











 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
PermalinkWe report the case of a 20-year-old female patient with a diagnosis of mixed connective tissue disease in 2018 but no follow-up for the last 18 months, and with Hashimoto's thyroiditis and bronchiectasis. The patient went to the Outpatient Emergency Room for abdominal pain, nausea and diarrhea. Signs of right heart failure (edema of the lower limbs, jugular venous distention without inspiratory collapse, positive hepatojugular reflux and enlarged liver), increased intensity of the second heart sound at the expense of the pulmonic component, and systolic murmur in the tricuspid focus were detected on admission. Initial diagnostic tests included an ECG showing signs of overload of the right chambers and complete right bundle branch block, and a chest X-ray with enlarged second right pulmonary arch and normal cardiothoracic ratio. Doppler echocardiography revealed enlargement of the right chambers, severe right ventricular dysfunction, severe tricuspid regurgitation with peak regurgitation velocity > 4.5 meters per second (m/s), pulmonary artery systolic pressure (PSP) 105 mmHg, mean pulmonary artery pressure (mPAP) 55 mm Hg, and mild pericardial effusion (Figure 1).
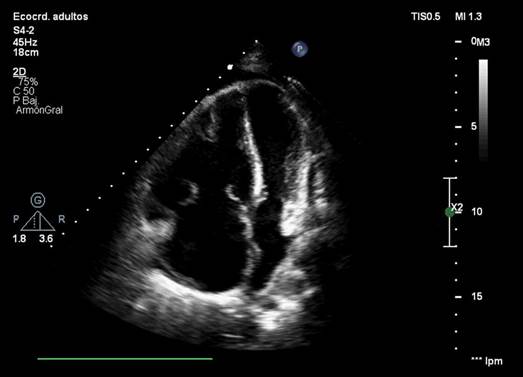
Fig. 1 Doppler echocardiography. Apical 4-chamber view showing marked enlargement of the right chambers, displacement of the ventricular septum, reduction in left ventricular diameter, and severe tricuspid regurgitation.
Right heart catheterization confirmed the diagnosis of severe pulmonary arterial hypertension (PAH) with mean right atrial pressure 11 mmHg, mPAP 63 mmHg, pulmonary wedge pressure 10 mmHg, pulmonary vascular resistance (PVR) 21 Wood units (WU), transpulmonary and diastolic gradients of 53 mmHg and 43 mmHg respectively, cardiac output (CO) 3.20 L/min, cardiac index (CI) 2.6 L/min/m2, systolic volume index (SVI) 23 ml/beats/m2, mixed venous saturation 65%, and arterial saturation 97%. Due to marked right ventricular failure, the patient was started on continuous intravenous infusion of furosemide with no positive response, inotropic support with high-dose milrinone that was later switched to levosimendan 0.1 ug/kg/ min, and vasopressor support with intermediate doses of noradrenaline. The patient progressed unfavorably, with low cardiac output and severe right ventricular failure. Given that immediate access to parenteral prostanoids was not possible, transseptal balloon septostomy was performed (5 mm fenestration) successfully (Figure 2). The patient's clinical condition improved, with early referral to a tertiary care center for pre-transplant evaluation and continuous intravenous epoprostenol infusion -increasing doses up to 12 ng/kg/min- after weaning and discontinuation of inotropic drugs, and administration of ambrisentan 10 mg and tadalafil 10 mg, which were well tolerated. Follow-up Doppler echocardiography showed moderate enlargement of the right chambers, PSP 70 mmHg, and 0.9 mm loss of atrial septal continuity (Figure 3). Cardiac catheterization showed decreased mPAP and PVR and improved CO and CI (43 mmHg, 7.3 UW, 4.8 l/min and 3.6 l/min/m2, respectively). After evaluation, the Rheumatology Department confirmed the diagnosis of systemic lupus erythematosus by clinical and immunological criteria, and class II lupus nephritis by renal biopsy.
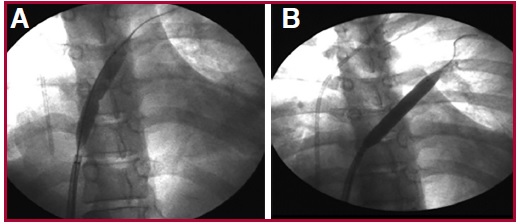
Fig. 2 Transseptal balloon septostomy. Balloon dilatation is performed reaching a maximum diameter of 5 mm under fluoroscopic guidance. A: Balloon inflation on guide wire centered in the atrial septum. B: Total balloon inflation.
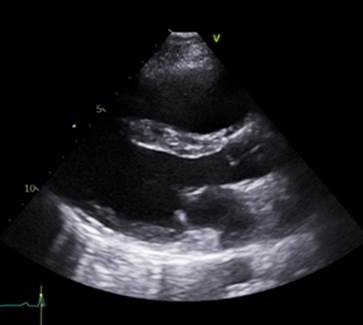
Fig. 3 Long axis parasternal view showing progressive improvement of the right ventricular diameter, reduction of compression to the left ventricle and ventricular septal hypertrophy.
The prevalence of PAH in connective tissue disease (CTD) is high, mainly in scleroderma and also in systemic lupus erythematosus, with a value ranging from 0.5 to 17.5%, depending on the diagnostic method used. 1 This entity continues to present high morbidity and mortality despite the evidence observed with specific drug therapies, which is high compared to idiopathic PAH (1-year survival in CTE-PAH 86% vs 93% in idiopathic PAH). 2 Patients not responding to maximal combination therapy, including parenteral prostanoids, should be referred for double lung transplant. 3 However, many patients with PAH are not candidates for transplantation, or the waiting list time is too long and patients die before being transplanted. For this reason, transseptal septostomy should be considered in patients who are on the waiting list for double lung transplant, in those who do not respond to the maximum therapeutic regimen or when it is unavailable or not tolerated. 4 It should be noted that this procedure is contraindicated in patients with arterial oxygen saturation < 90%, right atrial pressure > 20 mmHg and hemoglobin value < 12 mg/dL, and should be performed in referral centers. Several studies have reported improvement in symptoms and hemodynamics after septostomy, allowing decompression of the right heart with increased left ventricular pre-load and systemic oxygen saturation without complications associated with the procedure in highly experienced centers. 5
Recently, a meta-analysis of 6 studies with 204 patients observed a reduction in right atrial pressure (p< 0.001), an increase in cardiac index (p < 0.001) and left atrial pressure (p < 0.001), but with significant reduction in oxygen saturation and 48-hour, and 30- day mortality rates of 4.8% and 14.6%, respectively. 6
These data suggest that atrial septostomy is an invasive and relatively safe procedure in experienced centers and should only be indicated in patients with advanced severe PAH as a bridge to transplantation or when there is no response to the triple regimen with parenteral prostanoids, or when drug therapy is unavailable.

