











 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkINTRODUCTION
Bonded ceramics have become the standard of care for esthetic restoration in current dentistry. According to numerous clinical studies, their advantages include excellent clinical performance, high rates of survival, near to ideal optical appearance, good biocompatibility, low thermal conductivity, chemical stability and surface smoothness 1 , 2 .
Glass matrix and polycrystalline ceramics are the two families, according to their structure and composition, which can be used to fabricate metalfree restorations. Glass matrix ceramics (GMCs) are preferred when the main goals are esthetic results and stable micro-mechanical and chemical adhesive interaction with composite resin luting materials 3-6 . Among GMCs lithium disilicate (LDS) based ceramics have gained popularity recently, due mainly to their versatility, with an indication range that goes from veneers to three-piece bridges in premolar areas and implant-supported single crowns 7 , 8 . LDS restorations can be made either by traditional heat-pressing procedure or through a digital workflow and milling process (CAD-CAM). There are key differences in crystal distribution, shape and size between pressed and CAD-CAM restorations, all of which are prone to affect the transmittance of the structure 8 , 9 .
One of the most important factors related to clinical success of glass ceramics is the achievement of durable bonding between dental tissues and the restorative unit through a composite-based luting material (CBLM) of adequate mechanical properties 10 . To ensure effective adhesive interaction, not only surface treatments of both substrates, but also an adequate activation of the polymerization in the composite organic matrix, are key factors 1 , 11-13 . Adequate activation is relevant for both light-cured and dual-cured materials. Although dual-cured materials were developed in an attempt to ensure activation in regions difficult to reach by light, they present significantly lower degrees of conversion when not properly photoactivated 1 , 14-17 .
Several variables have been reported to affect the quality of CBLM polymerization, including specific luting material composition, adhesivecement negative interaction, and transmitted light attenuation due to scattering and absorption as light passes through the restoration 14 , 18 , 19 . The amount of radiant energy that is lost whilst being transmitted through a ceramic restoration” depends on ceramic composition, structure, quality and quantity of the crystalline phase, thickness, shade and porosity, among other factors 14 , 17 . This reduction results in less energy being absorbed by the initiator system of the luting composite and thus, a lower degree of conversion and lower mechanical and chemical properties, biological compatibility and bond strength 8 .
Light transmittance for successful activation of composite luting materials depends not only on the characteristics of the restorative materials, but also the quality of the irradiated light. Hence, the transmittance in the 360-540 nm range should be considered, rather than the one occurring in the whole visible spectrum, which is more related to the concept of translucency as an optical property. Brodbelt 20 found that dental ceramics transmit two hundred times more light when scattering is taken into account (total transmission) and that transmittance also increases with higher wavelengths, as stated by Rayleigh’s law. Transmittance of blue light would thus be overestimated if total spectrum transmission is considered. Lieberman et al. 2 found that different ceramics transmitted higher rates of visible light than light in the blue spectra. This difference in transmittance may also be of interest when considering the different emission spectra of the curing units (CU) available. One study found that transmittance was significantly lower for CU emitting in the violet range than for others which spectrum was in the blue area 1 . The emission spectra vary among different CU, for instance, typical halogen units have broad range of emission spectra, from about 390 nm to 500 nm, while LED curing units, depending on their generation, may have different spectra of 440-500nm, 420-475 nm, or 390-415 nm and 430-490 nm in bimodal emission units 21-23 .
The aim of this study was to assess the transmittance of a lithium disilicate ceramic of different opacities and thicknesses with different curing units.
