











 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkIntroduction
Since the beginning of the COVID-19 pandemic, there has been a lot of debate about the usefulness of corticosteroids for the treatment. From the beginning, they were thought to have even a potential harmful effect1; subsequently they showed their usefulness in patients with severe acute pneumonia with requirement of oxygen therapy or some type of ventilatory support2. Patients who overcome the acute phase of the disease may show clinical and radiological alterations3, 4, 5 in the post-acute period, with their long-term evolution not clearly known yet. It is very important to have tested treatments in order to accelerate recovery and reduce potential sequelae6. Corticosteroids would counteract the inflammatory process triggered by the viral infection and perpetuated by an “uncontrolled” immune system7. This case report tried to give at least an initial response to this hypothesis, describing the clinical and radiological evolution of patients who received that treatment.
Materials and Methods
For this report, we included 18 patients with severe8 COVID-19 pneumonia who 14 days after the be ginning of the symptoms persisted with significant clinical alterations (dyspnea FC III - IV according to the NYHA scale, not explained by any other cause), altered oximetry readings (oxygen desaturation (O2) breathing ambient air, not present before COVID-19) and/or tomographic alterations (bilateral parenchymal infiltrates suggestive of organizing pneumonia (OP) or late appearance of new infiltrates not explained by an infection of a different etiology). The patients were evaluated and treated in 3 polyvalent private medical institutions of the Autonomous City of Buenos Aires.
All the patients received treatment with dexamethasone during the acute period, according to what was described in the Recovery study2, indicating in some cases other therapeutic measures based on what was approved at the moment of the hospitalization (convalescent plasma, hyperimmune equine serum, hydroxychloroquine, antiretroviral medicines).
We performed chest tomographies (CAT) upon hospitalization, in cases of clinical changes showing worsening of the patient’s respiratory condition, at the beginning of corticosteroid treatment and 4 weeks after the beginning of such treatment. We used intravenous pulse corticosteroids (methylpredniso lone, 500 mg a day, 3 doses) in patients with mechanical respiratory assistance (MRA) or spontaneous breathing with high O2 requirement through high flow cannula or mask with reservoir bag. Patients with O2 requirement per conventional nasal cannula or less than 5 liters/minute were prescribed oral corticosteroids (meprednisone, 0.5 to 0.75 mg/kg/day). This regimen was administered after the intra venous dose in patients who required pulse dosing. The treatment was extended for 3 to 6 months, like other organizing pneumonias9, with progressive decrease depending on the clinical, oximetric and radiological response. Patients with suspected aggregated infections underwent a bronchoscopy (FBC) with bronchoalveolar lavage (BAL) and transbronchial biopsies (TBB), provided that it was clinically possible and safe, in order to dismiss the suspicion and also to try and record the anatomopathological characteristics of the inflammatory process shown in the images.
Ethical consideration
This draft is a series of case reports. Merely descriptive approaches focused on the interpretation of the results have been adopted, trying to reach valid conclusions. It hasn’t been produced in the context of a research trial with control groups or randomized treatments. The patients signed their informed consent upon hospitalization and before performing the bronchoscopy. It follows the guidelines of the Personal Data Protection Act No. 25,236, particularly sections 1, 5 subsection D, 8 and 11, subsection D.
Results
15 out of the 18 patients included were male and 3 female, with a mean age of 58.4 ± 13.6 years. There were five patients without a pathological history. The other 13 had clinical and oncological medical history (Table 1). All the patients were administered dexamethasone, 6 mg/day intravenously or orally for 10 days, according to the Recovery study. Mean time from the onset of symptoms until the beginning of corticosteroid, “non-dexamethasone” treatment was 28.1 ± 10 days. Given the severity of their clinical condition, 7 patients initially received intravenous treatment with methylprednisolone (5 patients with high-flow nasal cannula or mask with reservoir bag and 2 with MRA). Those treated with oral corticosteroids received meprednisone, 50 ± 12 mg/day.
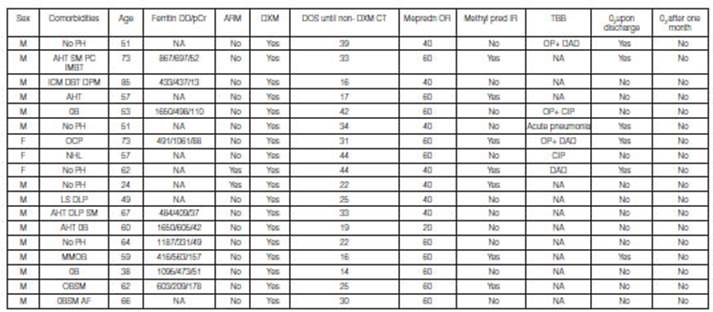
6 patients underwent FBC with BAL and TBB. No germs were isolated. The anatomopathological report showed OP pattern in 3 patients: it was associated with diffuse alveolar damage (DAD) in 2 cases, and with lymphocytic inflammation or cell interstitial pneumonia (CIP) in 1 patient. One patient showed isolated DAD changes, another patient had acute neutrophil inflammatory damage and the remaining one reported CIP.
Six of the 18 patients required home O2 supply after hospital discharge, due to dyspnea or desatura tion. One month after discharge, none of the patients continued with the indication of O2 supply.
