











 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkINTRODUCTION
The Covid-19 pandemic presented approximately 10 874 146 million cases and around 521 355 deaths on a worldwide level.3
In Ecuador, the rate was 147 033 cases confirmed by RT-PCR (reverse transcription-polymerase chain reaction), with more than 10 800 deaths.4
The city of Guayaquil was one of the most af fected areas, with the largest number of confirmed cases (17 973); whereas in the Manabí province, 10 151 cases confirmed with swab PCR tests have been reported up to now.5
The Intensive Care Units around the country collapsed during the first four weeks. There was a group of patients who couldn’t have access to a ventilator. The mortality rate was 7%.
The Hospital de Especialidades Portoviejo re ceived during the first 6 months more than 12 000 cases of suspected Covid-19 based on clinical and epidemiological criteria and chest imaging, with 491 deaths from SARS-CoV-2; and the highest mortality rate occurred in the Intensive Care Unit (48.8%) (Table 1).
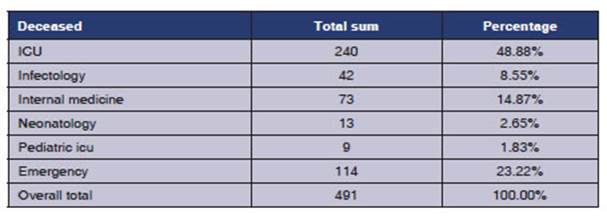
Table 1 Number of deaths from March to September, 2020, due to Covid-19 at the Hospital de Especialidades Portoviejo
In view of the severity of this disease, the Pulmonology and Infectology Service of the Hos pital de Especialidades Portoviejo, based on poor pharmacological and therapeutic evidence about the Covid-19 pandemic, created a protocol for the compassionate use of medication with ruxolitinib. It was used in SARS-CoV-2 cases with increased in flammatory markers (Ldh [lactate dehydrogenase], ferritin, D-dimer, IL6) and those with more than 50% of radiologic involvement in chest images, at the IIB stage of the disease with hypoxemia. The hypothesis included the fact that the use of rux olitinib could provide a benefit, because it reduces the cytokine levels, and so it could reduce the number of patients admitted to the Critical Care Units with moderate and severe acute respiratory distress syndrome; this would cause radiological improvement and faster lymphocyte recovery.6
Secondary hemophagocytic lymphohistiocy tosis (sHLH) is a hyperinflammatory syndrome secondary to several triggers, including sepsis, characterized by strong increase in cytokines with multi-organ failure and a very high mortality rate.7
Ruxolitinib reduces the spleen volume and circulating levels of proinflammatory interleu kins, particularly IL-6 and TNF-alpha.8 Recently, preliminary data from 7 patients with sHLH who were treated with ruxolitinib 15 mg (twice a day) showed promising results regarding global sur vival, and improvement has been observed in the inflammatory markers such as ferritin and soluble IL-2 receptor.9
MATERIALS AND METHODS
Patients were studied from April 2020 to June 2020 at the Hospital de Especialidades Portoviejo.
Inclusion criteria
Patients who met the following criteria:
• High suspicion and diagnosis of Covid-19.
• Chest X-ray and tomographies showing more than 50% of radiologic involvement.
• PaFi ≤ 250 mmHg.
• Rapidly worsening respiratory failure requiring invasive ventilation.
• Increase in any of the systemic inflammatory response in dicators: LDH 300 U/L, ferritin 1000 ng/mL, D-dimer 1500 ng/mL.
• SpO2 ≤ 93%.
Exclusion criteria
• Patients diagnosed with Covid-19 plus chronic renal failure with clearance of less than 30 mL/h.
• Infectious diseases, such as tuberculosis, HIV.
• Hypersensitivity to the active principle.
• Pregnant women.
• Patients who weigh less than 50 kg.
• Platelets <50,000 cells/mmc.
• Hemoglobin < 8 g/dL.
• Neutrophils < 500 cells/mmc.
• Sepsis documented by pathogens other than SARS-CoV2.
• Patients who didn’t sign consent to the use of ruxolitinib.
DATA ANALYSIS
In the analysis of the information gathered from the medi cal records of Covid patients, we applied the quantitative paradigm through the use of descriptive statistics and the creation of contingency tables, absolute and relative frequencies, and the calculation of mean values, standard deviation and minimum and maximum values. Inferential statistics is also applied to support the research hypothesis through student-t techniques for independent samples and chi square test, as applicable, depending on the type of variable. For data processing we used the program Excel for windows and the statistical program SPSS, version 21.
Treatment as compassionate use
Patients were randomly selected; 1:1 ratio. They were divided in two groups, 50 patients each, with a total of 100 patients diagnosed with Covid-19 through PCR: group 1 received 250 mg chloroquine phosphate every 12 h, for 7 days; group 2 received 5 mg ruxolitinib, twice a day, for 10 days. Also, systemic corticoids were used during 3 days, plus general measures (Figure 1).