MATERIAL AND METHODS
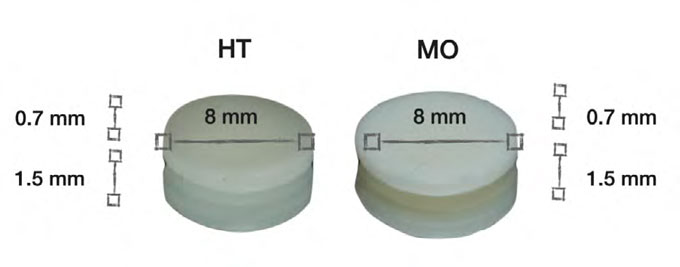
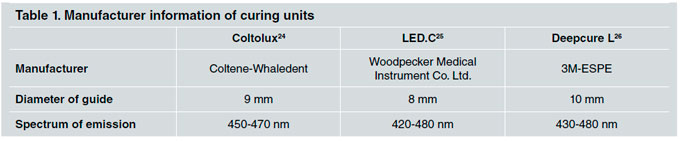
Disc-shaped specimens 8 mm in diameter and 1.5 mm or 0.7mm thick were designed with Zbrush® and Cura 3D® (Ultimaker) software, milled from high translucency (HT) and medium opacity (MO) IPS e-maxCAD blocks (Ivoclar Vivadent), (Fig. 1) with Ceramill Mikro 4 (Amann Girrbach, Austria) and processed according to manufacturer instructions. Thickness was verified in each case with a Mitutoyo (Mexico) caliper. Four different groups (n=4) were formed: G1(HT/1.5mm), G2(MO/1.5 mm), G3(HT/0.7 mm) and G4(MO/0.7 mm). Three curing units with fully charged battery throughout the procedure were used: Coltolux (Coltene- Whaledent)24, LED.C (Woodpecker Medical Instrument Co.Ltd)25 and Deepcure L (3M-ESPE)26 (Table 1). After installing an opaque 8mm diameter ad hoc sample holder, the reading of an halogen and led radiometer (Woodpecker® LM-1-Guilin Woodpecker Medical Instrument Co.Ltd) was registered with each curing unit guide placed in the sample holder directly on the reading window (SL - source luminance) and after interposing each of the specimens (CL - ceramic luminance). Absolute values were registered and transmittance (T) was determined in each case as the ratio between the first and second reading T= CL/SL. Data was analyzed with repeated measures ANOVA and Tukey test for multiple comparisons
RESULTS
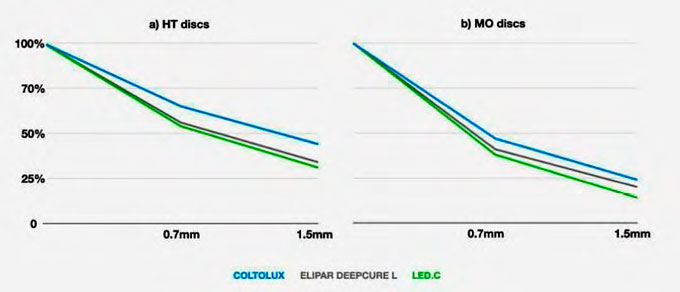
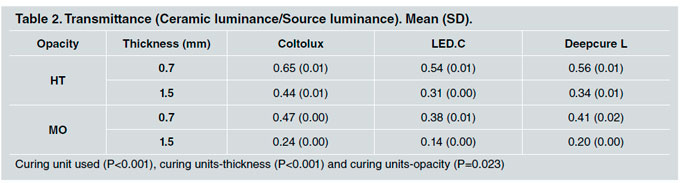
Under all the study conditions, the interposing of the specimens caused a statistically significant decrease in irradiance from 35% to 86% (Fig. 2), resulting in transmittance values of 0.65 to 0.14, which were related to the curing unit used (P<0.001) and to the interactions between curing units and thickness (P<0.001), as well as between curing units and opacity (P=0.023). CU source luminance values were 1275 mW/cm2, 1600 mW/cm2 and 1500 mW/ cm2 for Coltolux (Coltene-Whaledent), LED.C, (Woodpecker Medical Instrument Co.Ltd), and Deepcure L(3M-ESPE), respectively. Significant differences were also found among the three CUs studied regarding the behavior of the samples of different thicknesses and opacities (Table 2) .