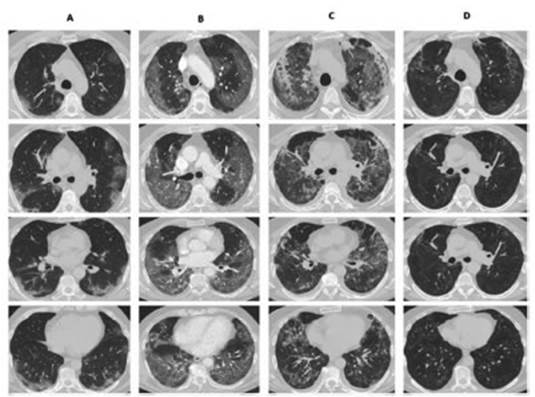
The chest CAT performed 4 weeks after hospital discharge showed in all of the patients a clear re duction of the parenchymal involvement, and the most frequent finding was ground-glass persistence associated with septal thickening (Figures 1and2). Only 1 patient had traction bronchiectasis and another one showed images compatible with pneumatocele.
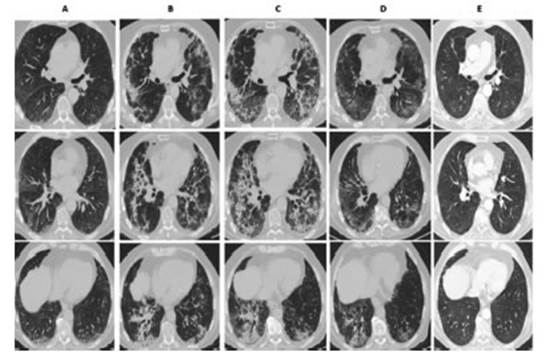
Figure 1 73-year old man. Column A: 11 days since the onset of symptoms. B: 26 days since the onset of symptoms. C: 30 days since the onset of symptoms/ 1st day of intravenous meth ylprednisolone. O: 40 days since the onset of symptoms. 7th day of oral meprednisone (60 mg/ day). E: 119 days since the onset of symptoms, receiving meprednisone, 10 mg/day.
Discussion
When the presence of the SARS COV 2 infection became known, it was assumed that the clinical pre sentation was the expression of the viral infection and the post-acute period was the consequence of an immune system deregulation, more commonly known as “cytokine storm”7. Corticosteroid therapy during the infectious acute phase showed its usefulness in the Recovery study,2 which described an improvement in survival with the use of dexamethasone in patients requiring some type of respira tory assistance. Other authors reported similar benefits using higher doses of methylprednisolone10-12. Once the acute infectious process is resolved, like other more common etiologic agents13, COVID-19 may evolve towards a clinical condition compatible with secondary organizing pneumonia14-15. This is shown in the tomographic characteristics observed during the evolution of the infection6. In the anatomopathological necropsy reports and in some “in vivo” biopsy reports, the damage pattern was confirmed, associated with other observed patterns such as diffuse alveolar damage and acute fibrinous and organizing pneumonia (AFOP)14,17.
At the moment, the natural evolution of the clinical and radiological consequences post-acute COVID-19 infection is unknown. But given the number of patients affected by this pandemic, it is imperative to find some treatment that accelerates recovery and reduces respiratory abnormalities as potential sequelae to the minimum. According to various reports3,4,18, 39% of patients remained asymptomatic one month after hospital discharge, up to 63% showed spirometric alterations 3 months after the infection and 30% after one year, and 25% of the patients still showed radiological alterations one year post-infection.
Myall et al18 described in their work one approach that is similar to the one described in this report, but they began corticosteroid therapy 6 weeks after discharge in patients whose clinical or radiological findings were suggestive of persistent pulmonary lesion, mainly OP. In that case they indicated only 3 weeks of treatment with oral corticosteroids and their results showed symptomatic, radiological and spirometric improvement. The French guidelines19 for the management of post-COVID respiratory se quelae also supported this approach, considering all the patients who remained asymptomatic or with radiological or spirometric alterations up to even 1 year post-infection as capable of being treated. Ac cording to these guidelines the treatment is more similar to the conventional treatment of organizing pneumonia, starting with prednisone, 0.5 mg/kg for one month and then reducing 10 mg every month.
Future studies shall define if corticosteroid therapy has to be administered during the immediate post-acute period or subsequently if there is no clinical or radiological improvement. They must also evaluate whether there is a group of patients that need the corticosteroid therapy of the acute period to continue for more than 10 “formal” days in cases of radiological or clinical markers suggestive of the subsequent “negative” evolution described herein. Finally, it would be adequate to define the dose and duration of the corticosteroid therapy considering that the underlying cause of the inflammatory process has been resolved (acute viral infection), and which are the adverse effects related to prolonged use.
This retrospective work about a series of cases has clear limitations: the lack of a control group and randomization of the indicated treatment. Treatment decision making was defined by the attending physician, who clinically analyzed each separate case. Still, the favorable results that were described allow us to suggest that systemic corticosteroid therapy indicated after the acute period would have a beneficial effect, both clinical and radiographic, in patients with torpid evolution of severe pneumonia caused by COVID-19, provided that the presence of pulmonary tromboembolism or bacterial or fungal superinfection or other causes of dyspnea and/or pulmonary infiltrates (heart failure, drug-induced pulmonary toxicity, exacerbation of underlying pulmonary diseases) that may justify the clinical con dition beyond the unfavorable evolution of the patient’s COVID-19 has been properly dismissed. It is necessary to conduct prospective studies duly designed to clearly establish the benefit suggested in this work, defining clear inclusion criteria, forms of therapy, dose and duration.
Conclusion
Systemic corticosteroid therapy administered after the acute period would have a potential beneficial effect in patients with severe pneumonia caused by SARS COV 2 who 14 days after the onset of symp toms still show clinical or radiological manifestations suggestive of damage generated by the immune response to the virus.

