











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
PermalinkKEY POINTS
Current knowledge
• The prevalence of strong myopia in Argentina is very low in adults, but there are no studies of visual impairment due to this condition.
Article contribution to current knowledge
• The study of the issuance of Certificates of Visual Dis ability of the City of Buenos Aires showed that strong myopia is the main cause of visual disability in working age.
Public health policies, such as planning of specific prevention programs, defining the national budget and developing health services, need epidemiological data on the causes of visual impairment and blindness1-5. Cataract, macular degeneration, glaucoma, diabetic retinopathy, trachoma, and uncorrected refractive errors have been identified as the most prevalent causes of legal blindness and vision impairment worldwide1,6-9. Most studies have focused on one population within a circumscribed region, but differences among ethnic groups, environmental fac tors, demographic parameters and lifestyle can affect the prevalence and causes of vision loss.
Argentina has been a country of immigration since the time of the colony. Buenos Aires city is an extended devel oped urban environment of ∼ 3 million people with different ethnic origins and varied family incomes or lifestyles. Most inhabitants are of Italian, Spanish, and German descent as European immigration after year 1880 doubled the original colonial population in few decades. In addition, there are many collectivities, as French, British, Jewish, Ukrainians, Arabs, Japanese or Chinese, among others, and a minority of old Creoles who date back to the Spanish colonial days. The Creole and Spanish-Aboriginal (mixed) population in the city has recently increased as a result of immigration from inner provinces and South American Spanish speaking bordering countries such as Bolivia, Paraguay, Chile, and Peru during the second half of the 20th century. In this context, the demographic complexity of Buenos Aires City inhabitants makes it an interesting scenario to analyze the causes of visual impairment in a mixed affluent population of Latin America. Such analysis could serve as basis for the region, where this type of study has not been yet performed to our knowledge.
Besides, epidemiological data about the prevalence and causes of low vision and blindness in Argentina in general, and in Buenos Aires City in particular, are scarce. The prevalence of blindness in Buenos Aires Province has been reported as 1.1% in people older than 50 years of age, with treatable cataract being the main cause of this vision impairment7. Moreover, a high prevalence of blind ness resulting from cataract was shown in the north-west district of Buenos Aires Province10 and in a representative cross-sectional population study in Argentina11. Cataract is a preventable cause of vision impairment, but data on the prevalence of age-related macular degeneration (ARMD), glaucoma, diabetic retinopathy, and other major causes of visual disability in Argentina are not yet available.
There is only one institution in Buenos Aires City au thorized to grant a personal visual impairment certificate (Santa Lucía Ophthalmologic Municipal Hospital). Since these certificates offer several benefits, such as a monthly pension, transport or tax discount, and 100% coverage for all medications and treatment costs, most individuals with visual disabilities in the City of Buenos Aires apply. The law 24.901 for this certificate was promulgated in 1997 but it was not until the years 2000 that people began to be aware of its importance and associated benefits. The aim of this study was to identify the main causes of legal blindness in Buenos Aires City. These data were obtained from the database of ocular disability certificates issued by the Santa Lucía Hospital between 2009 and 2018.
Materials and methods
In Argentina, visual disability is defined as a visual acuity ≤ 20/200 or a corresponding visual field of less than 20 de grees in the less impaired eye. A certificate of visual disability is issued by the Ministry of Health of Buenos Aires City for all individuals who meet the above definition. The procedure consists of a complete eye examination by an ophthalmologist, including best corrected visual acuity testing, visual field test ing and a complete ophthalmologic examination with Goldman tonometry, anterior segment biomicroscopy under slit-lamp and fundus evaluation after pupil dilation. The ophthalmologists sent eligible patients to the certification process which was carried out at Santa Lucía Hospital. Patients were re-examined by an Evaluation Committee. If the diagnosis was confirmed, each patient received the certificate using the 10th revision of the International Classification of Disease (ICD-10) to codify the cause of visual disability.
