











 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
PermalinkKEY POINTS
• There was no evidence correlating a greater number of administered antiepileptic drugs and higher mortality rates. Patients who were administered anesthetic drugs died after 21 days, whereas those who were not, died after 60 days. These results presume the high mortality rate associated with anesthetic drugs, regardless of the number of anticonvulsant drugs previously administered.
Current knowledge
• One third of patients are refractory to benzodiazepines and treatment at next stage is still being discussed. There is no Class I evidence to favor one drug over another.
• When SE becomes Refractory and Super- Refractory, controversy surrounding the treatment is even greater and intravenous anesthetic drugs have been recommended.
Contribution of the article to current knowledge
• With these results could be presume the high mortality rate can be associate with anesthetic drugs, regardless of the number of anticonvulsant drugs previously administered.
Status epilepticus (SE) is a neurological emer gency with an estimated incidence of 60 cases per 100 000 per year and a 20% mortality rate around the world.
“SE health-care cost in refractory stages is high1, and a German study has estimated a cost of €1.365 a day”2.
The concept “Time is brain” applies to SE, which has been reported to worsen when it is prolonged. Early and appropriate treatment is associated with lower morbidity and mortality rates and a lower number of administered drugs. This results in a shorter hospital stays and lower health-care costs.
SE represents approximately 3.5% of ICU (in tensive care unit) patients and 15% of neurology department inpatients3.
In Argentina, its adjusted annual incidence was 24.3 cases per 100 000 per year, in 20133.
Non-Convulsive Status Epilepticus (NCSE) has a 10% global incidence in patients with impaired awareness and a 16% incidence on elderly pa tients upon admission4. Patients with a history of epilepsy, elderly or septic patients are at high er risk of developing NCSE.
It has been demonstrated that NCSE patients’ condition is more likely to deteriorate when the episode durations prolonged or due to systemic complications. However, etiology is the most in fluential factor to develop NCSE.
The ILAE (International League Against Epilep sy) defines SE as “a condition resulting either from the failure of the mechanisms responsible for seizure termination or from the initiation of mechanisms which lead to abnormally pro longed seizures (after time point t1). It is a con dition that can have long-term consequences (after time point t2), including neuronal death, neuronal injury, and alteration of neuronal net works, depending on the type and duration of seizures”5.
Time point t1 determines the time when the seizure is considered to be abnormally prolonged and when the treatment should be started. Time point t2 determines the time beyond which ic tal activity is considered to be a risk and deter mines how aggressive the treatment should be.
Some types of SE can only be diagnosed by EEG monitoring because motor clinical symptoms are usually absent or very subtle; sometimes the only symptom is the impaired awareness.
Therefore, differentiating SE with predomi nantly motor symptoms (Convulsive SE) and SE without symptoms (Non-Convulsive SE) it been proposed7,8.
Ictal patterns shown in the EEG are not spe cific, and they have limited clinical value in con vulsive SE due to overloading movement and muscle artifice. However, EEG monitoring is es sential to diagnose NCSE because clinical signs may be very subtle or even nonexistent.
As it was mentioned above, NCSE diagnosis sometimes is not straight forward, so it is essen tial to perform an EEG. Hence, in 2013, the Salz burg criteria were proposed to diagnose NCSE. These criteria have a 97.7% sensitivity, 89.6% specificity. Therefore, the diagnosis is 92.5% ac curate7-9.
The ILAE describes a staged treatment10,11. Initially it must be with benzodiazepines. Sever al studies have demonstrated benzodiazepines efficacy and safety. Up to two thirds of cases are successfully controlled in this early stage. Mid azolam efficacy is 73.4% while lorazepam effi cacy is 63.4%12.
Around 30-40% of patients go into Stage II: Established SE (refractory to benzodiazepines). Treatment in Stage II is still being discussed. Administration of antiepileptic drugs (AEDs) like phenytoin (PHT), valproic acid (VPA), leveti racetam (LEV), phenobarbital (PB) or lacosamide (LCM) is recommended. There is no Class I evi dence to favor one drug over another. The effi cacy of these drugs to control SE has been tested in cohort and case and control trial studies for years13,14. VPA has been proved to have an effi cacy rate of 70-76%; PB, 73-80% (although with a high rate of respiratory depression); LEV, 50-70%; PHT, 50-58% (with several cardiovascular secondary effects and respiratory depression); LCM, 56%15-21. Currently, perampanel (PER) or brivar acetam (BVT) are being studied in order to prove their efficacy to control seizures. So far there is little reliable literature22-25.