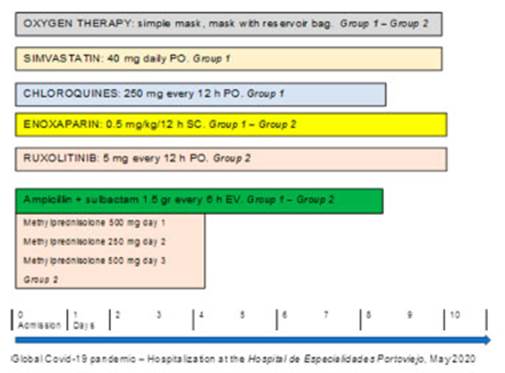
We performed daily electrocardiogram control and sus pended medication in patients with prolonged QT interval ≥ 500 ms.
RESULTS
This study intends to compare the use of two types of treatment in patients admitted to the Hospital Especialidades Portoviejo, Ecuador, an institution in the province of Manabí with the sentinel sur veillance system for cases of SARS-CoV-2. Group 1 includes patients who receive chloroquine + azithromycin; and in group 2 patients receive ruxolitinib + methylprednisolone.
Table 2 shows the clinical aspects of the cases according to the treatment group. One of the variables is “age”, where patients aged 60 or older predominate in both groups (62% in group 1 and 58% in group 2). Mean age was 60.9 ± 10.7 years and 62.2 ± 12.7 years, respectively.
Regarding sex, males predominate in group 1 (62%), and account for 50% in group 2.
The degree of severity that is most frequently presented is “severe” (70.0% in group 1 and 78.0% in group 2). With regard to comorbidities, the presence of an underlying disease (40% in group 1 vs. 34% in group 2), or two or more associated diseases (22% in both groups) predominate in both groups. The most frequently found conditions were: hypertension (22% vs. 16%), hypertension and diabetes (12% vs. 14%), and diabetes (8% vs. 2%), group 1 vs. group 2, respectively.
Table 3 shows some of the clinical parameters used for the Covid diagnosis protocol. SaO2 was measured upon admission, and similar mean val ues were observed in both groups (82.94 ± 12.2 in group 1, and 84.12 ± 8.6 in group 2). Also, upon admission, we carried out chest X-ray or lung tomography in patients who were able to move in order to observe the percentage of involvement of the pulmonary parenchyma, and found 51.55 ± 11.9 in group 1, and 54.4 ± 12.7 in group 2. Then, 72% of the patients underwent a control chest X-ray, and a lower percentage of involvement was found in patients treated with ruxolitinib + methylprednisolone (79.1 ± 30.3 in group 2). An assay conducted in China showed significant improvement in the chest computed tomographies of 43 patients who received ruxolitinib.10
In order to show the differences between the groups regarding the percentages of lung involve ment through imaging, we applied the student-t for independent samples. The results showed that there weren’t any statistical differences between the groups in relation to the percentage of lung involvement (p > 0.05; at 95% CI).
Adverse effects
Group 1: chloroquines + azithromycin: 4 out of 50 patients had prolonged QT interval, so treatment with chloroquines was suspended. Those patients, who were older than 70 years, died on days 7, 8 and 10 of hospitalization. On day 4 of hospitalization, another patient showed lower gastrointestinal bleeding; it is worth mentioning that the patient had arterial hypertension, diabetes mellitus and nephrectomy due to clear cell cancer. Four patients had sudden death on days 6 and 7 of hospitaliza tion.
Group 2: ruxolitinib + methylprednisolone: 1 out of 50 patients died on day 5 due to a stroke. The other symptoms presented by 4 patients were mild, such as cephalea, insomnia and nervousness on days 1 to 3 of hospitalization; we couldn’t de termine if those symptoms were characteristic of the ongoing disease.
