











 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkIntroduction
Focal Segmental Glomerulosclerosis (FSGS) is the most frequent cause of renal failure among the primary glomerulonephritis.1) FSGS patients, who do not achieve a remission in proteinuria, usually advance to end-stage renal failure (ESRF) within 5 to 10 years.2) Primary FSGS is characterized by hematuria, hypertension (HT), hypo-albuminemia, asymptomatic proteinuria, and decrease in glomerular filtration rate.3) Long-term development of FSGS is influenced by nephrotic range proteinuria at the time of diagnosis, kidney failure, tubulointerstitial fibrosis and the failure of treatment attempts.4
Treatment options for FSGS include blood pressure control, angiotensin converting enzyme inhibitors (ACEI) / angiotensin receptor blockers (ARBs), corticosteroids (CS) and cytotoxic drugs, such as calcineurin inhibitors (CNIs) and mycophenolate mofetil.5-6Kidney Disease Improving Global Outcomes (KDIGO) Clinical Practice Guideline for Glomerulonephritis suggests CS and immune-suppressivetherapy in idiopathic FSGS associated with clinical features of nephrotic syndrome.7
This retrospective study has been conducted on 47 primary FSGS patients, who had been diagnosed by renal biopsy and followed-up for at least 12 months. This study aims to analyze the admission symptoms of primary FSGS patients and to determine the possible symptoms of admission. Besides, we intended to reveal the criteria other than the existing remission criteria. Finally, although KDIGO suggestsCS therapy for initial treatment, we compared the treatment response rates of the participants that received CNI and steroids for initial treatmentversus only steroids treatment group. In short, we intended to analyze clinical data, therapy methods and immune-suppressive treatment response of the primary FSGS patients and compare data obtained with the findings in the literature.
Methods
The study was conducted on 47 patients, who had been followed-up for at least 12 months and diagnosed with primary FSGS at the Nephrology Department of Diskapi Yildirim Beyazit Education and Research Hospital between 1 June 2006 and 1 August 2017. Written informed consent was obtained from all participants. All patients were included in the study after signing informed consent forms. The study was performed in accordance with Declaration of Helsinki. Permission from the Ethical Commission Board of 24.07.2017 was obtained (N°:40/02). Data on patient characteristics were obtained from the routine tests that were administrated during diagnosis, treatment and follow-up and data obtained from the renal biopsies.
We obtained the parameters for treatment response from the 2012 KDIGO Clinical Practice Guideline for Glomerulonephritis. Reduction of proteinuria to 0.3-3.5 g/d (or spot urine protein/creatinine ratio 300-3500 mg/g [0-350 mg/mmol]), and stable serum creatinine (change in creatinine <25 %), or a decrease in proteinuria >50 % from baseline and stable serum creatinine (change in creatinine <25 %) were used to define partial remission of nephrotic syndrome in adults with FSGS. On the other hand, reduction of proteinuria to <0.3 g/day, or spot urine protein / creatinine ratio<300 mg/gr (<30 mg/mmol), and normal serum creatinine and serum albumin >3.5 g/dL (35 g/L) were used as parameters to define complete remission. When comparing the treatment responses, we presented the sum of the number of patients with partial and complete remission as the total number of patients with remission since the number of participants of our study was limited.
According to KDIGO 2012, the patients having proteinuria lesser than 3 gr/day were administered ACEIs or ARBs by dosing according to blood pressure. If the patients had proteinuria higher than 3 gr/day, prednisolone treatment was given as 0.5-1 gr/kg/day. CS treatment was continued at least for 6 months as maximized in the first 16 weeks. If CS was contraindicated 3-5/mg/kg/day, CNI treatment was ordered. If response for CS treatment was not achieved in six months, it was switched to CNI treatment.
Statistical analysis
Data obtained was analyzed by using Statistical Package for the Social Sciences (SPSS) for Windows computer program (release 22.0; SPSS Inc., Chicago, IL, USA). Data distribution was analyzed with Kolmogorov Smirnov test. Mean, and standard deviation (SD) were used for descriptive analysis of parametric quantitative data whereas number (n) and percentage (%) were used for the analysis of qualitative data. We used Student’s T-Test for parametric data and Mann-Whitney U Test for non-parametric data analysis. Pearson’s chi-square test was used for the analysis of qualitative data and p<0,05 was considered as statistically significant.