As to stages III and IV, when SE becomes Refractory (RSE) and Super-Refractory (SRSE), controversy surrounding the treatment is even greater26. For years, and even today, intravenous anesthetic drugs (IVADs) like propofol, midazol am, thiopental or pentobarbital had been rec ommended.
Several studies had shown that using IVADs is associated with higher infection rates (11% vs. 43%), a 2.9-fold death risk increase, a high rate of cardiovascular complications and severe im munosuppression27-31.
In order to assess SE outcome and mortality rate, two scores had been proposed32. EMSE (Ep idemiology-based Mortality Score in Status Epilepticus, cutoff value of ≥ 34) and STESS (Status Epilepticus Severity Score, cutoff value of ≥ 3) can predict short-term mortality with high sensitiv ity and specificity. The worst outcomes were as sociated with the following factors: old age (≥ 65), New Onset Refractory Status Epilepticus (NORSE), NCSE, the impaired consciousness at the onset of the episode, the duration of the seizures, comor bidities, etiology, EEG features, infections, respi ratory failure, or cardiovascular failure15,30-38.
NCSE has a high morbidity-mortality rate be cause it does not present evident motor clinical signs. Sometimes the diagnosis, and therefore, appropriate treatment, can be delay.
In the last few years, several studies had shown that certain drugs are more effective than others to treat NCSE. Also, some drugs can have potential secondary effects that increase mortality rates.
We proposed to study NCSE management, establishing the therapy provided in our health-care center and the patients evolution, compar ing with the available literature.
The main objective is to assess the use of an tiepileptic and anesthetic drugs in relation to NCSE mortality rate in the ICU.
A secondary objective is to assess the correla tion between the pharmacological treatment in NCSE patients in the ICU and how they had re sponded. This was observed in the clinical signs and symptoms and in the EEG. The values of ST ESS and EMSE were correlated with the patients’ clinical and EEG evolution.
We presumed that mortality rate of NCSE patients in the ICU correlates with the chosen therapy.
Material and methods
Study design
An observational, descriptive, cross-sectional study was performed. Data was collected and analyzed from the time of admission to the time of discharge or decease.
The reviewed data was collected from the Buenos Aires British Hospital clinical records and neurology de partment database from January 2018 to June 2021.
STESS and EMSE scores were applied to determine mortality risk.
The primary research question was to establish the mortality rate correlating to the scores values and the ad ministered drugs.
Participants
Ninety (90) patients over 18 years-old, diagnosed with NCSE and fulfilling Salzburg criteria were included. Pa tients with post-anoxic encephalopathy (NCSE after cardiac-respiratory arrest) and/or insufficient data were excluded.
Variables
The variables included were sex, age, history of epi lepsy, comorbidities, level of consciousness upon ad mission, worst type of epileptic seizures, etiology, EEG pattern (at onset and after treatment), antiepileptic drugs administered (loading and maintenance dose) and outcome (hospital discharge or decease). The Apache II score was applied to avoid potential confounders and bias sources.
Statistical Analysis
Basic descriptive statistics were used and the confi dence interval was estimated at 95%, with a value of p < 0.05 as statistically significant. An age-adjusted, univa riate and multivariate analysis was performed. The cu toff values stablished were ESME ≥ 34 points, STESS ≥ 4 points and Apache-II ≥ 31. STATA 17 statistical software was used. X2 test was performed with the dichotomous data. All patients with missing data were excluded from the study.
Results
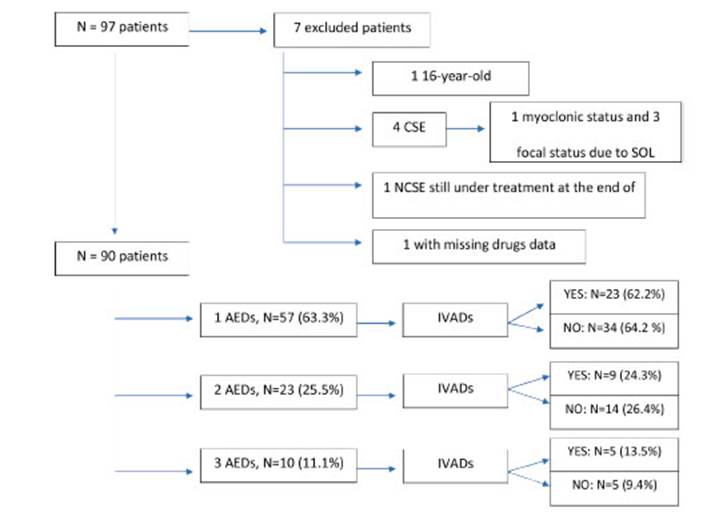
We enrolled 97 patients with SE at the Buenos Aires British Hospital from January 1st 2018 to June 30th 2021. Seven (7) patients were excluded because of the following causes: a 16-year-old patient; 4 patients with Convulsive SE (1 with myoclonic status and 3 with focal status due to a space-oc cupying lesion); one patient diagnosed with NCSE but still hospitalized at the end of trial; a patient with missing data, thus hindering assessment of pharmacological treatment and its results (Fig. 1).