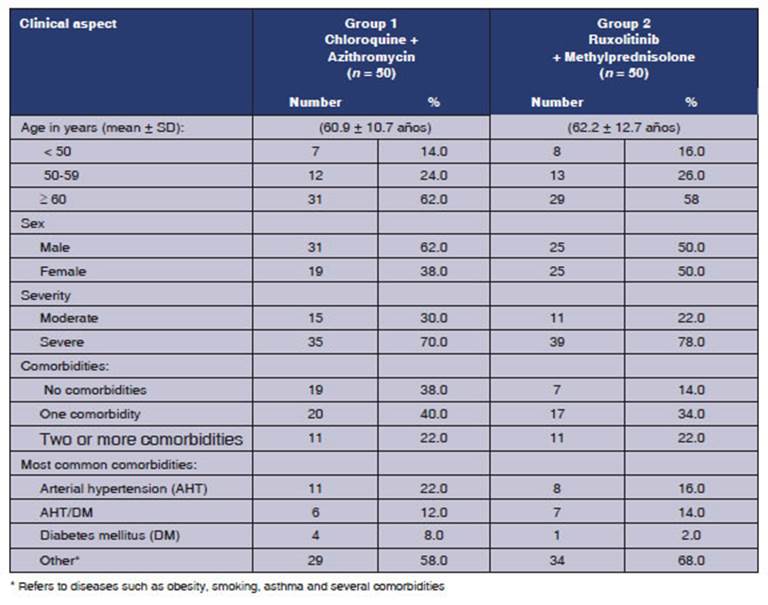
Table 2 Clinical aspects according to the treatment group. Cases of covid-19. Hospital de especialidades portoviejo. Period: May, year 2020
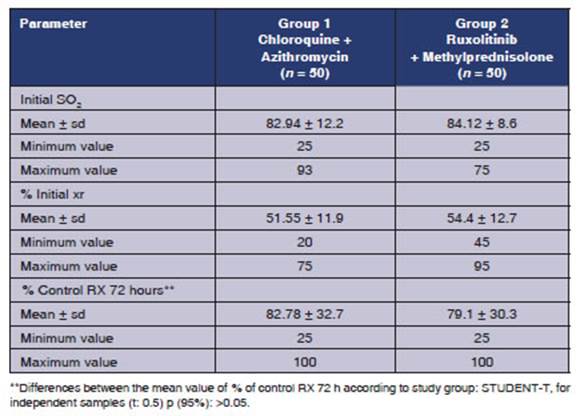
Table 3 Clinical parameters according to the treatment group. Cases of COVID-19. Hospital de especialidades portoviejo. Period: May, year 2020
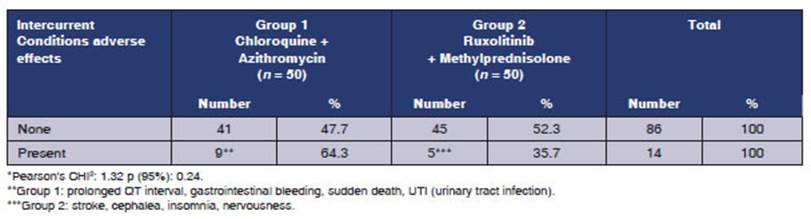
Table 4 Adverse effects and intercurrent conditions according to the treatment group*. Cases of COVID-19. Hospital de especialidades portoviejo. Period: May, year 2020
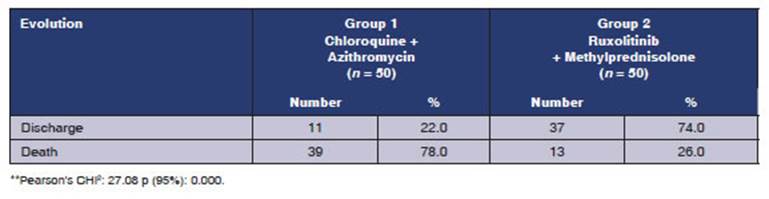
Table 5 Evolución de la enfermedad según grupo de tratamiento*. Casos COVID-19, hospital de especialidades portoviejo. Período: mayo, año 2020
The stroke could have been a matter of causal ity, considering the hypercoagulability syndrome of Covid-19. The bibliography describes venous thrombosis in patients diagnosed with Sars- CoV-211, of 5%-15% in patients outside the ICU, and up to 35% in patients inside the ICU.
Table 4 compares the adverse effects found in patients treated with chloroquine + azithromy cin (group 1) vs. those treated with ruxolitinib + methylprednisone (group 2). A higher number of adverse effects and intercurrent conditions was observed in group 1 (64.3%) compared to group 2 (35.7%). Some of the adverse effects are: prolonged QT interval, gastrointestinal bleeding, sudden death, UTI (group 1), and stroke, insomnia, nervousness (group 2). However, the research hy pothesis about the differences between the groups according to the treatment couldn’t be supported when applying the chi square, obtaining a p value > 0.05, 95% CI.
Likewise, there are new lines of research that would show with greater certainty the adverse ef fects that could be caused by the compassionate use of these treatments for this reemerging disease and its different variants.
It is necessary to mention there was a limita tion upon this research, since we couldn’t ask for the autopsy, given the measures imposed by the Ministry of Public Health for the management of corpses of patients diagnosed with Covid-19. Thus, it wasn’t possible to determine the real cause of death of these patients, whose treatment (with its adverse effects and complications) is showing effectivity up to this day, and is being evaluated by specialists around the world.
The number of patients referred to the Inten sive Care Unit was higher in group 1: 30 patients. Only one of those patients was discharged (3.3%), whereas 14 patients from group 2 were referred to the ICU, and 4 of them recovered (28.5%).
CONCLUSION
We can’t attribute the decrease in mortality and ICU admissions to the group using ruxolitinib, since patients from this group received systemic corticosteroids; but, the increase in the number of patients being discharged and the lower number of adverse effects found in group 2 (ruxolitinib + methylprednisolone) are surprising. A significant increase in mortality was seen with the use of chloroquines and azithromycin.
This case report invites health professionals to conduct studies with more statistical weight to evaluate drugs that inhibit the cytokine storm induced by Covid-19.

