











 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkINTRODUCTION
With the growing recognition of asthma and COPD as heterogeneous diseases that share clinical, func tional and inflammatory similarities, attention has been drawn to patients with clinical features of both diseases, who were qualified as patients with asthma-COPD overlap (ACO)1,2. In smokers, asthma is considered a risk factor for developing COPD, as shown in the Tucson epidemiologic study, with a 12 times higher risk in asthmatic smokers versus non-asthmatic smokers3.
Another information that supports the coexis tence of the asthma-COPD overlap is the fact that it has been proven that bronchial hyperresponsive ness is an independent predictor of COPD and mortality from respiratory causes in population-based studies4, as well as a risk indicator of the accelerated decline in lung function in patients with mild COPD5.
At present, there isn’t any evidence supporting the therapeutic decisions in patients with ACO, since traditionally they have been systematically excluded from research protocols in order to main tain the homogeneity of the population among those who complied with the standard definitions of COPD or asthma1.
Approximately one every four patients with COPD has asthmatic features; those were recently qualified as ACO by the Global Initiative for Asth ma (GINA) and the Global Initiative for COPD (GOLD). Therefore, to identify them in real life poses a diagnostic and therapeutic challenge1; also the accurate definition of ACO is still controversial6.
However, there is emerging agreement that some of the key features of ACO include persistent airflow limitation defined as a post-bronchodilator FEV1/FVC ratio < 70%, in symptomatic individu als aged 40 years or older with well-documented history of asthma during childhood or early adult hood, and exposure to cigarette smoke (more than 10 p/y) or to biomass1.
In patients with COPD, the ACO diagnosis is fundamental for including the prescription for an inhaled steroid (ICS). On the other hand, asth matic patients diagnosed with ACO don’t show sig nificant therapeutic implications, because initial therapy with the combination of long-lasting beta agonists plus ICS is the same for pure asthmatics and patients with asthma-COPD overlap2.
The impact of the correct diagnosis for and ade quate treatment choice is crucial, because patients with ACO have a higher symptom burden, such as dyspnea and cough, an increased risk of rapid decline in FEV1, of exacerbations, hospitalization and mortality due to COPD1 when compared to patients with pure COPD or asthma.
The purpose of this study about the prevalence of the asthma-COPD overlap through the database of the EPOC.AR epidemiological study7 was to know the reality of our country, since up to now there isn’t any information regarding this topic.
Objectives
Primary: to determine the prevalence of ACO in the EPOC.AR epidemiological study regarding the prevalence of COPD in Argentina7.
Secondary
1. To evaluate and analyze the clinical features of patients with ACO compared to patients with COPD.
2. To describe and compare treatments received by patients with ACO and COPD.
MATERIALS AND METHODS
This study is a sub-analysis of the EPOC.AR study which includes all the patients diagnosed with COPD and differen tiates (within that group) patients with diagnostic criteria of ACO from those with COPD. The EPOC. AR. study7 is multicenter, cross-sectional, and population-based. The population of the study has been randomly selected using cluster sampling and was divided into 6 urban clusters of Argentina, with the purpose of establishing the prevalence of COPD and evaluate the clinical and sociodemographic characteristics of patients, the treatment, and the various risk factors. The study was conducted between August 2014 and May 2016.
The following urban clusters were selected: La Plata, Rosario, Autonomous City of Buenos Aires, Northern Region of Gran Buenos Aires, Córdoba and Mendoza. The sample was selected by means of proba bility, multistage cluster sampling based on map units and described in detail in supplementary material. Each selected person was invited to participate in the study. Subjects who accepted were requested to sign the informed consent7.
Definition of terms
COPD was defined as a post-bronchodilator FEV1/FVC ratio < 0.7, and the GOLD 2017 classification was used to define the degree of obstruction and multidimensional ABCD assessment10.
GOLD 2017 classification10 Global Strategy for the Diagnosis, Management and Prevention of COPD, Global Initiative for Chronic Obstructive Lung Disease (GOLD) 2017. http://goldcopd.org
Definition of ACO
The diagnostic criteria for ACO were recommended by a panel discussion with experts from North America, East Europe and Asia that took place in Denver (CO, USA) on May 16th, 2015.
There are 3 major criteria and 3 minor criteria. The Committee recommends the presence of all 3 major criteria and at least 1 of the minor criteria.
Even though the Committee acknowledges that it is an arbitrary definition that needs validation, these are dynamic criteria, and with the addition of new data, modi fications will be required11.