All the information of the emitted visual disability certificates gathered between years 2009 to 2017 was comprehensively collected in a dataset. The database included the following variables: name, ID number, year of issue of the certificate, age, gender and major cause of visual disability (ICD-10 classification system). An independent investigator built an excel database replacing each patient´s name, surname and ID number by correlative numbers to provide the research team with a new excel database, so that none of the patients could be identified during the analysis, according to the ethi cal recommendations. All data were maintained confidential in accordance to the Declaration of Helsinki. The present study was approved by the Institutional’s Review Board of the Santa Lucía Hospital and by the Santa Lucía Hospital Ethics Com mitte (Register Code 2645).
The relative prevalence of each cause of visual disability was studied by age and gender, and presented as relative percentage of the studied sample. Chi Square tests were used for finding differences in these prevalences for each individual disease. The R Project for Statistical Computing Sofware (ver sion 3.2.0) and SPSS version 15 (SPSS, USA) were used to perform the statistical analysis. Age, time (in years), gender and the interaction between each independent variable were included in the analysis. Differences were considered statisti cally significant with p < 0.05.
Results
In nine years-time (2009 to 2017) a total of 7656 subjects were certified as legally blind by the Hospital Santa Lucía in the city of Buenos Aires. The mean age of the sample was 57 ± 21 years (range from newborns to 101 years) and 52.1% were females. The emission was near 700 certificates per year. The age distribution of the sample showed that 62.8% of certificates were from patients older than 50 years and that only 6.6% were given to subjects under 20.
In all, visual disability was classified in 286 different diagnoses according to the ICD10 classification system. The distribution of the 50 principal causes of visual dis ability certificates issued during the study period is shown in Table 1, with 7022 subjects (91.7% of the sample). The leading causes of visual disability in Buenos Aires City were age-related macular degeneration (ARMD) with a rate of 15.5% (n = 1186), degenerative myopia (14.4%, n = 1104), primary open-angle glaucoma (11.3%, n = 865) and diabetic retinopathy (6.6%, n = 504). Phthisis bulbi, although reached 6.8% (n = 522) prevalence of certifi cates, is not a true disease but the final stage of many different diseases, so it was not included among the principal diseases.

The analysis of the five main diseases of visual disabil ity along age of the sample is shown in Figure 1 (ARMD, primary open angle glaucoma, degenerative myopia, diabetic retinopathy and hereditary retinal dystrophies). It can be seen that degenerative myopia, diabetic reti nopathy and hereditary retinal dystrophies are producing disability in the middle working ages, while glaucoma and ARMD produce disability later in life. There was no clear tendency of these diseases to change their relative preva lence along the time of the study except for an increase in recent years of the relative prevalence of ARMD (Pearson 0.833, p = 0.005) (Table 2).

Fig. 1 Distribution of number of subjects for each of the principal diseases along ages. In this cross-sectional data it can be seen that degenerative myopia and diabetes peak at ages 50-60, age-related macular degeneration (ARMD) and glaucoma peak at older ages, and hereditary retinal dystrophies are distributed evenly across all ages
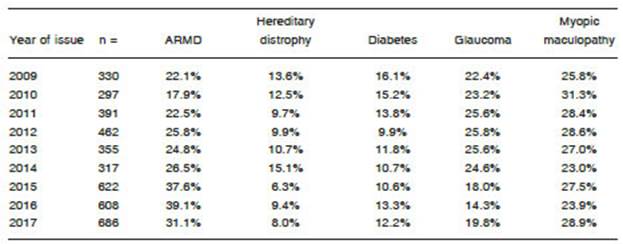
Table 2 Relative percentages of the five principal diagnosis according to year of issue (n = 4068 subjects)
Degenerative myopia was the leading cause of dis ability in subjects younger than 50, while ARMD was the leading cause in those older than 50 (Fig. 2).

