashion to patients with characteristics of SIADH despite the absence of other adrenal insufficiency findings (hypotension or hypoglycemia), given that a delay diagnosis could lead to deleterious consequences in patients' health and survival derived from a wrong approach and therapy since they do not answer to the conventional therapy and had a high frequency of alterations in other hormonal axis that also need replacement therapy. Is also important to draw attention about the need for education of physicians in thyroid hormone profile interpretation to avoid misdiagnosis of central hypothyroidism as primary hypothyroidism, given that inadequate initiation of thyroid hormone supplementation before knowing the hypophyseal adrenal axis function, could lead to adrenal crisis as was seen in two cases. Another unmet educational need for patients and physicians is the adjustment of glucocorticoid dose in perioperative period and during acute illnesses in patients with secondary adrenal insufficiency or a strong clinical suspicion.
The retrospective characteristic of this case series, along with lack of ACTH for all cases, lack of confirmatory test in these cases and extemporaneous measurement of cortisol in 4 of the 11 patients are the main limitations of this case series. Conclusions
Euvolemic hypotonic hyponatremia is the one of the syndromic presentations of secondary adrenal insufficiency, is often not accompanied with other manifestations of adrenal insufficiency but these patients do have symptoms and signs of involvement of another pituitary axis. This disease is clinical and biochemical indistinguishable from SIADH. A low threshold for suspicion, a thorough interrogation and physical examination looking for hypopituitarism signs and symptoms (absence or loss of secondary sexual characteristics, diminished libido, lack of morning erection in men, and secondary amenorrhea in women) in patients presenting with SIADH would expect to improve diagnosis with a serum morning cortisol measurement in these patients to avoid an inappropriate management. It's important to underscore the high prevalence of misinterpretation of thyroid hormone levels that lead to supplementation without prior hypophyseal-adrenal axis evaluation, and lack of adjustment of glucocorticoids during surgery and sickness in these patients, since addressing these unmet educational needs could improve outcomes and avoid increased costs derived from adrenal crisis that are preventable in such cases.
ACKNOWLEDGMENTS
The authors wish to thank E.S.E. Hospital Universitario de Pereira and Universidad Tecnológica de Pereira for the support during the development of this publication.
CONFLICT OF INTEREST:
Vallejo-Gonzalez, S have worked as speaker for Novonordisk, AstraZeneca, Medtronic and Boehringer Inghelheim and Forero-Gómez, JE have worked as clinical investigator for Pfizer and received financial support from Novonordisk. None of the authors perceive any grants or financial support for this paper and there is no conflict of interest that could be perceived as prejudicing the impartiality of this research.

