











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
PermalinkINTRODUCTION
Acute coronary syndromes (ACS) are mainly made up of the spectrum of patients with epicardial coronary artery disease in whom the index event is secondary to plaque rupture, and are classified as unstable angina (UA), non-ST-segment elevation myocardial infarction (NSTEMI) and ST-segment elevation myocardial infarction (STEMI). 1 Patients without significant epicardial coronary artery disease may also fall into the ACS spectrum and are divided into different categories; although their etiology and pathophysiology may differ widely, the final event is myocardial injury in all the categories. 2-4
Over the past few years, several randomized and observational studies have provided new treatments and interventional strategies to address the different types of ACS. However, due to the situation in our region, it is difficult to determine which modalities are implemented in our daily practice and to what extent they are used, especially considering the wide spectrum of diseases due to acute myocardial injury.
In our country, the most updated information available comes from the BUENOS AIRES 1 registry published in July 2020, which gathered 1100 patients with a diagnosis of NSTEACS in multiple centers in the Autonomous City of Buenos Aires and the Province of Buenos Aires. 5 Previous information was provided by registries developed by the Argentine Society of Cardiology (SCAR registry) in 2011 and the Argentine Council of Residents in Cardiology (CONAREC XVII registry), which collected information from patients treated during 2010. 6,7 Furthermore, the ARGEN-IAM-ST registry is continuously evaluating the in-hospital outcome of patients with ST-segment elevation myocardial infarction and has even published an analysis of patients without significant epicardial lesions. 8-11 These registries have provided extremely valuable information for understanding the current regional situation; however, in our case, and unlike previous registries, our intention is to expand this information by adding to our registry data on the prevalence, diagnosis and treatment of the entire spectrum of acute coronary syndromes, including, for the first time, those without significant epicardial coronary artery disease.
METHODS
ReSCAR was a prospective multicenter observational registry carried out in medical centers of Argentina and included patients between January and August 2022. The registry was designed and conducted by the Council on Cardiovascular Emergency Care of the Argentine Society of Cardiology (SAC).
Participating centers
The participating centers were affiliated to the Argentine Society of Cardiology and fulfilled the following require ments: they had coronary care unit, 24-hour catheterization lab availability and cardiovascular surgery capabilities. All the centers in Argentina were invited to participate.
Follow-up
The pre-established follow-up of patients at 12 months is ongoing; therefore, we do not have final data at the time of publication of the initial analysis. We used the information obtained by telephone contact and complemented with data retrieved from the medical records.
Objectives
- To describe the characteristics of patients hospitalized for a coronary event, the diagnostic modalities, and their treatment.
- To analyze the in-hospital outcome of patients with ACS, according to the different etiologies and treatment strategies implemented.
Inclusion criteria
- Patients older than 18 years, with ACS (with or without significant epicardial coronary artery disease) who signed the informed consent were included.
Sample
We planned to include 1000 patients, which should allow us to have enough number of the different ACS categories. Patients' data were uploaded using the RedCap platform, with one user per center.
Collected data
Past medical history: cardiovascular risk factors and relevant medical history and comorbidities were obtained during history taken at the time of hospital admission. The following variables were recorded: history of hypertension, diabetes mellitus, dyslipidemia, smoking habits (current or former smoker), 12 family history of early cardiovascular disease, sedentary lifestyle, self-reported emotional stress, chronic obstructive pulmonary disease (COPD), chronic kidney disease (CKD), history of COVID-19 and other relevant medical history and comorbidities. In addition, we asked about history of cardiovascular diseases, acute myocardial infarction (AMI), percutaneous coronary intervention (PCI), coronary artery bypass grafting (CABG), chronic stable angina (CSA), stroke, transient ischemic attack (TIA), atrial fibrillation (AF), peripheral vascular disease (PVD), and previous bleeding events.
Characteristics of ACS: the information related with the ACS was obtained from the medical record, considering:
a) Type of ACS: UA, NSTEMI, STEMI, type 2 AMI, myocardial infarction with non-obstructive coronary arteries (MINOCA), myocarditis or Takotsubo syndrome. 1,2
b) Killip and Kimball (KK) class at admission and during hospitalization.
c) Electrocardiographic (ECG) changes: temporary ST-segment elevation; ST-segment depression, T-wave changes, Q waves associated with ST-segment deviations or T-wave changes, left bundle branch block (LBBB), pacemaker rhythm or absence of acute ischemic changes.
d) Initial strategy used (invasive or conservative) and time to coronary angiography (CA).
e) Treatment implemented: aspirin (ASA), P2Y12 receptor inhibitor (P2Y12i) used and time of prescription, and anticoagulant therapy and drug used.
f) Result of CA, type of lesions, number of vessels and type of stent used.
g) Ischemic complications:
1. Recurrent angina, refractory angina, post-infarction angina
2. Reinfarction
3. Stent thrombosis
4. Need for CABG
7. Stroke/TIA
h) Electric complications: atrial fibrillation, ventricular tachycardia or ventricular fibrillation and high-degree atrioventricular block.
i) Mechanical complications: ventricular septal defect, acute mitral regurgitation, free wall rupture.
j) Need for mechanical ventilation or ventricular assist device.
k) Other complications: contrast-induced nephropathy, acute kidney injury (AKI) and heart failure.
l) Bleeding during hospitalization according to BARC types 1-5 13
m) In-hospital mortality.
n) Treatment on hospital discharge: antiplatelet therapy (aspirin, clopidogrel, prasugrel or ticagrelor), oral anticoagulation, beta-blockers (BB), angiotensin converting enzyme inhibitors (ACEIs), angiotensin II receptor blockers (ARBs), statins, ezetimibe, aldosterone antagonists, trimetazidine and calcium channel blockers.
o) Length of hospital stay.