Demographic data, clinical features and phar macological comparisons can be observed in Table 1.
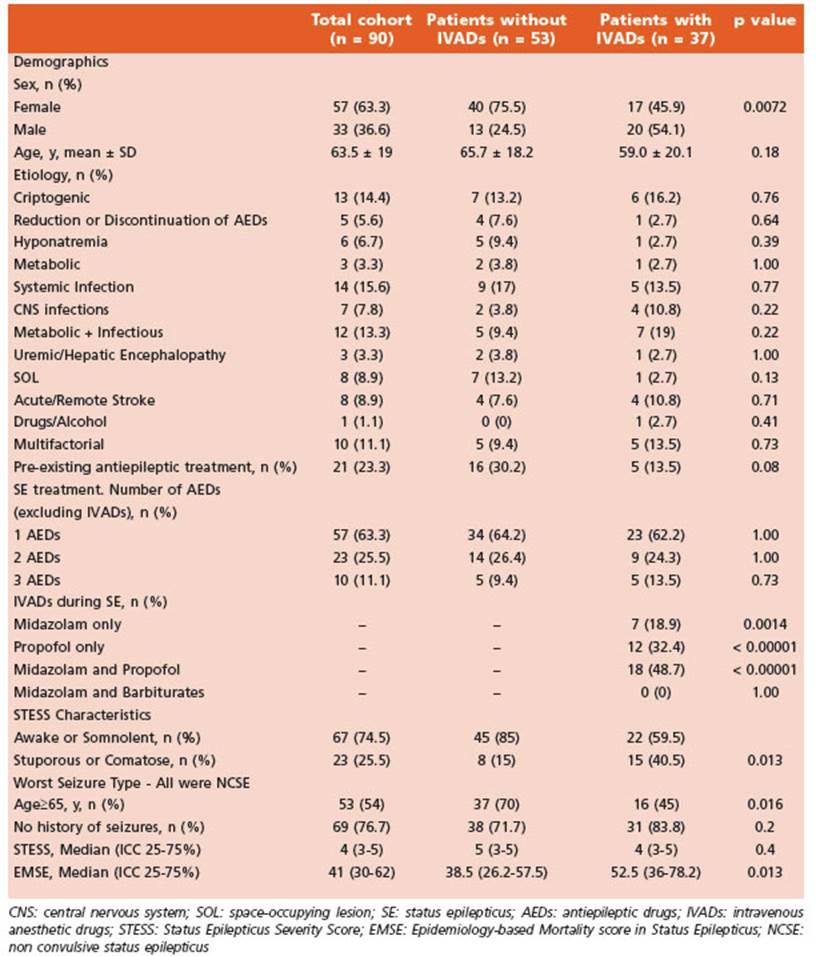
Tabla 1 Demographic and clinical features of patients with and without continuous IV anesthetic drugs treatment
A univariate and multivariate statistical anal ysis was performed on a total of 90 subjects. Fifty-seven (57) were females (63.3%). The mean age was 63.5 years-old (SD ± 19). Thirty-seven-point eight percent (37.8%) of patients died dur ing hospital stay (34/90).
Seventy-nine (79) out of 90 patients were re ported with generalized NCSE (13.3% after a con vulsive SE evolved [12/90]), with a 34.4% death rate (31/79).
As to STESS values, 12.2% of the 90 patients (11/90) had a score between 0-2 and all were dis charged; 41.1% (37/90) had a score between 3-4, where 16 died (43.2%); 46.7% (42/90) had a score between 5-6, where 17 died (40.5%).
As to EMSE values, 27 of the 90 patients (30%) had a score of < 34 and a 7.4% death rate (2/27), while 63 of patients (70%) with a score ≥ 34 had a 50.8% death rate (32/63).
Out of the 90 patients, 37 (41.1%) were ad ministered anesthetic drugs. Twenty-nine (29) of them (78.4%) had an EMSE value of ≥ 34, out of which 20 (69%) died at the hospital. Seventy-nine of the total sample (87.8%) had a STESS val ue of ≥ 3, out of which 34 (43%) died.