MAJOR CRITERIA
1. Persistent obstruction of the airway (post-BD FEV1/FVC < 70% or LLN) in individuals aged 40 or older.
2. Smoking (at least 10 packs/year) or exposure to indoor or outdoor air pollution (for example, biomass).
3. Documented history of asthma before 40 years or broncho dilator response > 400 ml for FEV1.
MINOR CRITERIA
1. Documented history of atopy or allergic rhinitis.
2. Bronchodilator response for FEV1 < 200 ml.
3. Peripheral blood eosinophil count ≥ 300 cells-Ul-1.
NOTE: the presence of eosinophilia in peripheral blood will be excluded from minor criteria, since no blood extrac tions were performed in patients from the EPOC. AR study for any type of test.
EXACERBATIONS
Exacerbations were defined according to the 2017 GOLD Guides10 as acute worsening of symptoms that require additional treatment.
Exacerbations are classified as:
1. MILD: treated with short-acting bronchodilators (SABDs).
2. MODERATE: treated with SABDs plus antibiotics and/or oral corticosteroids.
3. SEVERE: the patient requires hospitalization or visits to the emergency department. They may also be associated with acute respiratory failure.
The following variables were analyzed in patients diag nosed with COPD:
1. Medical record data:
• Smoking history (packs/year).
• History of asthma, atopy or allergic rhinitis.
• Respiratory symptoms: CAT (COPD Assessment Test) questionnaires8 and mMRC (Modified Medical Research Council) questionnaire.9
• Frequency of exacerbations the previous year with/ without hospitalization.
• Systemic comorbidities.
• Treatment received.
2. Pre- and post-BD spirometries.
RESULTS
The population with diagnostic criteria for COPD included 504 patients, but there weren’t any available data in 6 of them, so the analyzed popu lation was 498 patients (n = 498). The prevalence of COPD was 14.5% (CI: 13.4-15.7%). In this population we detected 95 patients with criteria for ACO, mostly males (53.4%) with a mean age of 63.6 years (SD ± 10.83) distributed in the fol lowing way: 28% of the population between 40-59 years, 52% between 60-75 years, and 20% more than 75 years.
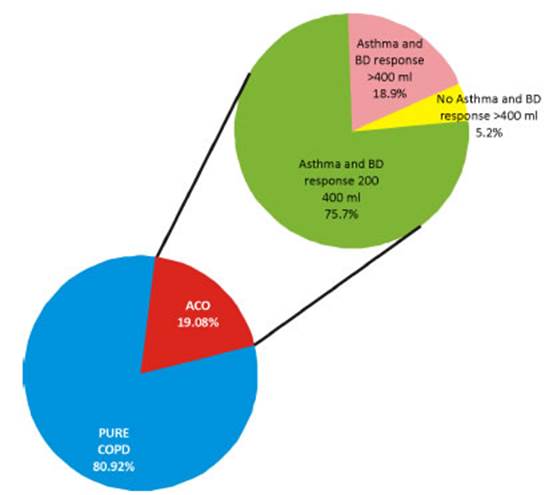
The prevalence of ACO in the population with diagnostic criteria for COPD was 19.08% (95% CI: 15.6-22.5), which is 2.6% of the whole population of the EPOC.AR study. The prevalence of cases compatible with ACO, according to the diagnostic criteria that were used, are shown in Figure 1, with 1% of patients with no history of asthma and a BD response ≥ 400 ml, and 32.7% of patients with asthma but with different bronchodilator respons es: 3.6% with a BD response ≥ 400 ml and 14.5% with a BD response of 200-400 ml (Figure 2).
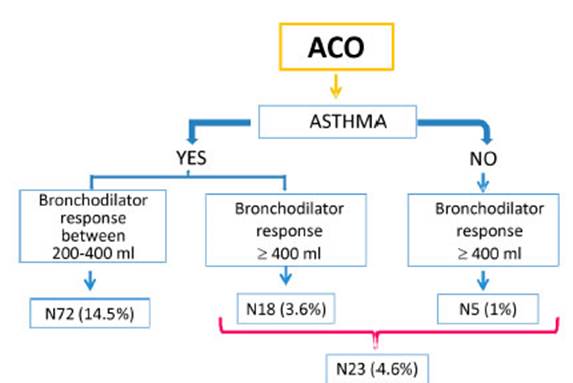
4.6% of the whole population with diagnostic criteria for ACO, including asthmatic and non asthmatic patients (n = 23) showed a BD response ≥ 400 ml.