Statistical analysis
All the statistical calculations were performed using IBM SPSS 25.0 software package (for Mac iOS). Continuous variables were expressed as median and interquartile range (IQR) according to the characteristics of their distribution. Categorical variables are expressed as frequencies and percentages. Normality of variables distribution was assessed using the Kolmogorov-Smirnov test or the Shapiro-Wilk test, as applicable. The chi square test or Fisher's exact test were used to compare the categorical variables, and continuous variables were analyzed using the Student's t test or the Mann-Withney test according to their distribution. A type I error < 5% (two-tailed p value < 0.05) was considered statistically significant.
Ethical considerations
All the patients gave their informed consent before participating in the study. Patients were clearly informed about the aim of the study and the mechanisms used to protect their identity to ensure the confidentiality of the data provided. They were informed that their participation was voluntary, that they could refuse to participate in the study without any consequences or differences in their medical care, and that they had the right to withdraw their consent at any time.
During the evaluation process for inclusion in the study, the investigator provided verbal explanation to the patient of the information included in the informed consent and answered all the participant's questions regarding the study. The consent was submitted for approval by the local institutional review board, which is under the regulations of the Central Review Board.
The investigators implemented measures to protect the confidentiality of all the information according to the Argentine Personal Data Protection Law 25 326, so the identity of the patients and all their personal data will remain anonymous, and only the researchers and the members of the learning, teaching and research ethics committee would have access to these data, if required.
The study was conducted following national ethical standards (Law 3301 of the city of Buenos Aires, National Law for Good Clinical Practice in Research on Human Subjects, and the Declaration of Helsinki, among others).
RESULTS
A total of 984 patients were included; median age was 66 years (IQR 56.5-74), and 75.3% were men. The prevalence of hypertension was 68.1%; 25.9% of the patients had diabetes mellitus, 46.1% had dyslipidemia, 56.9% were current or former smokers and 7.8% presented family history (Table 1). A history of UA or NSTEMI, remote PCI, recent PCI, and previous CABG was reported by 25.4%, 19,5%, 7.1% and 7.1% of the patients, respectively.

On admission, median GRACE score and median CRUSADE score were 127 (IQR 104-154) and 22 (IQR 13-34), respectively. The hemodynamic status was classified as Killip and Kimball (KK) class A in 88.1% of patients, B in 8.2%, C in 1.3% and D in 2.4%.
Most ACS corresponded to epicardial coronary artery disease: UA 22.2%, NSTEMI 39.1% and STEMI 24.1%. Additionally, 4.1% presented as type 2 AMI, 1.2% as myocarditis, 0.7% as Takotsubo syndrome and 8.6% as MINOCA.
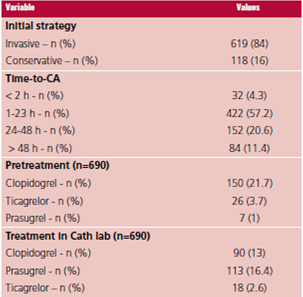
An initial invasive strategy was used in 84% of the patients without ST segment elevation; 76.5% of them had significant stenosis > 50% with multivessel disease in 33.7% and left main coronary artery disease in 13.8%. Percutaneous revascularization was performed in 61.2% and surgical revascularization in 8.5%. Delay to CA was measured in intervals of ≤ 2 h (4.3%), 2-23 h (57.2%), 24-48 h (20.6%) and > 48 h (11.4%). Among patients in whom CA was carried out, pretreatment with a P2Y12 inhibitor was used in 26.4% and clopidogrel was the agent most used, in more than 80% of the cases. Among those patients treated with a P2Y12 inhibitor in the catheterization lab (32%), prasugrel was the one more commonly used. (Table 2).
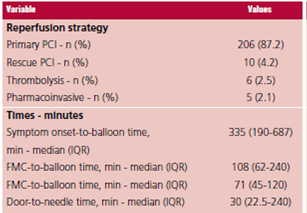
Primary PCI was the most frequent strategy in STEMI patients (87.2%), followed by rescue PCI (4.2%), thrombolytic therapy (2.5%) and pharmacoinvasive strategy (2.1%). In patients undergoing primary PCI, median (IQR) times were as follows: pain-to-balloon time, 335 min (90-687); first medical contact-to-balloon time, 108.5 min (62-240); and door-to-balloon time, 72 min (41-120). In patients treated with thrombolysis, median door-to-needle time was 30 minutes (22.5-24) (Table 3).
