











 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkINTRODUCTION
Caries prevalence today is still high in many populations1. Due to the negative impact on patients' lives associated to more severe stages of the disease,2 efforts have focused on developing more effective treatments associated to preventive measures3. As a result, the World Health Organization (WHO) has recommended Atraumatic
Restorative Treatment (ART) as part of the Basic Package of Oral Care (BPOC)3.
Glass Ionomer Cements (GIC) have been proposed as the material of choice for ART. Although GIC longevity is similar to that of other restorative materials in primary teeth4, it still poses a challenge for the survival of occlusal-proximal restorations. In this regard, the use of protocols to improve substrate-material adhesion may enhance the longevity of restorations. However, there is still no consensus regarding which substrate pre-treatment protocol is best when using GIC.
The GIC bonding mechanism can be explained as an ionic interaction with bipolar electrostatic forces between the cement and the dental structure, with an important role of the initial wetting, promoted by the carboxylic free radicals, for effective adhesion5. Knowing that this adhesion is more critical in dentine than in enamel, several authors have assessed methods to improve it6-11, understanding that the frequently used technique of leaving a "smear layer" on the cavity walls in the carious tissue removal process may help. Two of the main discussion points are whether or not the smear layer should be removed and which is the best pre-treatment alternative6-11. Previous studies have used different products for surface pre-treatment, ranging from different polyacrylic acid concentrations to phosphoric acid, which has a conditioning/cleaning effect. However, it has been suggested that in addition to removing the smear layer, strong acids used as pre-treatment agents could also cause enamel and dentine decalcification, considerably reducing the amount of calcium available for adequate adhesion, leading to a decrease in bond strength9. Regarding the use of polyacrylic acid, the literature has shown some advantages in relation to GIC properties1011. Other studies have shown that some products do not interfere in adhesion quality or even that mechanical cleaning procedures only may be enough6.
Thus, there is a lack of evidence regarding the influence of pre-treatment on the materials' bond strength to dental substrates, especially those submitted to cariogenic challenges, which are clinically relevant because they are commonly found during restorative procedures in the current scenario of minimal intervention.
Thus, the aim of this in vitro study was to assess the influence of different pre-treatment approaches on GIC bond strength to both sound and carious dentine. The hypothesis is that there is no difference in bond strength values according to the pretreatment of dentine.
MATERIALS AND METHODS
Study design and ethics
This in vitro study received ethical and legal approval from the Santa Cecilia University Ethics Committee (Protocol #04/2016). Experiments were conducted following the Ethical Principles on Animal Experimentation, adopted by the Brazilian Laboratory Animal Science Association (COBEA) and certified by the Use of Animals Ethics Committee of the Cruzeiro do Sul University according to Law 11.794/2008.
Teeth were randomly assigned to six experimental groups according to substrate - sound or caries-affected dentine; and substrate pre-treatment approach - no conditioning (control), polyacrylic acid for 10 s or phosphoric acid for 7 s.
Sample selection
The sample consisted of 60 bovine teeth (n=10), according to a previous study of GIC bond strength to bovine dentine12. Inclusion criteria were the absence of structural defects and/or cracks and fractures. Teeth were cleaned with pumice slurry and stored in chloramine solution T 0.5% at 4 °C for 30 days, with the solution being changed weekly.
Tooth preparation
Roots were removed with diamond discs in a cutting machine (Labcut 1010, Extec Co, Enfield, USA) and crowns were embedded in PVC tubes with chemically activated acrylic resin, (JET Classico®, Sao Paulo, SP, Brazil).
The dentine surface was abraded with silicon carbide water sandpaper #180 for 60 sec to obtain a flat surface, and then with #600 for 60 sec to standardise the smear layer.
Cariogenic Challenge
Caries-affected dentine specimens were submitted to a pH-cycling cariogenic challenge as follows: 14 immersion cycles (8 hours) in a demineralising solution (2.2 mM CaCl2, 2.2 mM NaH2PO4, 0.05M acetic acid, pH adjusted at 4.5 with 1M KOH); and then, immersion (16 hours) in a remineralising solution (1.5 mM CaCl2, 0.9 mM NaH2PO4, 0.15 mM KCL, pH =7.0), at room temperature without shaking13.