Discussion
Worldwide studies about vision impairment began by the end of the 90s1 and after their data were available, many countries began to implement laws for emitting visual disability certificates, social security benefits and reha bilitation programs for the affected people. Uncorrected refractive errors and cataract are the leading causes of vision impairment worldwide and are generally not considered for emitting permanent disability certificates because these diseases can be treated. The present study is interesting in the sense that shows the causes of visual disability certificate emissions, and few previous studies of this kind could be found. One was performed in Israel12,13, other in England and Wales14, a third in Ireland15 and a fourth in China16. The records of the Israeli study from 1998 to 2008 showed that for a country population of 7 million, 19 862 newly certificates of vision disability were emit ted in 10 years (2.8‰) while in Buenos Aires there were 7656 in 3 million inhabitants (2.5‰). The five principal causes of disability in the Israeli study, in 2008, were AMD (28.7%), diabetic retinopathy (13.2%), glaucoma (12.1%), cataract (5.1%) and retinitis pigmentosa (7.8%), leaving 46.0% for other causes in which probably degenerative myopia was included12,13,17. The England and Wales study (1999) involved 13 723 blind subjects with certificates and here again degenerative myopia was not reported14 but when the study was repeated in 2010 then degenerative myopia was informed at a rate of 2.8% in working age population (16-64 years)18. Interestingly, the Irish study also reported on visual disability in the working population (16-64 years) showing that hereditary dystrophies (reti nitis pigmentosa + albinism) had a relative prevalence in certificates of 23.4%, myopia 6.6%, glaucoma 6.0% and diabetes 3.5% (this was in 1998, before the epidemics of myopia in East and South East Asia). A very recent visual disability certificates study in Shanghai (Jing-An District)16 showed that the relative prevalence of vision impairment due to myopic maculopathy increased from 14.5% in 2001 to 26.1% in 2007, when it became the leading cause of vision disability. A study in 1989 performed in Australian Royal Blind Society showed ARMD and glaucoma were the leading causes of certificate emission, but here again myopia was reported among other diagnosis19.
In general terms, the most prevalent causes of visual impairment identified in this study were ARMD and de generative myopia (both near 15%). The high prevalence of degenerative myopia is interesting in the context that Buenos Aires City, as previously described by Cortinez et al.,20 has 2.3% prevalence of high myopia (greater than -5.00 diopters, prone to myopic maculopathy) in an unselected sample of highly educated office workers. Pathologic myopia is an important cause of vision loss worldwide, affecting up to 3% of the population21. Studies performed in China and Japan found that pathologic myo pia was the cause of blindness or low vision in 12.2-27.4% of individuals with visual impairment22-24, while The Los Angeles Latino Eye Study reported that pathologic myopia was the cause of blindness or low vision in 4.5% of Latin American residents in Los Angeles25. A survey performed in Australia, clearly showed the exponential increase of vision loss with increasing age and supports the impact that increased ageing of the population will have on the number of people with vision loss and blindness9. Interestingly, degenerative myopia was there the second leading cause of disability at all ages, and by much the leading cause of disability in people younger than 50. High myo pia usually has early onset between 6-10 years of age in early school years, and when detected can undergo treatment to prevent progression up to high myopia in the next five years (if the children progress at a rate of -1.00 diopters per year, as is usually seen). The most effective treatment today is the instillation of diluted atropine drops in a regular annual basis26-29. It is important that pediatric and general ophthalmologists refracting schoolchildren be aware that the disease progression can be limited, as high myopia and its macular complications have been now shown to be major causes of vision impairment at early adult ages.
The principal study limitation is the cross-sectional design but as certificates are emitted for a period of 10 years-time, we can be sure that no subject was dupli cated. Other concern could be the lack of evidence that this sample is population based, representing the vision impairment prevalence in Buenos Aires. In this sense, as medical coverage for rehabilitation of vision impairment covers treatment costs and low vision visual aids only for those with visual disability certificates, and ophthalmolo gists in Argentina are encouraged to send patients to vi sion rehabilitation, we then argue that most vision impaired subjects are possibly included in this centralized database.
Interestingly, degenerative myopia was the second leading cause of disability at all ages, and by much the leading cause of disability in people younger than 50. Thus, in Buenos Aires, where the prevalence of high myopia has been shown to be low, degenerative myopia was found to be the major cause of visual disability in younger subjects. The reason for that is not clear and should be further studied. Moreover, recently introduced methods to control the progression of myopia and high myopia28, should be actively propagated in Argentina to prevent this vision disability. The treatment of early onset cases of myopia in primary school years, the ones that are prone to develop myopic maculopathy, could arrest their progression and avoid that disability. As prevention programs would show results after long time when these children have grown up to adulthood, urgent preventive programs are needed.

