










Serviços Personalizados
Journal

Artigo
 texto em
texto em  Espanhol (pdf)
Espanhol (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkRevista argentina de cardiología
versão On-line ISSN 1850-3748
Rev. argent. cardiol. vol.92 no.1 Ciudad Autónoma de Buenos Aires mar. 2024 Epub 28-Fev-2024
http://dx.doi.org/10.7775/rac.es.v92.i1.20730
SCIENTIFIC LETTER
Molecular Imaging of a Cardiac Paraganglioma

We present a 12-year-old male patient, with no relevant medical history, who began with intense headache associated with severe arterial hypertension of unknown cause. Lab test detected elevated urinary normetanephrine. Abdominal magnetic resonance imaging (MRI) showed no specific features.
Exploratory positron emission tomography combined with computed tomography (PET-CT) with 18F-DOPA (a radiotracer analogue of L-DOPA) was requested due to suspicion of a functioning paraganglioma of unknown location.
The 18F-DOPA PET-CT showed a hyperenhancing intracardiac mass located in the right atrium, with intense enhancement in the arterial phase of intravenous contrast, as can be seen in Figure 1.
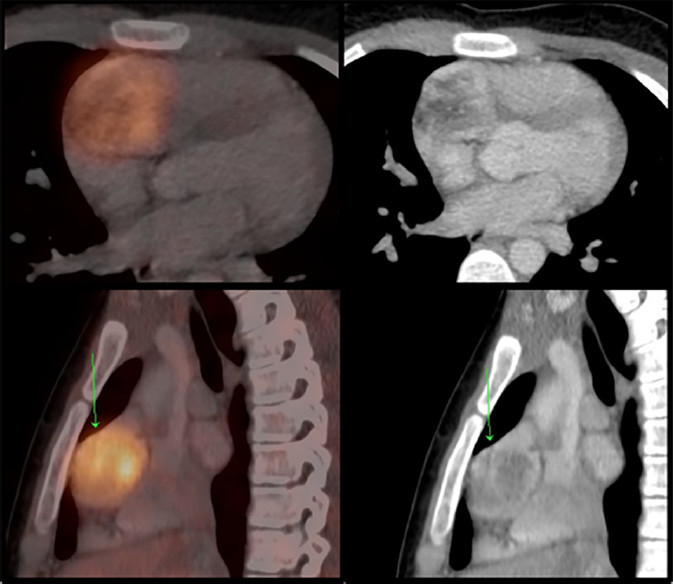
Figure 1 18F-DOPA PET - CT showed a hyperenhancing and hypervascularized mass at the level of the right atrium.
It is important to highlight the great difference that exists between the pathological uptake of the mass and the physiological fixation of the cardiac tissue, due to the presence and functionality of L-amino acid transporters (LAT) and the enzymes of the biogenic amine metabolic pathway, in relation to the neuroendocrine nature of the tumor.
The exact localization of the pathology was crucial for surgical planning. In the 18F-DOPA PET-CT performed for evaluation after surgery, the suture threads are observed after complete excision. (Figure 2)
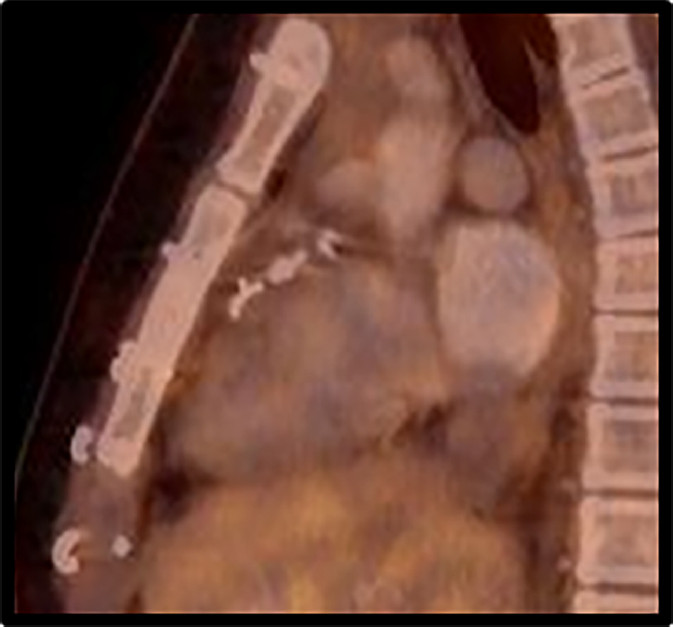
Figure 2 18F-DOPA PET-CT treatment response assessment. The hyperenhancing mass observed in Figure 1 is no longer noticeable, and the post-surgical morphological changes are seen.
Paragangliomas are neuroendocrine tumors that originate in paraganglionic cells derived from the neural crest. These cells form accumulations or conglomerates called paraganglia, which are located very close and related to the ganglia of the Autonomous Nervous System (ANS) in its two subdivisions and are disseminated throughout the body.
Although they can be of sympathetic or parasympathetic lineage, paraganglia have morphologically no differences. The sympathetic ones are located nearby, on the surface or embedded in the capsules of the sympathetic chain ganglia or in the fibers of the large autonomic plexuses. The adrenal medulla is a sympathetic paraganglion specialized in producing epinephrine.
The parasympathetic paraganglia are located along the cranial and thoracic branches of the glossopharyngeal and vagus nerves, at the level of the head, neck, and middle and anterior mediastinum. Despite containing neurosecretory granules and having the potential to exhibit signs of physiological activity, the vast majority of paragangliomas arising from parasympathetic paraganglia are non-secreting. On the other hand, paragangliomas of sympathetic origin may or may not secrete biogenic amines. 1
Germline mutations in more than 20 genes have been identified as responsible for more than a third of paragangliomas, thus revealing their rich hereditary nature. Depending on the mutation that causes them, they are classified into three clusters or genetic groups: pseudohypoxic, related to the kinase signal, and those related with WNT signaling. Each of these groups present distinctive differences from each other in terms of their biochemical, genetic and molecular characteristics, and each of these particular profiles has a direct impact on the clinical presentation. 2
