










Servicios Personalizados
Revista

Articulo
 texto en
texto en  Español (pdf)
Español (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO
Links relacionados
-
 Similares en
SciELO
Similares en
SciELO
Compartir

 Permalink
PermalinkRevista argentina de cirugía
versión impresa ISSN 2250-639Xversión On-line ISSN 2250-639X
Rev. argent. cir. vol.116 no.1 Cap. Fed. mar. 2024 Epub 15-Feb-2024
http://dx.doi.org/10.25132/raac.v116.n1.1708
Scientific letter
Gastrointestinal bleeding due to ulcerated intussuscepted jejunal lipoma
1
 http://orcid.org/0000-0001-9229-2642
http://orcid.org/0000-0001-9229-2642
1
http://orcid.org/0000-0003-2563-5881
1
http://orcid.org/0000-0001-7272-3214
1Servicio de Cirugía General, Hospital Municipal de Vicente López, Prof. Dr. Bernardo A. Houssay. Buenos Aires. Argentina
Jejunal lipomas are rare benign mesenchymal tumors made up of adipocytes confined to the submucosa layer. They are usually asymptomatic and are incidentally found during imaging or endoscopic tests. Those measuring > 2 cm may become symptomatic as a result of complications as intestinal intussusception, obstruction and bleeding.
We herein report a rare case of intussusception of an ulcerated jejunal lipoma in an adult patient, that was diagnosticated in the setting of an intestinal hemorrhage.
Keywords: small intestine; gastrointestinal bleeding; intestinal obstruction
Gastrointestinal lipomas are benign fatty tumors most commonly found in the colon (64%) and small intestine (31%), predominantly in the ileum and, less commonly, in the jejunum with an incidence of approximately 2%3),(4. Small bowel lipomas are asymptomatic and are usually an incidental finding in imaging tests requested for other diseases, but may become symptomatic as the result of some complications such as bleeding, intussusception, or intestinal obstruction. This condition represents a diagnostic challenge because of its clinically silent course, vague and late symptoms, and difficult
We report a rare case of an ulcerated and intussuscepted jejunal lipoma in an adult patient, diagnosed in the setting of an obscure gastrointestinal bleeding.
A 67-year-old female patient presented with melena and cramping postprandial abdominal pain, moderate in intensity. She had experienced similar episodes of pain over the previous two months, with changes in bowel habits alternating between constipation and diarrhea, abdominal bloating, and nausea after ingestion.
The patient had a history of chronic microcytic anemia which was being treated with iron supplementation. On admission, the hematocrit was 20% with hemoglobin levels of 5.9 g/dL, so 100 mL of packed red blood cells were transfused.
On physical examination the patient was pale and mildly dehydrated; the abdomen was slightly distended, with generalized tenderness without guarding or peritoneal signs. The rectal examination revealed normal sphincter tone and black tarry stools with normal consistency.
The patient underwent upper gastrointestinal endoscopy, which did not show any abnormality until the second part of the duodenum was reached, and there were no signs of bleeding.
Because emergency colonoscopy and more complex endoscopic procedures were not available at the hospital, workup continued with a computed tomography scan of the chest, abdomen, and pelvis with oral and intravenous contrast. A circumferential thickening of 10 mm was observed in a jejunal loop with contrast enhancement, and a tendency to invagination, consistent with a tumorous process (Fig. 1).
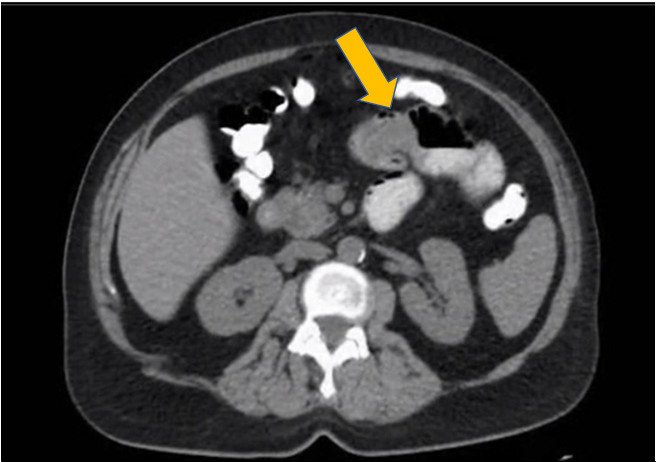
FIGURE 1 omputed tomography scan with oral contrast agent showing thickening of the small bowel with a tendency toward intussusception (arrow)
Based on the presumed diagnosis of active bleeding caused by the tumor, and without the possibility of performing endoluminal hemostasis, we decided to perform open surgery. A 5-cm endoluminal, intussuscepted mass, hard-elastic in consistency, was found 30 cm from the angle of Treitz, with no signs of intestinal obstruction (Fig. 2A). The tumor was resected with safety margins of 5 cm and a two-layer end-to-end anastomosis was constructed. The patient evolved without complications and was discharged on postoperative day 6.
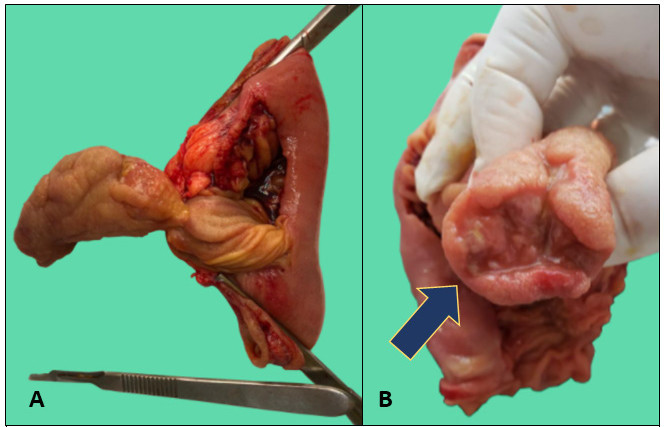
FIGURE 2 Small bowel resection. Jejeunal lipoma with intussusception (A) and ulceration (arrow) (B).
The postoperative pathology examination reported an ulcerated and intussuscepted lipoma measuring 4 × 2 cm (Fig. 2B).