Out of the 90 patients, 53 were not adminis tered anesthetic drugs (58.9%). Thirty-four of them (64.2%) had an EMSE value of ≥ 34, out of which 12 (35.3%) died at the hospital. Forty-five of them (84.9%) had a STESS value of ≥ 3, out of which 13 (28.9%) died.
It is worth highlighting the finding that pa tients who were administered anesthetic drugs were younger (< 65 years-old). This data was statistically significant (p 0.016).
No significant differences were found be tween EMSE (Fig. 2) and STESS (Fig. 3) values cor relating to the number of administered AEDs.
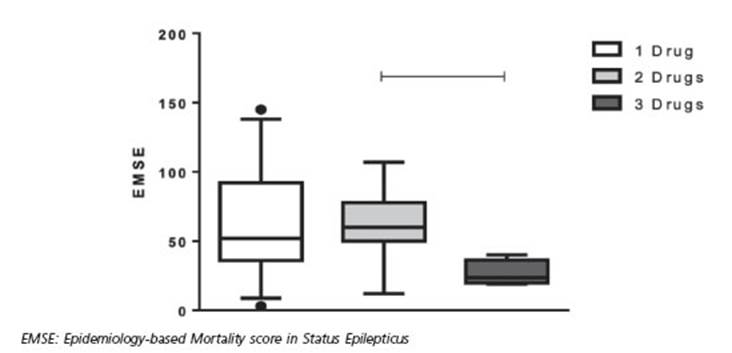
Figura 2 Epidemiology-based Mortality Score in Status Epilepticus and number of antiepileptic drugs administered. No statistically significant differences were found
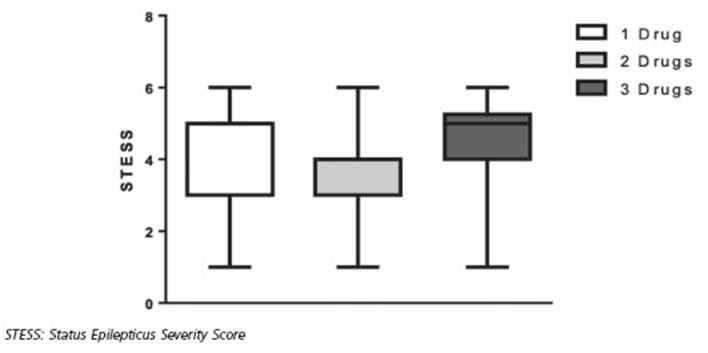
Figura 3 Status Epilepticus Severity Score and number of antiepileptic drugs administered. No statistically significant differences were found
Treatment and outcome: use of antiepileptic drugs and anesthetics
No significant differences were found on sur vival rates correlating to the number antiepilep tic drugs: 1 drug, OR 1.255, 95% CI 0.42-3.75; 2 drugs, OR 0.669, 95% CI 0.2-2.2; 3 drugs, OR 1.38, 95% CI 0.23-8.3 (Fig. 4). This suggests that using 3 anticonvulsant drugs does not increase death risk.
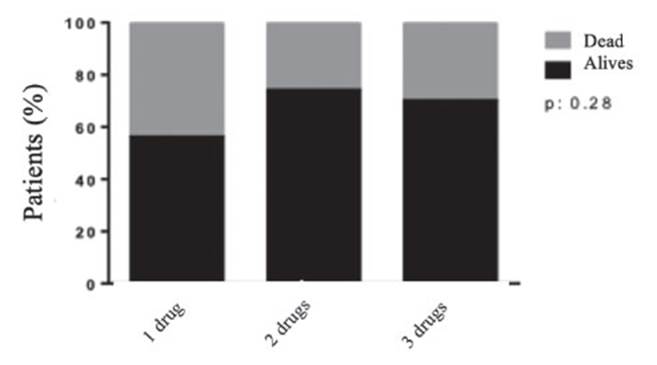
Figura 4 Correlation between number of administered antiepileptic drugs and survival. No significant differences were found on survival rates correlating to the number anticonvulsant drugs regardless of age and Status Epilepticus Severity Score or Epidemiology-based Mortality score in Status Epilepticus values. Using 3 anticonvulsant drugs does not increase death risk
Fifty-three out of 90 (58.9%) of patients were not administered anesthetic drugs and 24.5% of them died (13/53). Among patients who were administered anesthetic drugs (37/90 [41.1%]), 56.8% died (21/37).
