











 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkINTRODUCTION
Tuberculosis is a public health issue, caused by Mycobacterium tuberculosis. The World Health Organization has been publishing reports since 1997 with the purpose of putting an end to tu berculosis (TB) on a worldwide level.1,2 The “End TB” strategy proposes reducing the number of deaths by 95%, and the incidence by 90%, in order to achieve less than 10/100,000 inhabit ants in the 2015-2035 period.3 The Covid-19 pandemic threatens the established programs for TB, since it generated some difficulties in access to healthcare.
Tuberculosis in Argentina is still an important public health issue; in 2019 there was a reported rate of 27.8/100,000 inhabitants, 6.4% higher than in 2018 (26.2/100,000 inhabitants). 78% of new cases were of pulmonary localization.4
Primary tuberculosis develops in patients who haven’t been previously exposed; it is common in pediatric patients, and appears as a consolida tion that affects the middle and lower lobes and adjacent lymph nodes. Lower lung field TB, as referred to in the reference studies, can be seen mainly in people living with HIV, diabetes, renal or liver disease, and those receiving corticoids and diagnosed with silicosis.5-7
This study was conducted for the purpose of describing the epidemiological and radiologi cal characteristics of tuberculous pneumonia in patients without immunosuppression showing consolidation in the lower lung field.
MATERIALS AND METHODS
It is a retrospective (2017-2019 period) and prospective (2019-2021) study that analyzed TB cases treated at the Hospital General de Agudos Parmenio Piñero within said periods. The hospital is located in an area with high prevalence of tuberculosis (>100/100,000 inhabitants). The selection criteria for tuberculous pneumonia were: a) positive bacilloscopy in sputum or bronchoalveolar lavage, or diagnosis of TB with compatible epidemiology and cli nical symptoms, b) not having comorbidities such as HIV, immunosuppression or addictions, c) not being underweight (BMI <18.5), d) chest X-ray with image of consolidation in lower fields.
The medical records of the patients included serological testing for HIV, hepatitis B and C and VDRL (Venereal Di sease Research Laboratory) test, the TB diagnostic method performed and radiographic images.
RESULTS
The analysis included 628 cases of pulmonary tuberculosis, 25 of which (4%) were diagnosed as lower lung field TB. 17 of those 25 cases (68%) were male. The mean age of patients was 33 ± 10 years. Most patients were Argentinian (56%), followed by Bolivians (24%), Peruvians (12%) and Paraguayans (8%). The proportion of females wasn’t significant, compared to males. Table 1 describes the characteristics of patients being evaluated. There is predominance of right lower lobe involvement: 84%. Figures 1 to 4 show examples of the images found.
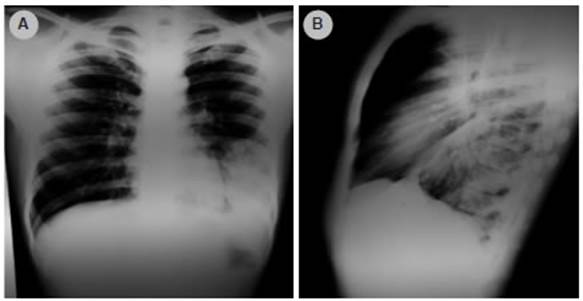
Figure 1 The anteroposterior (AP) and lateral chest X-ray of a 22-year-old man shows homogeneous consolidation at the left lower lobe.
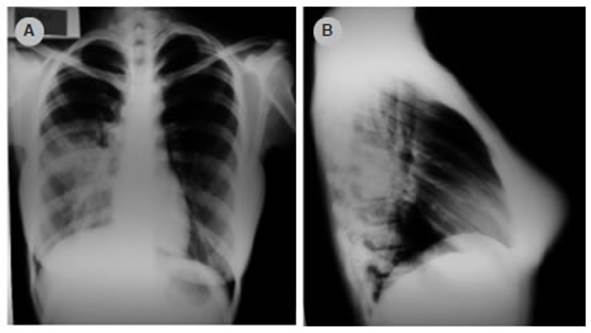
Figure 2 The anteroposterior (AP) and lateral chest X-ray of a 38-year-old woman shows homogeneous consolidation at the left lower lobe.
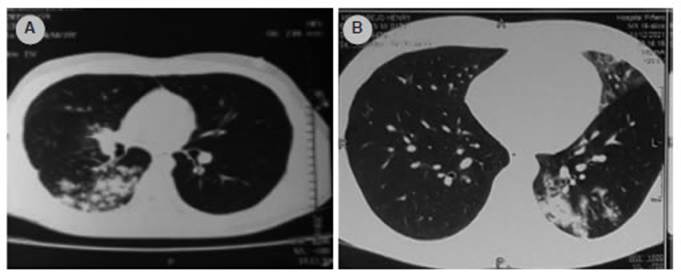
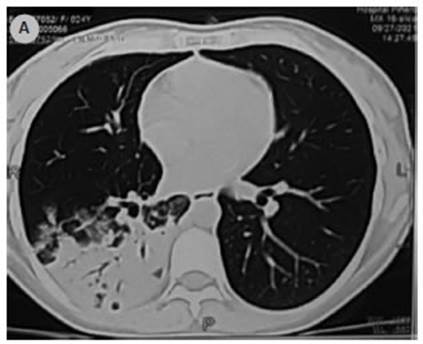
Figure 3 A) Axial tomography of the chest of a 29-year-old woman showing heterogeneous opacities at the superior segment of the right lower lobe. B) Axial tomography of the chest of a 47-year-old man showing heterogeneous opacities at the posterior segment of the left lower lobe.
DISCUSSION
In the group admitted to the study, we identified 4% of patients with lower lung field tuberculosis without associated comorbidities; there were no significant differences regarding sex; and involve ment of the right lung base was predominant in the X-ray.
One of the published studies describing 62% predominance of women suggests the hypothesis that women have intercostal breathing with less diaphragmatic stretching that could result in less ventilation and less expansion of the lower lobes.8 In our case report we didn’t find any differences relating to sex that support such hypothesis.
The observed predominance of the right lung base coincides with what was evidenced in previ ous studies.8,9 In the studies of India (61%) and Taiwan (64%), a predominance of the right lung base involvement was found that was close to the one found by us (84%). The hypothesis that was suggested for this finding is that the main right bronchus is anatomically shorter and has a sharper angle compared to the left bronchus, thus the infectious microorganisms more easily propagate towards the right lower lobe.8-10
Many authors have described that lower lung field TB occurs more frequently in specific groups of patients with diseases without immunosuppres sion.10-11 In agreement with this, some studies in India found that tuberculous pneumonia is more frequent in: diabetes (29%), patients living with HIV (12%), patients receiving treatment with corticosteroids (12%), with liver disease (11%), and with renal disease (5%). On the other hand, we couldn’t find any published studies that describe this form of TB manifestation in groups of patients without comorbidities.8
Lower lung field TB is an atypical presentation of pulmonary TB. The radiographic image similar ity with acute community-acquired pneumonia or even some types of bronchogenic adenocarcinomas entail diagnostic delays.12 One of the proposed explanations is the transbronchial perforation of an affected hilar lymph node, with dissemination to the adjacent parenchyma.13
One limitation of this study is the lack of data identifying the exact time of diagnostic delay of the described group of patients. One strength is the fact of having shown that tuberculous pneumonia occurs even in patients without comorbidities considered as predisposing factors.
To conclude, tuberculosis must be included in the group of differential diagnoses of patients who show consolidation of the lower lung field and have a history of exposure or epidemiological risk, even if they don’t have significant comor bidities or immunosuppression, thus avoiding diagnostic delay.