Table 1 compares the populations of patients with COPD with those with diagnostic criteria for ACO; it was detected that the latter show a lower mean age and lower average pre-BD FEV1, both with statistical significance (p < 0.01). There were also significant differences in post- BD spirometries, since a higher BD response was found (p < 0.05) in patients with ACO. Also a higher frequency of sibilance (p < 0.01; CI 2.75-7.64%), and larger increase in previous asthma and bronchitis diagnoses (p < 0.01; CI 3.79-10.05%) were detected, and in 26.08% (CI 22.16-29.99%) the patient was aware that some family member had an asthma diagnosis. If we consider the medication of patients with ACO, they mostly used inhaled corticosteroids com bined with long-acting B2 agonist bronchodila tors (ICS/LABA) p < 0.05; CI 1.1-5.3%. The fre quency of exacerbations was higher in the group of patients with ACO (12.47%; CI 9.56-15.39%), with an increase in the use of ATBs (p < 0.05) indicated by health professionals in 90.48%. Patients with ACO showed 2.49 times (95% CI: 1.50-4.15) more probabilities of having respira tory problems that altered their daily activities or caused absence from work, in comparison with pure COPD patients (p < 0.05).



DISCUSSION
There are wide variations in the prevalence of ACO that are related to the type of population under evaluation (database analysis or clinical trials), the different criteria used for the identi fication of ACO, and the definition of asthma and COPD6, and also to the age group (all the adults or subjects older than 40 years).
The prevalence of ACO in the general popula tion oscillates between 1.6 and 4.5%, in patients with COPD, between 12.1 and 55.2%, and in pa tients with asthma, between 13.3 and 61%13.
In the UPLIFT (Understanding Potential Long-term Impacts on Function with Tiotropium) study, when considering the criterion of a significant re sponse to bronchodilator, the prevalence in COPD patients was 52%16.
In a recently published meta-analysis including 19 studies, the prevalence of ACO among patients with a COPD diagnosis was 27% in population-based studies, and 28% in studies carried out in hospitalized patients6.
In Spain, results from the recent CHAIN study including 831 COPD patients from 36 university hospitals showed a prevalence of ACO of 15% (us ing the specific major and minor modified GesE POC [Spanish COPD Guidelines] criteria). These results are similar to those of the COPDGene study, which were 13%6.
In our study, the prevalence of ACO was 19.08% (CI 15.6-22.5) in the COPD population of the EPOC.AR study, representing 2.6% of the total population of this population-based study (N 3,469). These percentages coincide with the data reported in the literature. But ultimately, while the prevalence of ACO ranges widely ac cording to the source that was taken into account and the criterion used to define it, we could say that it ranges between 1.6 and 4.5% of the adult general population and between 15 and 25% of the adult population with chronic obstruction of the airflow6.
Llanos et al reported that patients with COPD had lower bronchodilator FEV1 than patients with ACO14, but in our study we observed that patients with ACO had significantly lower pre-bronchodilator FEV1.
Several studies showed that individuals with ACO have higher frequency of respiratory symp toms in comparison with subjects with pure COPD. Maselli et al15 found that this group of patients shows higher frequency of dyspnea and a great impact on their quality of life. The author says that at present there isn’t any evidence of the worsening of symptoms, but this could be due to a “double hit”, with disease both of the airway and the alveolus and increased susceptibility to exacerbations. Generally speaking, the group of patients with ACO show more symptoms, worse quality of life and higher risk of exacerbations than patients with COPD, but they have better survival13. These findings can be observed in our study, since patients with ACO had higher fre quency of sibilance and of previous diagnosis of asthma and bronchitis.
Both patients with asthma and those with COPD are characterized by acute worsening of respiratory symptoms, and these events have a significant im pact on quality of life and healthcare costs7. Many cohorts compared only patients with asthma or COPD and observed that exacerbations were more frequent in the ACO group, but these observations are not consistent in mild degrees of the disease, and the mechanism explaining this assertion is unknown. In our studies we also observed a signifi cantly higher frequency of exacerbations when com paring patients with ACO with the COPD group.
There is increasing interest in the factors af fecting the disease, including comorbid conditions. Recent studies have shown a higher frequency of comorbid conditions in patients with ACO, but the mechanisms aren’t clear15. In our group of patients, we didn’t observe any increase in comor bidities within the ACO group when compared to the pure COPD group.
There are limitations to our study, some of them correspond to those of the EPOC-AR study. In the population evaluated within the group of patients with ACO there was majority of males, but the dif ference wasn’t significant. This may be due to the fact that most surveyed women stayed at home, especially during daytime schedules, and to their better willingness to carry out the procedures of the study. One specific limitation of this work regarding the Prevalence of the Asthma-COPD Overlap in the EPOC. AR7 study is the fact that we didn’t get the peripheral blood eosinophil concentrationbecause no blood extractions were performed in patients from the EPOC. AR study for any type of test.
CONCLUSIONS
The prevalence of ACO was 19.08% in patients diagnosed with COPD from the EPOC.AR study. Patients who met the diagnostic criteria for ACO where significantly younger, had higher degrees of obstruction, greater use of inhaled corticosteroids, higher frequency of sibilance and exacerbations that required the use of antibiotics. We emphasize the importance of identifying this phenotype that has different and more severe clinical and prog nostic implications, for the purpose of optimizing its management.

