











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
PermalinkComplicated diaphragmatic hernias (DH) during preg nancy are a life threatening entity. Since first description in 1913 by Muller, it continuous to be an uncommon compli cation during pregnancy and puerperium1. The underlying cause may be a congenital or traumatic diaphragmatic defect in adults who may have gone undetected for many years. During pregnancy, abdominal viscera are displaced within the thorax because of the growth of the uterus. Incarceration and ischemic complication of herniated viscera are some consequences of this displacement2-4. Most cases described in literature occur during the preg nancy period and required an urgent cesarean procedure. In other cases, diagnosis is made at puerperium. Com plicated DH represents a surgical emergency with high morbidity and mortality for mother and baby1,2,5.
Both diagnosis and management of this patient is challenging, and when visceral complication is suspected immediate surgery is indicated. Operative approaches described include laparotomy, thoracotomy, laparoscopic repair or combinations, but we did not find any mention of video-assisted thoracic surgery (VATS). However, VATS may also be an option, alone or in combination with ab dominal procedure, with the advantages of a minimally invasive technique in its recuperation.
We present the case of a woman with a postpartum right sided diaphragmatic hernia, with large bowel ne crosis, that was treated by combination of VATS and laparotomy in the emergency. She had a misdiagnosed diaphragmatic hernia that started to be symptomatic at immediate puerperium and complicated 3 months after the birth of her baby.
Clinical case
A 43-years-old woman admitted to emergency department with complaints of right-side chest and shoulder pain that worsen intensity in the previous 12 hours, associated with nausea and vomiting in the last 3 hours, with no pathology antecedents or trauma history. She had a child 3 months before by natural birth and referred that during puerperium period she started to feel right side shoulder pain. She sought medical advice several times in different emergency departments and analge sics were the only treatment in all cases. At physical exams, she only presented tachycardia and mild tenderness in the upper abdominal region. The emergency department decided to perform a thoraco-abdominal CT instead of conventional x-rays, attending to the medical record of the patient.
CT showed a right sided diaphragmatic hernia with colonic contents in the right hemithorax. Large bowel had signs of distention with a hydro-aerial level inside. It also presented an associated pleural effusion (Fig. 1a-b). As another relevant findings, the laboratory demonstrated white blood cell count of 17 000/ml and mild hypokalemia.
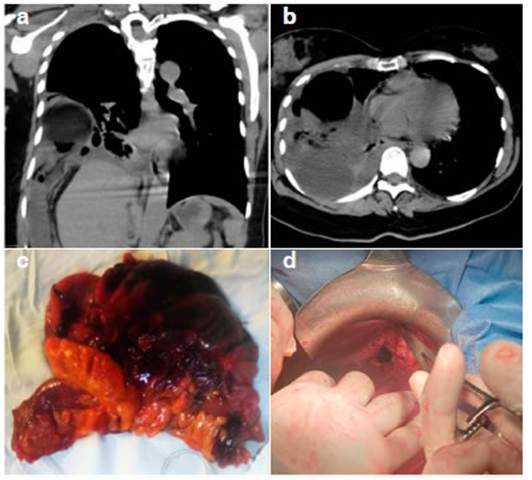
Fig. 1 a) CT coronal image, it can be seen the pedicle and the colonic loop through dia phragmatic ring, b) CT axial image with dilated colonic loop in thoracic cavity and loculated pleural effusion, c) Hemicolectomy surgical piece, d) Ring of diaphragmatic hernia, anterior to the liver
According to the CT findings, we decided on an immediate surgical intervention due to the suspicion of potential perfora tion of the colonic loop. As the patient was clinically stable, we explored the thoracic cavity first. A right-side bi-portal VATS was performed. A 3-4 cm utility incision was made at the 6th intercostal space between anterior and middle axillary line, and a second 10 mm camera port was put at the 9th intercostal in posterior axillary line. An incarcerated colonic hernia with necrosis of the wall was confirmed. VATS allows us to free pulmonary and pleural adhesions without touching colonic wall, then to take samples of serohematic pleural effusion and finally to wash pleural cavity with saline solution. Diaphragmatic ring enlargement was also performed to free incarcerated colonic loop by the use of VATS. No hemodynamic repercussion was verified during selective lung ventilation.
After VATS, an upper midline laparotomy was made. Semi ology of abdominal cavity verified the presence of a right sided diaphragmatic hernia in anterior position (Fig. 1d). The bowel loop was reduced by gently dissection. A right hemicolectomy was necessary because of the necrotic-non perforated colonic wall (Fig. 1c). A two folds handed side to side anastomosis was performed and two latex drainages were left in the cavity. The 5 cm diaphragmatic defect was closed primarily with a non-interrupt 1-0 two folds non absorbable suture.
The patient had a post operatory period without complica tions. Food tolerance and diet started at the 4th day, and institutional discharge was given at day 7th. Four months later, she is in good health.
Discussion
Diaphragmatic hernias complicating pregnancy and postpartum are not a common problem. A 2018 review by Reddy et al6 described 56 cases in which only 13% of them were right sided diaphragmatic hernia, while a 20% were presented during labor or postpartum. Diaphragmatic hernias are classified as congenital, traumatic or hiatus1,3. Their etiology in pregnancy or postpartum may be diffi cult to certify, although a postero-lateral defect supports congenital origin and a traumatic history orients to an acquired hernia as possible diagnostics1. However, there is an important number of hernias without relevant data for diagnostic. Consistent with this, Chen et al.3 described a 30% of unknown etiology in their review. This is the case of our patient who did not refer any relevant antecedent that could classify her hernia etiology.
Not only diagnostic is difficult, but also treatment. Most patients require urgent surgery during pregnancy and it represents a life-threatening condition for both mother and baby. Uncomplicated DH cases that are diagnosed during the postpartum period must be treated prior to a new pregnancy in order to avoid future com plications3,7.
There are several surgical access being laparotomy the most commonly used. Other approaches like lapa roscopy or combinations like laparotomy/laparoscopy with thoracotomy have also been described. Minimally invasive techniques have well known benefits that may have an impact on postoperative. However, laparoscopic repair represents approximately 1% of repairs performed8. Even more, we could not find in our searching descriptions of VATS use to treat this condition in the emergency. Julien et al9, in their case report exposed the benefits of lateral decubitus and minimally invasive technique to treat a right diaphragmatic hernia. They also mentioned the possibil ity of using thoracoscopy if necessary, although they did not performed a thoracic procedure in their patient. VATS allows us to free adhesions, the aggressive wash of the pleural cavity and also hernia repair if it is possible with a better postoperative recovery. In our case, we did not treat hernia ring because of the high risk of perforation due to necrotic wall of the organ.
As we describe here, VATS and their variants (con ventional, bi-portal or mono-portal) could be an option to board these patients. When VATS is performed first as a combined access, it could allow better manipulation of ischemic or necrotic organs with minimum risk of rupture during hernia reduction, avoiding thoracic contamination. In our case, we first decided to performed a bi-portal VATS and liberate all colonic adhesions without touching the necrotic viscera, then take samples of pleural fluid, wash pleural cavity and finally enlarge hernial ring for a better reduction through the laparotomy access.
In conclusion, VATS could be an option instead of tho racotomy to treated thoracic cavity in the management of complicated diaphragmatic hernias during pregnancy and puerperium. VATS has shown to be a secure procedure in trained hands, with well-established benefits against thoracotomy. With time, more examples of minimally in vasive techniques to manage this pathology might arise and VATS could become a standard approach for these patients.