Results
Forty seven patients with primary FSGS were included in the study. Demographic characteristics of the patients can be seen in Table 1. Mean age of the participants was 45.68 (± 13.92) and the number of male patients was 22 (46.8 %). Fifteen patients (31.9 %) had hematuria at the time of biopsy. Besides, 25 patients (53.2 %) had HT, 11 (23.4 %) had diabetes mellitus (DM), and 2 patients (4.3 %) had cardiovascular diseases (CVD). Mean duration of disease was 3.38 (± 2.40) years. The laboratory features of the patients at the time of biopsy can be seen in Table 1.
The average glomerular number was 20.53 (±13.23), 44.70% of the patients had sclerosis, 43% had interstitial fibrosis; and, 40% of the patients had tubular atrophy. The interstitial fibrosis ratio of CNI group was 30.85±6.26 whereas this ratio was 28.96±6.80 in CS group. The difference between groups was not statistically significant (p>0.05) (Table 4). Tubular atrophy in CNI group was 35.7±7.33 and 32.31±5.72 in CS group and this was not statistically significant (p>0.05). (Table 4)Treatment methods of the primary FSGS patients can be seen in Table 3.
Twenty one patients (44.68%) received ACE/ARB therapy, 7 patients (14.89%) had CS therapy, and the remaining 19 patients (40.42%) received CNI and low dose CS therapy. Six (12.7%) of these 19 patients used CNI and low dose CS without prior CS therapy whereas 13 patients (27.6%) received CS therapy prior to CNI and low dose CS. According to KDIGO 2012, the patients having proteinuria lesser than 3 gr/day were administered ACEIs or ARBs by dosing according to blood pressure. If the patients had proteinuria higher than 3 gr/day, prednisolone treatment was given as 0.5-1 gr/kg/day. CS treatment was continued at least for 6 months as maximized in the first 16 weeks. If CS therapywas contraindicated, 3-5/mg/kg/day CNI treatment was ordered. If response for CS treatment was not achieved in 6 months, it was switched to CNI treatment. Comparison of the primary FSGS patients in terms of first-line immunosuppressive therapy options reveals that glucose levels of the patients that received CNI and low dose CS therapy was statistically significantly higher (p=0.032). Apart from this, we found no statistically significant difference between the patients that received CNI and low dose CS and the patients that received CS as first-line treatment in terms of demographic or baseline laboratory characteristics (p>0.05) (Table 4).
Comparison of the laboratory characteristics for the sixth month in Table 5reveals that glucose levels of the patients that received CNI and low dose CS was statistically significantly higher than the patients that received CN (p=0.038). Once again, we did not find any statistically significant difference between the two groups in terms of other laboratory characteristics (p>0.05). Eleven patients had diabetes and 6 patients were given CNI as an initial treatment. These 6 patients had risk factors other than diabetes. Five patients with diabetes, whose diabetes were regulated, were given CS treatment as an initial treatment.Table 6, which shows the laboratory characteristics of the participants for the 12th month, reveals that glucose levels of the patients that received CNI and low dose CS therapy was statistically significantly higher that the patients that received CN (p=0,018) whereas the difference between the two groups in terms of the other remaining laboratory characteristics was not statistically significant (p>0.05).
Table 7 shows the treatment responses of the two groups with different initial treatment for the 6th and the 12th months. The sum of the patients with partial and complete remission was shown as the number and the percentage of patients with remission in the table. For both groups, there were no patients with complete remission in the 6th month. Regarding the responses of the patients to first-line immunosuppressive therapies in the sixth month, we found that 3 (50%) of 6 patients that received CNI and low dose CS without prior CS therapy and 4 (57.1%) of 7 patients that received CS therapy achieved partial remission.
On the 12th month, we found that 4 (66%) of 6 patients that received CNI and low dose CS without prior CS therapy and 6 (86%) of 7 patients that received CS therapy achieved remission. The comparison of the findings reveals no statistically significant difference between two groups (p>0.05) (Figure 1, Table 7). Three (50%) of the 4 patients with remission achieved partial and the remaining 1 patient (%16) achieved complete remission in the CNI group. On the other hand, 4 (57%) of the 6 patients with remission achieved partial and 2 (29%) patients achieved complete remission in the steroid group (Figure 2). Given the number of patients with remission was low in both groups, we compared the sum of the patients that achieved partial and complete remission.