Less than 2% of paragangliomas are located in the thorax, and cardiac locations are extremely rare. 3
Paragangliomas of the heart originate from the visceral paraganglia; they are described at the level of all cardiac chambers, predominantly the left atrium, and present high morbidity due to the high levels of norepinephrine they produce, with the consequent cardiovascular signs and symptoms. 4
The most common clinical presentation of cardiac paragangliomas is, as described above, characteristically noradrenergic. Distinctive symptoms are hypertension, palpitations and arrhythmia. It may also have a silent profile, when dedifferentiation does not allow the production of biogenic amines.
The vast majority of cardiac paragangliomas are pseudohypoxic, with a starting point in mutations of the different subunits of the mitochondrial succinate dehydrogenase (SDH) complex, predominantly SDHB, SDHC and SDHD. These paragangliomas are characterized by having a high density of somatostatin receptors and also variable presence/functionality of LAT and enzymes of the noradrenergic metabolic pathway, their vesicles housing dopamine or norepinephrine when they are functional, as occurs in most cases. 4
The radiopharmaceuticals used to evaluate these tumors are 68Ga-DOTAs (somatostatin receptor ligands) and 18F-DOPA (LAT amino acid substrate). Therefore, PET-CT with 18F-DOPA is one of the morphometabolic tools used for its study.
18F-DOPA is a radiolabeled amino acid that is introduced into the cells through the aforementioned LAT. It is a substrate of the cytoplasmic aromatic amino aciddecarboxylase (AADC) enzyme, which transforms LDOPA into dopamine, the first of the biogenic amines in the metabolic pathway. It will then be converted within the vesicles into norepinephrine, according to the functionality of the dopamine beta-hydroxylase enzyme. 5
These radiolabeled biogenic amines (18Fdopamine and 18F-norepinephrine), which originate from 18F-DOPA administered to the patient, are stored in the secretory granules of the paraganglioma, and constitute one of the molecular tools indicated for staging and evaluating the response to treatment.
In conclusion, molecular images are an essential tool for the correct staging and assessment of response to treatment of cardiac paragangliomas. Accurate localization is crucial for the correct pre-surgical planning, and post-surgical molecular verification must correlate with biochemical negativization, and clinical improvement.
REFERENCES
1. Crona J, Taïeb D, Pacak K. New Perspectives on Pheochromocytoma and Paraganglioma: Toward a Molecular Classification. Endocr Rev. 2017;38:489-515. https://doi.org/10.1210/er.2017-00062 [ Links ]
2. Taïeb D, Pacak K. New Insights into the Nuclear Imaging Phenotypes of Cluster 1 Pheochromocytoma and Paraganglioma. Trends Endocrinol Metab. 2017;28:807-17. https://doi.org/10.1016/j.tem.2017.08.001 [ Links ]
3. Wang JG, Han J, Jiang T, Li YJ. Cardiac paragangliomas. J Card Surg. 2015;30:55-60. https://doi.org/10.1111/jocs.12455 [ Links ]
4. Tella SH, Jha A, Taïeb D, Horvath KA, Pacak K. Comprehensive review of evaluation and management of cardiac paragangliomas. Heart. 2020;106:1202-10. https://doi.org/10.1136/heartjnl-2020-316540 [ Links ]
5. Taïeb D, Imperiale A, Pacak K. (18)F-DOPA: the versatile radiopharmaceutical. Eur J Nucl Med Mol Imaging. 2016;43:1187-9. https://doi.org/10.1007/s00259-016-3354-0 [ Links ]
 This is an open-access article distributed under the terms of the Creative Commons Attribution License
This is an open-access article distributed under the terms of the Creative Commons Attribution License
