










Servicios Personalizados
Revista

Articulo
 texto en
texto en  Español (pdf)
Español (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO
Links relacionados
-
 Similares en
SciELO
Similares en
SciELO
Compartir

 Permalink
PermalinkRevista argentina de cirugía
versión impresa ISSN 2250-639Xversión On-line ISSN 2250-639X
Rev. argent. cir. vol.114 no.2 Cap. Fed. jun. 2022
http://dx.doi.org/10.25132/raac.v114.n2.1564
Articles
Appendiceal diverticulitis as differential diagnosis
1 División Cirugía General, Hospital Militar Central. Buenos Aires. Argentina
The presence of diverticula in the vermiform appendix was described for the first time by Kelynak in 18931. Appendiceal diverticulosis is rare, with a mean incidence of about 1%. The diagnosis is usually incidental in histopathology examinations as the clinical presentation and presumptive diagnosis mimic acute appendicitis (AA).
Appendiceal diverticulitis (AD) is a clinicopathological inflammatory disease that is different from acute appendicitis2, more common in men around the fifth decade of life, and with a higher mortality rate. Diverticula can be classified in 2 main subtypes: true and false. True or congenital diverticula are caused by abnormal bowel permeability, while pseudodiverticula or false diverticula are generated by high pressure and are only made up of mucosa. We report the case of a patient with appendiceal diverticulitis who attended the emergency department of our institution.
A 59-year-old male patient with a history of benign prostatic hyperplasia and coronary artery disease with three bypass grafts visited the emergency department due to abdominal pain with an intensity of 6/10 and sequence of Murphy lasting 12 hours.
The patient was hemodynamically stable and afebrile. The abdomen was tender on deep palpation of the right iliac region with guarding and bowel motility was preserved. He did not complain of gastrointestinal symptoms as anorexia, nausea or vomiting. Laboratory tests: high white cell count 11,800/mm3 (73% of neutrophils). The abdominal ultrasound revealed a partially compressible tubular loop with a diameter of 7.8 mm and a thin band of laminar fluid, consistent with acute appendiceal process.
A diagnosis of right iliac fossa pain syndrome was made and treatment with ampicillin-sulbactam and analgesics was initiated. Surgical treatment was decided3. On exploration, the distal vermiform appendix had signs of inflammation with no evidence of diverticulosis. Conventional appendectomy was performed. The patient had favorable postoperative outcome and was discharge 24 hours later.
The pathology report revealed an appendix with herniated mucosa through the muscular layer and chronic active peripheral inflammation, with extravasation of mucin, and follicular lymphoid aplasia. The diagnosis was appendiceal diverticulitis complicated with rupture and active chronic inflammation (Fig. 1 and 2).

Figure 1 Gross examination (formalin): longitudinal and cross-sectio nal section of the surgical specimen. A thick white wall with hard-elastic consistency is observed, with signs of fibrosis and chronic in flammation (measured in centimeters).
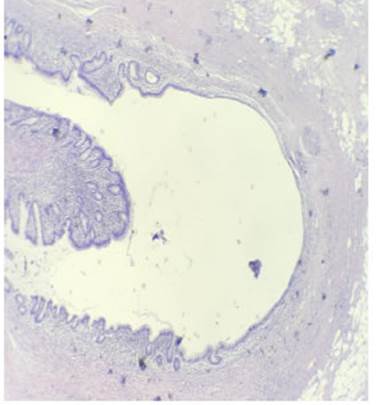
Figure 2 Microscopic examination, magnification x40, hematoxylin and eosin stain: appendiceal wall with herniated mucosa accompanied by mus cularis mucosa.
The patient progress was favorable during outpatient follow-up.
Two months after surgery he underwent video-assisted colonoscopy due to the pathological findings and his age (59 years); the test did not show polyps or lesions suggestive of malignancy.
Appendiceal diverticulitis is usually a postoperative incidental finding at the time of analyzing the surgical specimen and presents signs and symptoms identical to those of acute appendicitis. Although the age of presentation is higher than in acute appendicitis, mean age of presentation is estimated to be 30 years, but it may occur at any age according to the literature3.
Abdominal ultrasound and computed tomography scan can help to make the accurate diagnosis, without modifying the treatment.
According to a review of the literature by Collins et al., the percentage of perforations in surgical specimens is higher in ADs than in AAs (27% and 6.6%, respectively). The risk of appendiceal neoplasm is ten times higher than in patients without appendiceal diverticulitis4.
If AD is evidenced in a surgical exploration, prophylactic appendectomy is recommended to avoid possible complications3. We conclude that appendectomy is the standard of care, due to the higher risk of perforation, the higher mortality rate and the possible association with neoplasms. Appendiceal diverticulitis is most common in young adults and postoperative colonoscopy is recommended, especially if the patient is > 50 years and the appendix is free of tumors5.
Acknowledgments:
We are grateful to the Department of Pathological Anatomy and the Residency in General Surgery of Hospital Militar Central 601, Cir. Mayor Dr. Cosme Argerich for their participation in the clinical work and data collection.
REFERENCES
1. Motos Mico J, Ferrer Márquez M, Berenguel Ibáñez M, Belda Lozanoa R, Moreno Serranoa A. Diverticulitis apendicular: un diagnóstico a tener en cuenta en el abdomen agudo. Cir Espan. 2015;93(6): 49-51. [ Links ]
2. Lobo-Machín I, Delgado-Plasencia L, Hernández-González I, Brito-García A, Burillo-Putze G, Bravo-Gutiérrez A. Diverticulitis apendicular y apendicitis aguda: diferencias y semejanzas. Rev Esp Enferm Dig (Madrid). 2014; 106:452-8. [ Links ]
3. Escobar F, Valentín Vega N, Valbuena E, Barón M. Diverticulitis apendicular, revisión de la literatura científica y presentación de dos casos. Rev Colomb Cir. 2013;28:223-28. [ Links ]
4. Collins DC. Diverticula of the Vermiform Appendix: A study based on thirty cases. Ann Surg. 1936;104(6):1001-12. [ Links ]
5. Singh-Ranger D, Mangalika M. Appendix Diverticula - A Serious Diagnosis: Case Report and Literature Review. Clin Surg. 2018;3:2270. [ Links ]
Received: March 06, 2021; Accepted: May 14, 2021
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