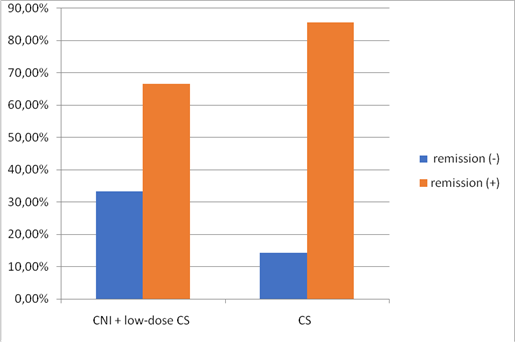
Figure 1 Remission rates in patients with initial therapy CNI + low-dose CS and CS only,66 % of the patients that that received CNI and low-dose CS and 86 % of patients that received CS therapy achieved remission in the 12th month. However, we did not find any statistically significant difference between two groups (p>0.05)
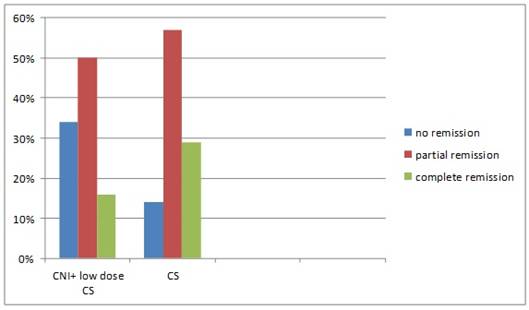
Figure 2 66 % of the patients (16 % complete, 50 % partial remission) that that received CNI and low-dose CS and 86 % of patients (29 % complete, 57 % partial remission) that received CS therapy achieved remission in the 12th month
Comparison of the laboratory characteristics of the primary FSGS patients that achieved or did not achieve remission at the end of 12 months with their baseline laboratory characteristics reveals no statistically significant difference between two groups (p>0.05) (Table 8). The patients who had remission had statistically significantly lower ratio of interstitial fibrosis (29.1 ± 5.96 vs 36.1 ± 3.3; p=0.001) and tubular atrophy ratios (32.99 ± 6.2 vs 40.56 ± 3.15; p=0.001).
At the end of the first year, 33 of the 47 patients achieved remission whereas the remaining 14 patients did not achieve remission. Regarding the responses, we found that only 1 patient (2.1%) achieved complete, 30 patients (63.8%) partial remission, and the remaining 16 patients (34%) achieved no remission in the sixth month. On the 12th month, we found that 6 patients (12.8%) achieved complete remission, 27 patients (57.4%) achieved partial remission while 14 patients (29.8%) achieved no remission.
Discussion
FSGS is the most common histological finding of glomerular damage and is one of the most important reasons of nephrotic syndrome in adults and children.8) Some evidence suggest an increase in the prevalence of FSGS in children.9Research shows that FSGS is brought about by several genes including transient receptor potential cation channel subfamily c member 6 (TRPC6).10) FSGS recurrence rate after kidney transplantation is ranging between 20 % and 40 %, and it is associated with poor graft survival.11) It has become the most common primary glomerular disease seen in the renal failure patients in the USA.12) The study conducted by the Glomerulonephritis Study Group of Turkish Society of Nephrology reveals that membranous nephropathy (28.8 %) is the most frequent primary glomerular disease in Turkey, which is followed by FSGS (19.3 %) and IgA nephropathy (17.2 %).13
This study was conducted on 47 primary FSGS patients that were followed-up between June 2006 and August 2017. We evaluated clinical findings, therapy methods and responses of the patients to first-line immunosuppressive therapies, including steroid and CNI therapies. Mean age of the 47 participants was 45.68 (±13.920),22 patients (46.8%) were male whereas 25 patients (53.2%) were female (Table 1). Primary FSGS is more common among the male population and the incidence of FSGS-related ESRF is 1.5 to 2 times higher among males compared to female population.14) Our study included slightly more female participants and found a mean age similar to other studies.15
FSGS patients are mostly characterized by acute or sub-acute onset nephrotic syndrome, peripheral edema, hypo-albuminemia and >3,5 g/day proteinuria.3) Studies that evaluated the clinical features of primary FSGS patients found that 75-95% of the admitted patients had nephrotic syndrome. Nearly 50% of the patients had hematuria whereas 20% had HT.16) As Table 1 demonstrates, 31.9% of the patients of our study had hematuria whereas 53,2% had HT at the time of biopsy. Similar to our findings, other studies note the high frequency of HT in FSGS patients. For example, the study of Deegens et al. on FSGS patients found that 80% of the initially untreated patients and 50% of treated patients had hypertension.17
Histopathological characteristics of the renal biopsies of the primary FSGS patients in our study shows that average number of glomeruli was 20.53 (±13.23), 44.70% of the patients had sclerosis, 43% had interstitial fibrosis;and40% of the patients had tubular atrophy as depicted in Table 2.