Median length of hospital stay was 3 days. During hospitalization, 2.84% of the patients presented reinfarction, 2.43% recurrent angina, 2% postinfarction angina and 0.5% stent thrombosis. Bleeding events occurred in 4.4% of the patients and were almost equally distributed (34% BARC type 1, 34% BARC type 2, and 32% BARC type 3).
Total in-hospital mortality was 3.76% (37 events). The highest mortality rate occurred in those patients with STEMI (7.6%) followed by NSTEMI (3.6%) and UA (2.3%); none of the patients with the other types of ACS died.
Finally, we analyzed the discharge medication. Among the antithrombotic regimen, 86.9% of patients were discharged with aspirin, 76% with a P2Y12i (clopidogrel in 56.6%) and 10.7% with oral anticoagulants, mostly (52.4%) direct anticoagulants (DOACs) and vitamin K antagonists in the rest of the cases. Statins were indicated in 90.9% of the patients and beta blockers in 78%.
DISCUSSION
The ReSCAR registry emerges from a multicenter database that provides the possibility of analyzing updated information about the diagnostic approach, treatment strategies implemented, outcome, complications, and prognosis of all the ACS, and of each ACS category. We would like to highlight five aspects of the data collected.
First, the registry has adequate representation of the spectrum of patients with "acute coronary syndrome" with a similar percentage of UA, NSTEMI, and STEMI. In addition, there is a place for describing the prevalence of MINOCA, myocarditis and Takotsubo syndrome, which represent part of the differential diagnoses of patients admitted with suspected ACS.
Second, in patients without ST segment elevation at presentation, as in the BUENOS AIRES 1 registry, invasive treatment predominated (84% vs. 86%); this implies a more aggressive approach despite most cases were NSTEMI (39.1%), the median GRACE score was 127, which represents an intermediate risk, and most of the sample presented with KK class A (88.1%). 5 We may consider that the predominance of invasive treatment was due to the preference of the treating medical team rather than to the ischemic risk, which was favored by the context of high complexity centers with high access to PCI. However, this was not so common in international registries, as the Swedish SCAAR registry (NSTEACS n = 15 442), where the rate of coronary angiography as initial management for patients with NSTEACS is 62.9%. 14-16
Third, this last registry showed a decrease in the pretreatment strategy (26.4%) compared with the BUENOS AIRES 1 registry, with a pretreatment rate of 65%. This could be explained by the latest recommendations of the ESC guidelines on NSTEMI which, based on the recent ACCOAST and ISAR REACT 5 studies, do not recommend the pretreatment strategy if an early CA strategy (<48hs) is decided. 5,17,18 Since most of the participating centers in our study have catheterization lab availability, this strategy was implemented in more than 60% of patients within 24 h and in 88% within 48 h. Clopidogrel was still the antiplatelet agent most used for pretreatment as in the BUENOS AIRES 1 registry, probably because of its lower cost and greater accessibility compared with ticagrelor, while in those treated in the catheteriza tion laboratory, prasugrel was the antiplatelet agent most used (more than half of the cases) in line with the recent evidence available from the ISAR REACT 5 study. 5,17-23
Fourth, the analysis of STEMI shows a high reper fusion rate with primary PCI with long out-of-hospital times and, in contrast, in-hospital times in line with the recommendations of the clinical practice guidelines and similar to those found in other international registries. 15,16 Mortality is higher than that reported by high complexity centers in the United States or Europe, close to 4.5%, but lower than the one shown in the analysis of the ARGEN-IAM registry. 11
Fifth, in-hospital mortality rate was 3.76%, higher than that of the BUENOS AIRES 1 registry (2.7%), which could be explained because high-risk patients were included, considering a GRACE score of 104 in the BUENOS AIRES I registry and the fact that patients with STEMI were included in the ReSCAR registry. These patients had the highest mortality rate, 7.6% versus 3.6% in NSTEMI patients and 2.3% in those with UA. 7,11
Finally, the rate of bleeding events was low (4.4%), less than expected, and significantly lower than the one recorded in previous similar studies, such as BUENOS AIRES 1 (20.9%). 5 It should be noted that all the patients in BUENOS AIRES I had epicardial coronary artery disease, with a revascularization rate of 76.5% of the sample by both revascularization methods. Despite the ReSCAR study included patients without heart disease, the revascularization rate was 69.5% (8.5% by CABG), which should result in similar bleeding risks associated with revascularization, especially considering the group of patients with diagnosis of STEMI. Therefore, we conclude that part of the bleeding events, especially those categorized as BARC type 2 or type 1, were probably under-recorded.
CONCLUSION
The multicenter ReSCAR registry represents a first approach to the wide spectrum of patients with myocardial injury as the final event, independently of the etiology. The registry has a good representation of the spectrum of patients with initial suspicion of “acute coronary syndrome”, managed in centers with an invasive initial strategy, low rate of in-hospital complications and acceptable overall mortality. The subgroup analysis will provide further conclusions.

