










Servicios Personalizados
Revista

Articulo
 texto en
texto en  Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO
Links relacionados
-
 Similares en
SciELO
Similares en
SciELO
Compartir

 Permalink
PermalinkRevista argentina de cirugía
versión impresa ISSN 2250-639Xversión On-line ISSN 2250-639X
Rev. argent. cir. vol.113 no.2 Cap. Fed. jun. 2021
http://dx.doi.org/10.25132/raac.v113.n2.1539.ei
Articles
Totally implantable venous access device fracture due to pinch-off syndrome
1 Equipo de Cirugía Vascular Unidad de Cardiología Intervencionista y Terapéutica Clínica Bazterrica. Buenos Aires. Argentina
Totally implantable venous access ports with a subcutaneous reservoir constitute permanent venous access for cancer patients requiring safe administration of systemic chemotherapy over a long period. These devices consist of a silicone or polyurethane catheter, attached to a reservoir or port made of titanium or polysulphone; the catheter can be inserted by surgical dissection of the cephalic vein or by puncture of the subclavian or internal jugular vein. Catheter fracture and migration is a rare, yet potentially serious complication described in the bibliography1-3 with increased risk of arrhythmias, pulmonary embolism, endocarditis, cardiac perforation and sudden cardiac death3,4.
We report the case of a 57-year-old obese woman with right breast cancer and metastasis in the central nervous system who underwent percutaneous implantation of an 8 Fr. Groshong catheter valve connected to a reservoir made of titanium (Bard Access Systems®) through the subclavian vein under ultrasound and radioscopy guidance for the administration of systemic chemotherapy. The patient received several cycles of chemotherapy without complications, but 5 months after implantation presented progressive malfunctioning of the catheter, with intermittent inability to administer fluids through the catheter that initially improved upon changing the position of the ipsilateral arm. A chest X-ray showed a complete fracture of the catheter at the level of the costoclavicular space with migration of a distal fragment of the catheter to the right cardiac chambers (Fig. 1). The patient reported few episodes of palpitations. The fractured catheter was percutaneously removed via the right femoral vein using nitinol gooseneck snare (Amplaz Goose Neck®) without complications (Fig. 2).
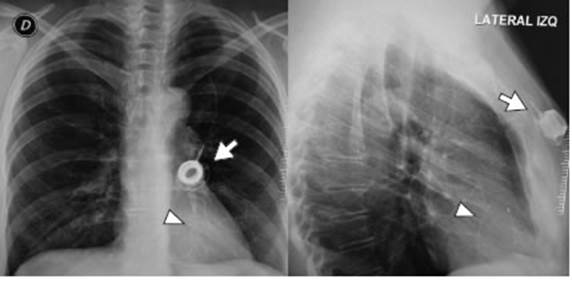
Figure 1 Posterioranterior and lateral chest x-ray showing complete fracture of the catheter (arrow) at the level of the costoclavi cular space with migration of a distal fragment of the catheter to the right cardiac chambers (arrowhead).
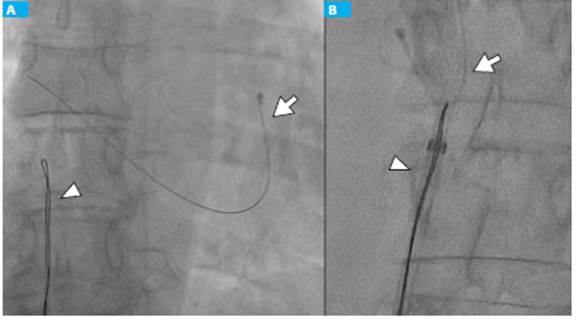
Figure 2 A. Fractured part of the catheter in the right cardiac chambers (arrow). B. Endovascular removal of the catheter using nitinol gooseneck snare (arrowhead).
Fracture of totally implantable venous access devices is a rare complication. Chang et al.1 analyzed 3953 cases and reported an incidence of 0.86%.
Wu et al. 5 analyzed the different venous access sites (cephalic/subclavian/jugular) and described that the rate of catheter fracture was higher when the subclavian vein was used, of 13.5% when the overall rate was 3.9% in the 1543 cases studied. Several studies recommend the use of jugular venous access for patients requiring central venous catheters for long-term treatment due to the low incidence of mechanical complications and fractures associated2,4-6. The most common site of fracture is the junction between the reservoir and the catheter, but it can occur in any segment of the catheter. In the case of catheters placed via the subclavian vein, the fracture can occur in the trajectory between the clavicle and the first rib. Several causes can lead to catheter fracture: extrinsic compression near the junction between the catheter and reservoir combined with material fatigue caused by repeated bending of the catheter due to shoulder motion, sharp angles in the subcutaneous tunnel from the jugular vein to the reservoir, catheter trauma during placement or removal, damage caused by the needle when puncturing the reservoir, and, in the case of a subclavian vein access, intermittent compression between the first rib and the clavicle. This latter mechanism of fracture is known as pinch-off syndrome6.