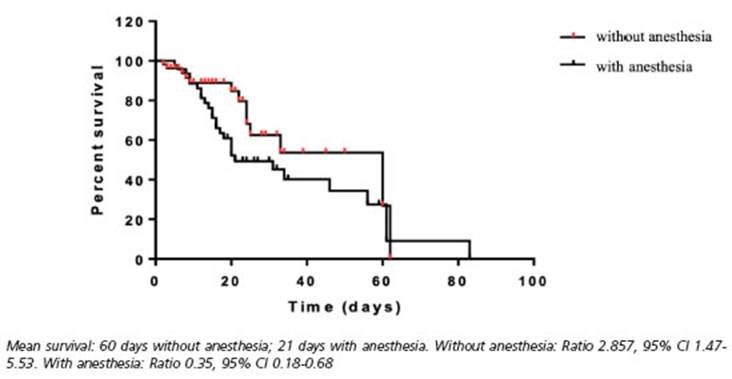
Upon performing a multivariate analysis, pa tients who were administered anesthetic drugs died after 21 days, while those who were not, died after 60 days (Fig. 5). It could be presumed that using anesthetic drugs carries a 2.61-fold death rate increase (95% CI 1.001-6.83). Even thought, more studies must be performed to confirm this association. The analyzed data would not be enough to confirm this hypothesis.
Discussion
SE is known to have a high morbidity-mortal ity rate globally. For years, benzodiazepines have been known to be the most effective treatment for Early SE (Stage I). However, there is insuf ficient Class I evidence to favor one drug over another for Established SE (Stage II) treatment. In our health-care center, the main antiepileptic drug used was levetiracetam, probably due to the lack of available endovenous drugs in our hospital. Phenytoin it is rarely used due to its associated high cardiologic secondary effects rate, high toxicity and narrow therapeutic win dow.
Some literature reports a 3-fold death rate in crease with the use of anesthetic drugs in Re fractory and Super-Refractory SE39. It had been reported an increase of infections, longer ICU stays and greater vasoactive drugs requirement rates. Despite this data, ICUs continue using an esthetic drugs40. We had observed a 56.8% (21/37) death rate in patients who were administered anesthetic drugs and a 24.5% (13/53) death rate in patients who were not. We presumed anes thetic drugs could cause a 2.6-fold death rate in crease. Death rate was lower (30% [3/10]) in pa tients who were administered 3 anticonvulsant drugs (10/90), compared to those who were ad ministered anesthetic drugs (37/90-41.1%) (mor tality rate 21/37-56.8%). Mortality was an inde pendent and statistically significant variable.
It is also worth highlighting that death rate was higher (50.8% [32/63]) among patients with ESME ≥ 34 compared to those with a lower score (7.4% [2/27]).
As to STESS, some papers use a cutoff value of ≥ 3 and others a cutoff value of ≥ 4. In this study, a higher mortality rate was observed with a cut off value of ≥ 3. With STESS 0-2, a 0% mortality rate was observed. With STESS ≥ 3, the patients had a 43% (34/79) mortality rate.
Due to the scarcity of literature on mortality rates associated with anesthetic drugs use in NCSE management, the number of subjects re quired for this kind of study to be significant has not been defined. Therefore, we cannot assess whether the number of subjects meets the re quirement. Further studies with a greater num ber of subjects are warranted to conduct a better analysis.
There was no evidence correlating a greater number of administered antiepileptic drugs and higher mortality rates. Patients who were admin istered anesthetic drugs died after 21 days, where as those who were not, died after 60 days. These results shown the high mortality rate associated with anesthetic drugs, regardless of the number of antiepileptic drugs previously administered.
Furthermore, it has been established that it is important to use EMSE and STESS scores to predict mortality with a cutoff value of ≥ 34 and ≥ 3, respectively. Other important predictive fac tors are the EEG pattern after treatment, the pa tients’ age and their history of epilepsy.
Further studies similar to ours, with a great er number of subjects, may revolutionize and modify the proposed and chosen therapy for NCSE in Refractory and Super-Refractory Stages, thus modifying patients’ survival rates.
Study limitations: The management protocol in the ICU was unclear. The choice between an tiepileptic and/or anesthetic drugs was not pre-determined or reported. Furthermore, many pa tients were not administered benzodiazepines as a first line treatment.
Patients with equal EMSE, STESS and Apache II values were treated with either more than one antiepileptic drug or with anesthetic drugs, without following a management protocol. This presume that the clinical condition of patients does not modify their survival.