Small bowel tumors are rare and include a wide spectrum of malignant and benign neoplasms6. Adenocarcinomas are the most common primary malignant tumors of the small bowel. Benign tumors like lipoma, fibrolipoma, fibroma, myoma, and heterotopias typically present as submucosal masses. It is not always possible to make a preoperative etiologic
diagnosis without prior biopsy2),(5).
Lipomas are mesenchymal tumors located in the submucosal layer in 90% of cases1 and appear as an extrinsic sessile protrusion into the lumen although because of peristalsis, they may become pedunculated and present with intussusception1. The incidence of intestinal lipomas ranges from 0.035% to 4.4% and are most commonly found in patients aged 50-70 years2.
They are usually small and asymptomatic, and their diagnosis is incidental3),(4. According to some published series, those measuring > 2 cm may produce non-specific symptoms: cramping abdominal pain (68%), nausea or vomiting (35%), gastrointestinal bleeding (33%), abdominal distension (12%), anemia (11%), and changes in bowel habits (9%)2,3,5. These symptoms are secondary to intussusception or intermittent obstruction4.
When intussusception of jejunal lipomas occurs, the mechanical effect against the intestinal wall can cause ischemia and ulceration, resulting in gastrointestinal bleeding1),(5. Intussusception is more common in children and is usually idiopathic. In adults, it is rare and associated with organic causes3),(5.
The diagnostic algorithm consists of an extensive set of tests. Upper gastrointestinal endoscopy and colonoscopy are the first line complementary tests for investigating gastrointestinal bleeding2),(5. However, they often yield negative results due to the anatomical location of these tumors. Other tests such as enteroscopy and capsule endoscopy may be useful, although they are not always available2),(3),(6.
Computed tomography scan is commonly used to assess abdominal pain. This method has a high success rate in diagnosing these tumors, with a sensitivity of 71 to 87% and a specificity close to 100% for detecting intussuscepted tumors of the small intestine. It is the most sensitive method for detecting intussusceptions although it does not offer therapeutic possibilities or biopsy6.
Endoscopic resection is another possibility mentioned in the literature for selected cases, based on tumor size and location6. Another option is conventional or laparoscopic surgical resection with anastomosis3),(6. The appropriate extent of safety margins is still a topic of discussion3. Symptomatic lipomas should be removed regardless of their size6.
Jejunal lipomas are rare tumors that are usually asymptomatic and are detected incidentally. Complications represent a real diagnostic challenge and include intestinal obstruction or gastrointestinal bleeding. Surgical resection is the treatment of choice for large and complicated lipomas.
Referencias bibliográficas /References
1. Balmadrid B, Gluck M. Chronic iron deficiency anemia caused by small-bowel lipoma. Gastrointest Endosc. 2014;79(4):678-9. Doi: 10.1016/j.gie.2013.10.048. Epub 2013 Dec 17. [ Links ]
2. Farkas N, Wong J, Bethel J, Monib S, Frampton A, Thomson S. A systematic review of symptomatic small bowel lipomas of the jejunum and ileum. Ann Med Surg. 2020; 58:52-67. Doi: 10.1016/j. amsu.2020.08.028. eCollection 2020 Oct. [ Links ]
3. Manouras A, Lagoudianakis EE, Dardamanis D, Tsekouras D K, Markogiannakis H, Genetzakis M, Katergiannakis V. Lipoma induced jejunojejunal intussusception. World J Gastroenterol. 2007 ;13(26):3641-4. Doi: 10.3748/wjg.v13.i26.3641. [ Links ]
4. Cuciureanu T, Huiban L, Chiriac S, Singeap AM, Danciu M, Mihai F, et al. Ulcerated intussuscepted jejunal lipoma-uncommon cause of obscure gastrointestinal bleeding: A case report. World J Clinic Cases. 2019;7(22):3765-71. Doi: 10.12998/wjcc.v7.i22.3765. [ Links ]
5. Li Z, Sun M, Song B, Shu Z. Gastrointestinal hemorrhage caused by adult intussusception secondary to small intestinal tumors: Two case reports. Medicine (Baltimore). 2018 97(34):et12053. Doi: 10.1097/MD.0000000000012053. [ Links ]
6. Kurniawan N, Rüther C, Steinbrück I, Baltes P, Hagenmüller F, Keuchel M. Tumours in the small bowel. Video J E of GI Endoscopy. 2014; 1(3):632-5. [ Links ]
Received: May 02, 2022; Accepted: June 14, 2022; pub: February 15, 2024
 This is an open-access article distributed under the terms of the Creative Commons Attribution License
This is an open-access article distributed under the terms of the Creative Commons Attribution License