Restorative procedures
Pre-treatment substrate approaches were performed following manufacturers' recommendations according to allocation group. After surface treatments, three polyethylene tubes 1.0 mm tall and 0.76 mm in diameter (micro-bore® Tygon S-54-HL Medical Tubing, Saint-Gobain Performance Plastics, Akron, OH) were placed on the exposed surfaces. Tubes were filled, with an encapsulated GIC (Riva Self Cure, SDI, Victoria, Australia) inserted with an applicator. A thin petroleum jelly layer was applied over the material to prevent both water absorption and loss.
Specimens were stored in distilled water at 37°C for 24 h. After this time, tubes were removed using a #15 blade. All samples were analysed under 10x microscope, excluding those presenting bubbles, interface failures and other defects. All specimens were prepared by a single trained operator at room temperature (24 °C).
Microshear test
After 24h storage, an external examiner, blinded to the experimental groups, fixed the specimens to a device, previously adapted to a testing machine (Kratos, Kratos Dinamómetros, Brazil). Thin wires (0.20 mm) were used to make a loop around the load cell projection and the GIC cylinder, maintaining the contact with the dentine surface as close as possible to the bonding interface. A shear force (0.5 mm/min crosshead speed) was applied until failure occurred.
Maximum load values supported by the dentine/ material bond were expressed in Newtons (N) and later converted to megapascals (MPa), considering the inner diameter area of the polyethylene tube used as matrix.
Failure Mode
After testing, the specimens were assessed under stereomicroscope at 400x magnification (HMV II,
Shimadzu, Kyoto, Japan) to establish the failure mode. Failures were classified as adhesive (failure in the substrate/material interface), cohesive in the dentine or the GIC (failure in the substrate or the material), and mixed (combination between adhesive and cohesive, with any type of cohesive failure of up to 25% on the interface).
Statistical Analysis
The experimental unit was the tooth. Bond Strength values (BS) in MPa were initially assessed for normality distribution and variances homogeneity using Kolmogorov-Smirnov and Levene's tests, respectively. To analyse whether the substrate pretreatment approaches influence the BS, two-way analysis of variance - pre-treatment and substrate condition - was conducted. Chi-square was used to compare premature failures among groups. Descriptive analyses of the failure modes in relation to experimental groups were also performed. A significance level of 5% was adopted for all analyses. SPSS V16 for Windows (SPSS Inc., Chicago, IL, USA) was used.
RESULTS
Microshear bond strength
Table 1 shows the results, including BS means and standard deviations, for the experimental groups in sound and caries-affected dentine.
ANOVA showed statistically significant differences between the main factors *pre-treatment* (p<0.001) and *substrate condition* (p=0.025). However, interaction among factors did not show any differences (p=0.058). GIC had better bond performance in sound dentine than caries-affected dentine. In addition, pre-treatment with phosphoric acid resulted in lower BS values when compared to both polyacrylic acid and control groups. Polyacrylic acid application led to similar BS values to those in the control group.
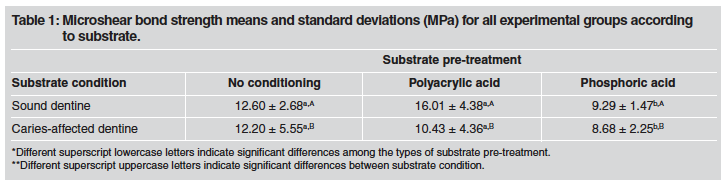
Table 1 Microshear bond strength means and standard deviations (MPa) for all experimental groups according
*Different superscript lowercase letters indicate significant differences among the types of substrate pre-treatment. **Different superscript uppercase letters indicate significant differences between substrate condition.