DISCUSSION
Adhesive cementation is one of the key factors related to clinical survival and success of bonded glass ceramic restorations, as any flaw in the interface between the substrates may lead to early failure due to fracture, secondary caries, postoperative sensitivity, pigmentation and marginal leakage 1 . Another important aspect related to longevity is the CBLM elastic modulus, since due to the brittleness of ceramics, tensile stress is more likely to cause catastrophic failure than compressive stress, and lower values of elastic modulus in the underlying structures result in increased tensile stress 27 . Resinbased luting materials, whether photo-activated or dual-cure, require that enough energy is absorbed by the initiator system to reach an adequate degree of conversion, providing suitable physical, mechanical and biological properties. For that to happen, sufficient energy must be transmitted through the ceramic restorative structure 11 , 28 .
Different authors found that thickness and ceramic type were related to transmittance 28-31 . Zhang et al. found that 37%, 14% and 9% of the irradiating energy was transmitted through 1 mm, 2 mm and 3 mm, respectively, of a lithium disilicate ceramic 31 . Furthermore, Lópes et al. 28 reported transmission of 20% of total irradiated energy through 1.5 mm of the same material, which is consistent with the findings in the current study.
Evidence has been found that transmittance of ceramic is also dependent on the wavelength of the incident light, therefore, under equal conditions, ceramics transmit a higher fraction of energy in the 400-700 nm range than in the 380-540 nm range 2 . Hardy also reported that the use of a curing unit emitting light at 390-419 nm resulted in a lower fraction transmitted than a CU emitting 430- 510 nm, in a zirconia-based material 1 . This may explain the effect of the curing unit factor found in the current study, where the higher the range emitted by the CU, the higher the fraction of energy transmitted [Coltolux - 450-470 nm, followed by Elipar Deepcure L (3M-ESPE 430-480 nm), and subsequently by LED C Woodpecker Guilin (420- 480 nm)]. Although the differences in emitting spectrum may seem small, they are related to significative differences in the amount of energy transmitted. O’Keefe found similar results with Vita B2 felspathic porcelain veneers, which had different transmittance at 460, 470 and 480 nm30. Della Bonna et al. reported spectral behavior showing a slight linear increase in transmittance as wave length increased in most ceramics up to 550nm, beyond which the function is material-dependent 29 .
Hence, when luting an indirect ceramic restoration, successful polymerization activation is potentially compromised by two relevant factors: the wavelength of the light and the amount of energy effectively transmitted 1 , 2 , 20 . Regarding the latter, reductions ranging from nearly 40% to 86% of total irradiance should be expected. This could be addressed by employing a CU with higher irradiance to deliver sufficient energy, or by increasing curing time in order to maintain the energy dose. However, Bueno et al. found that for some luting materials, increasing curing time does not effectively compensate light attenuation due to the presence of an indirect restoration, so it should be considered material-dependent 13 . This could be explained by the transmitted light spectra, since the shorter the wave length, the less the transmission, so the effect should be more detrimental to CBLMs that include initiators such as PPD, TPO or Ivocerin® with absorbance peaks in the range of 350-400 nm, than to materials with camphorquinone 32 .
The roughening of the inner surface of the restoration as result of acid etching, and the increase of reflection due to finishing procedures, polishing or glazing of the outer surface, could be interesting factors to add to the equation of light transmittance in dental ceramics because additional scattering and reflection, respectively, could enhance the loss of transmitted energy.
Transmission efficiency affects the degree of conversion of composite-based luting materials and has direct consequence on longevity and clinical success. Moreover, the CU plays an important part in this process, mainly through its emission spectrum range. Therefore, when planning the adhesive procedures for bonded ceramics, the following factors are important and should be considered: type, composition, thickness, color and translucency of the ceramic system; spectrum of emission and irradiance of the curing unit and, according to Hardy et al., the monomer fraction, the presence of TEGDMA in the resin matrix, and the initiator system of the luting material 1 .