The patients who had remission had statistically significantly lower ratio of interstitial fibrosis (29.1±5.96 vs 36.1±3.3; p=0.001) and tubular atrophy ratios (32.99±6.2 vs 40.56±3.15; p=0.001). Interstitial fibrosis in FSGS is associated with poor renal survival.18) The study of Heybeli et al. showed for the first time that mesangial C4d deposition is an independent predictor of disease progression and treatment failure in patients with primary FSGS.19) However, the main prognostic indicator of renal survival is the initial response of proteinuria to therapy irrespective of histology type.20
Compatible with suggestions of the KDIGO, 21 patients were treated with renin-angiotensin system (RAS) blockade and 7 patients received CNI as first-line immunosuppressive therapy. The remaining 19 patients received CNI and low dose CS therapy(Table 3). However, 6 of the 19 patients received CNI and low dose CS without prior CS monotherapy because of uncontrolled DM (4 patients), osteoporosis (1 patient) and psychiatric reasons (1 patient). Despite the fact that KDIGO7 suggests steroids as first-line immunosuppressive therapy, we compared steroids and CNI therapy as first-line therapies. KDIGO suggests CS as first-line therapy if there are no contraindications. The study of Huang et al. showed additional glucocorticoids therapy is more efficacious compared to ACEI/ARB alone in the treatment of patients with primary FSGS with moderate proteinuria (urine protein between 1.0 and 3.5 gr/day).21) Complications due to long-term CS use may be decreased by every-other-day therapy, which may achieve results similar to daily therapy.7) Immunosuppressive medications may be used on their own or in combination with low dose CS as alternative for the patients, who cannot tolerate long-term high-dose CS. However, the risk of nephrotoxicity is higher for the patients that have high serum creatinine and sclerotic glomeruli prior to treatment and that receive cyclosporin more than 5.5 mg/kg/day.22
Similar to our study, in various studies, medications other than steroids were used as first-line immunosuppressive therapy. In retrospective study of Goumenos et al. that followed 51 FSGS patients for a period of 5 years, 25 patients were treated with CS or a combination of CS with azathioprine or CsA (cyclosporin) whereas the remaining 26 patients received no immunosuppressive drugs. The study found an increase of baseline serum creatinine by 50% in 2 treated and 9 untreated patients. CS monotherapy led to remission in 62.5% of patients whereas 80% of the patients that received CS and azathioprine and 85.7% of the patients that received CS and CsA achieved remission. Goumenos et al. concluded that CsA could be used as initial treatment for patients that cannot tolerate high-dose CS.23) On the other hand, the study of Duncan et al. that used tacrolimus therapy as initial treatment, achieved remission in all of the six patients.24
Our study compared the demographic (age and gender), laboratory (creatinine, albumin, hematuria, etc.) and clinical features (DM, HT, CVD, etc.) of the baseline, 6th month and 12th month of the primary FSGS patients that received CS versus CNI and low-dose CS therapy for an average of three years. We found that glucose and DM levels of the primary FSGS patients that received CNI plus low-dose CS therapy was statistically significantly higher than the patients that received CS. Six of 11 diabetic patients received CNI. The reason why CS was not given was not only diabetes. Patients with regulated diabetes were given CS. We found no other statistically significant difference between the two groups. (Tables 4, 5, 6)
About 66.7% of the patients that received CNI and low-dose CS and 85.7% of patients that received CS therapy achieved remission in the 12th month. However, we did not find any statistically significant difference between the two groups (p>0.05) (Table 7,Figure 1). Baseline proteinuria levels of the patients that received CNI and low-dose CS (7636.16±4041.95 mg/day) and CS therapy (7747.14±4840.91 mg/day) decreased to 2562.83±2532.84 mg/day and 3278.71±2646.54 mg/day, respectively. However, we did not find any statistically significant difference between the two groups in terms of decrease in proteinuria levels (p=0.630). (Table 6)
Regarding the treatment responses, we found that 2.1 % of the patients achieved complete remission, 63.8 % achieved partial remission while 34 % had no remission in the sixth month. For the 12th month, 12.8 % of the patients achieved complete remission, 57.4 % partial remission whereas 29,8 % achieved no remission. At the end of one year, in our study, 27 of the 33 patients achieved partial and 6 patients achieved complete remission. One of the 6 patients with complete remission belonged to the group that received CNI, 2 received only CS and the remaining 3 received CNI after CS. Since the number of patients was low, we did not conduct statistical analysis for these patients.