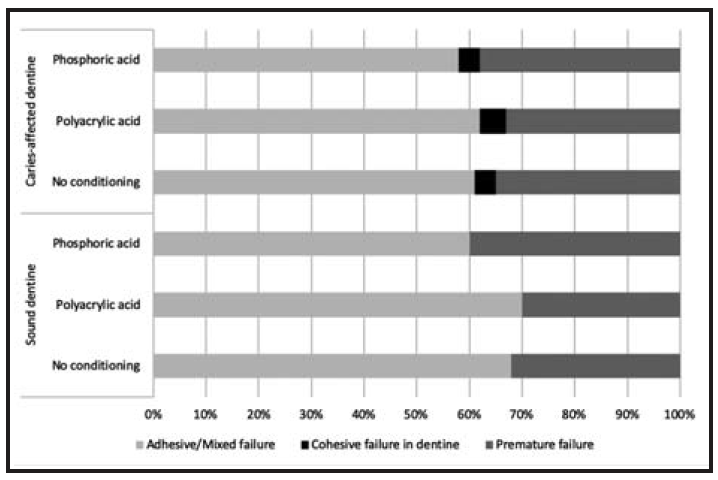
Fig. 1 presents the failure pattern distribution in the experimental groups. In general, there was predominance of adhesive and mixed failures. Cohesive failures in the substrate were only seen, though less frequently, in caries-affected dentine. Table 2 shows the distribution of premature failures in the experimental groups. Regardless of substrate, there was no statically significant difference among groups.

DISCUSSION
The field of dental materials still lacks evidence of the influence of pre-treatment approaches on GIC bonding to dental substrates. Clinically, substrates subjected to cariogenic challenges are the most relevant because they are commonly found during restorative procedures in the current scenario of minimal intervention.
In this study, the application of polyacrylic acid led to BS values similar to those in the control group, regardless of the substrate, corroborating previous studies that showed no benefit of surface pretreatment with 10-25 % polyacrylic acid in terms of GIC bond strength to the dentine14-16. However, other reports refute such findings by showing several advantages of polyacrylic acid pretreatment for enhancing GIC properties10,11.
GIC chemical bonding to dental substrates has been recognised as one of the main characteristics of these materials5-7. However, the effective validity of these bonds is still poorly understood, with only some explanatory theories. Bond strength is basically influenced by two factors: substrate composition and surface pre-treatment (conditioning). The presence of contaminating agents may alter the surface energy and therefore the material wettability to the dental surface17. Thus, the smear layer interferes with the GIC bonding to the dental structures,18 which is why pre-treatment is advocated7,19,20. Still, this theory was not confirmed by the present study.
Pre-treatment with phosphoric acid resulted in lower BS values than those in the polyacrylic acid group and even those in the control group. This could be explained by the excessive demineralisation and consequent lack of minerals, which are essential for the GIC chemical bonding. Results from this study complement those found by Kokmaz et al.20, who did not observe better GIC bonding to either enamel or dentine after the application of phosphoric acid.
These findings may be explained by the GIC bond mechanism itself, which is mainly produced by ionic exchange with calcium free radicals. Thus, strong acids such as citric or phosphoric acid, in addition to removing the smear layer, (rich in calcium radicals and capable of forming a bonding bridge between the cement and the dentinal walls), also act as enamel and dentine decalcifying agents, greatly reducing the amount of available calcium required for adequate bonding7,17.
As has also been observed in previous studies, the GIC that we used had better adhesive performance on sound dentine21-23. It has been hypothesised that differences in chemical compositions and morphology may be responsible for the poorer restorative materials performance, especially GIC, which, as mentioned above, needs calcium bonds to the substrate to support the chemical reaction.
It should be highlighted that the caries-affected dentine in this study was artificially developed. This method for developing carious lesions produces dentinal lesions resembling natural ones13. It has proven to be effective, especially for BS tests, and has been suggested for use because it allows a greater area of exposed dentine than other methods of artificial carious lesion development13. Additionally, other factors, such as operator variability, may affect mechanical tests results. Indeed, Adebayo et al.24 observed that as the operator gained experience, there was a gradual increase in mean values and decrease in standard deviations and variation coefficient from tests results. This reflects the importance of training in the methodology used. The present study found a high number of premature failures, possibly as a result of the stress applied to the specimens, which may have caused a fracture when the polyethylene tubes were removed before microshear testing, as previously suggested by Tedesco et al.,25 who verified a clear trend to premature failures as a result of removing polyethylene and/or starch tubes.
To conclude, dentine pre-treatment showed no benefit for the GIC bond to either sound or affected dentine. However, this study was conducted using a single GIC brand, and the results cannot be extrapolated to other GIC brands. Studies assessing the bond stability of GIC when submitted or not to pre-treatment approaches are needed to contribute to the evidence to support the best protocol for restorations with Glass Ionomer Cements, which are effective, cheaper, less time-consuming materials.