The pinch-off syndrome can be evaluated with a radiologic scale of catheter distortion due to compression in the costoclavicular space: grade 0, absence of narrowing along the catheter course; grade 1, catheters show any degree of bending or deviation from a single curved course but no luminal narrowing; grade 2, catheters show some degree of luminal narrowing when passing below the clavicle (true pinch-off sign); and grade 3, catheters have been transected between the first rib and clavicle and have subsequently become embolized6.
Pinch-off syndrome can occur shortly (in months) after placement or can have a delayed presentation (in years), with a mean interval of 207 days and up to 534 days2,3. The most common clinical presentation is pain in the anterior chest region close to the insertion site with or without edema and catheter malfunctioning with intermittent inability to administer fluids and withdraw blood through the catheter. Palpitations or ventricular premature beats, chest pain and sepsis have also been described; however, in some cases, catheter fracture is asymptomatic, and its incidentally discovery in the routine chest X-ray of an embolized catheter3.
The key to the prevention of pinch-off syndrome is to avoid the clavicle and first rib during totally implantable venous access device implantation. Therefore, some authors reported that more lateral cannulation of the subclavian vein could reduce the incidence of the pinch-off syndrome3, while Jung et al.2 suggested the internal jugular vein approach since the incidence of catheter rupture is significantly lower. Chang et al.1 reported that a port-clavicle distance < 2.5 cm and duration of implantation > 200 days were independent predictors associated with increased risk of catheter fracture. Patients should be advised to avoid strenuous exercise of the shoulder girdle, since many fractures are located at the catheter-reservoir junction. To avoid long-term complications (fracture, migration, catheter disconnection), removal of implantable catheters that will not be used after treatment should be discussed with the oncologist and if the decision is to keep the device, radiological control during follow-up is necessary to early detect complications.
In summary, fracture and migration of totally implantable venous access devices is a rare complication that usually occurs with subclavian venous access. Once the diagnosis has been made, the fractured catheter should be removed by endovascular approach to avoid serious complications.
Referencias bibliográficas /References
1. Chang HM, Chou YC, Hsu SD, Liao GS, Chen TW, Hsieh CB, et al. Predictive Risk Factors for Fracture at Catheter of Totally Implant able Venous Access Devices via Subclavian Vein Insertion. J Med Sci. 2014; 34(4):161-5. [ Links ]
2. Jung PY, Ryu H, Jung JH, Lee E, Oh JH, Byun CS, Park LH. Complica tions of Central Venous Totally Implantable Access Port: Internal Jugular versus Subclavian Access. Korean J Crit Care Med. 2015; 30(1):13-7. [ Links ]
3. Ilhan BM, Sormaz İC, Türkay R. Pinch-Off Syndrome, a Rare Compli cation of Totally Implantable Venous Access Device Implantation: A Case Series and Literature Review. Korean J Thorac Cardiovasc Surg. 2018; 51(5):333-7. doi:10.5090/kjtcs.2018.51.5.333. [ Links ]
4. Tang T, Li Y, Zhang L, Li H, Geng C, Zhou T. Handling measures for the implantable vascular access device to prevent of catheter fracture/disruption. Int J Clin Exp Med. 2016; 9(2):3191-6 www.ijcem.com /ISSN:1940-5901/IJCEM0017669. [ Links ]
5. Wu CF, Ko PJ, Wu CY, Liu YH, Kao TC, Yu SY, Li HJ, Hsie HC. A single-center study of vascular access sites for intravenous ports. Surg Today. 2014; 44:723-31. [ Links ]
6. Hinke DH, Zandt-Stastny DA, Goodman LR, et al. Pinch-off syn drome: a complication of implantable subclavian venous access devices. Radiology. 1990; 177:353-6. [ Links ]
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