Spontaneous remission rate is less than 10 % for the FSGS. However, different treatment methods increased remission rates up to 70 %.25) Remission rates after CS therapy ranged between 28 % and 74 %.(7) Complete and partial remission rates in our study were 70.2 % after one year. Retrospective study of Toronto Glomerulonephritis Registry Group followed 281 nephrotic FSGS patients for at least one year. Two-thirds of the patients received immunosuppressive therapy, including high-dose glucocorticoid (50 %), cytotoxic agent (19 %) and cyclosporine (12 %); whereas 54 % of the patients received ACEI or ARB therapy. The participants were followed-up for an average period of 64 months. 20 % of the patients had complete, 41 % had partial remission and 39 % of the patients had no remission.26
Comparison of the demographic and baseline laboratory features of patients in our study that achieved or did not achieve remission reveals no statistically significant difference between two groups (p>0.05) (Table 8). Baseline serum creatinine levels and remission achievement rate have been important indicators of ESRD.27Two (4.3%) FSGS patients in our study had ESRD and received renal replacement therapy. Prognostic factors in FSGS include proteinuria and creatinine levels, histopathological characteristics of biopsy, and more importantly, treatment response.28
This study aimed to compare the clinical and treatment findings of FSGS with the findings in the literature. The study has two main limitations: firstly, it was a retrospective study, and secondly, this study has been conducted at a single center with a small number of patients. Despite the limitations, we found that admission symptoms and treatment responses of the FSGS patients were similar to the literature. FSGS is common among the male population and people between the ages of 35 and 50. Mean age of the FSGS patients was similar to the literature. However, the number of female primary FSGS patients was higher in our study. Primary FSGS patients mostly have proteinuria at nephrotic-range at admission time. Hematuria is common and may occur in nearly 50% of the patients whereas 20% of the patients may have HT. Proteinuria rates of the patients in our study is parallel to the literature. However, contrary to the literature, hematuria is less often (31.9%) and HT is more frequent (53%) in our study. Spontaneous remission rate is less than 10% for the FSGS. However, remission rates may be increased to nearly 70% by using different treatment methods. In our study, 12.8% of the patients achieved complete remission and 57.4% partial remission at the end of 12 months. At the end of one year, 16% of the patients in the CNI group achieved complete remission and 50% achieved partial remission. The percentages of complete and partial remission for the patients in the CS group were 29% and 57%, respectively (Figure2). Complete and partial remission rates amounted to a total of 70.2% after one year similar to the literature.
Conclusion
We found statistically significantly lower ratio of interstitial fibrosis and tubular atrophy for the patients with remission. In line with the literature, our study revealed the importance of pathological findings for the clinical prognosis of FSGS. KDIGO suggests steroids as first-line immunosuppressive therapy. Although the sample was limited, we found that CS and CNI had equal efficiency as first-line therapy. Steroid, which is suggested by the KDIGO, may be used as a first-line therapy option due to its lower costs. However, CNI may also be used for patients with steroid intolerance. Given the fact that the sample of this study is limited, further studies with a larger sample size should be conducted.

