










Serviços Personalizados
Journal

Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkActa Odontológica Latinoamericana
versão On-line ISSN 1852-4834
Acta odontol. latinoam. vol.28 no.3 Buenos Aires dez. 2015
ARTÍCULOS ORIGINALES
Family impact scale (FIS): cross-cultural adaptation and psychometric properties for the Peruvian Spanish language
Jenny Abanto1, Ursula Albites2, Marcelo Bönecker1, Saul M. Paiva3, Jorge L. Castillo4, Denisse Aguilar-Gálvez2
1 Department of Pediatric Dentistry and Orthodontics, School of Dentistry, University of São Paulo, Brazil.
2 Department of Pediatric Dentistry, Dental School, Universidad Científica del Sur, Peru.
3 Department of Pediatric Dentistry and Orthodontics, School of Dentistry, Federal University of Minas Gerais, Brazil.
4 Department of Pediatric Dentistry, Dental School, Universidad Peruana Cayetano Heredia, Peru.
CORRESPONDENCE Dr. Jenny Abanto Department of Pediatric Dentistry and Orthodontics Faculty of Dentistry, University of Sao Paulo. Av. Lineu Prestes, 2227, Sao Paulo SP, 05508-000, Brazil. jennyaa@usp.br
ABSTRACT
The lack of a Family Impact Scale (FIS) in Spanish language limits its use as an indicator in Spanish-speaking countries and precludes comparisons with data from other cultural and ethnic groups. The purpose of this study was therefore to adapt the FIS cross-culturally to the Peruvian Spanish language and assess its reliability and validity. In order to translate and adapt the FIS cross-culturally, it was answered by 60 parents in two pilot tests, after which it was tested on 200 parents of children aged 11 to 14 years who were clinically examined for dental caries experience and malocclusions. Internal consistency was assessed by Cronbach’s alpha coefficient while repeat administration of the FIS on the same 200 parents enabled the test-retest reliability to be assessed via intraclass correlation coefficient (ICC). Construct and discriminant validity were based on associations of the FIS with global ratings of oral health and clinical groups, respectively. Mean (standard deviation) FIS total score was 5.20 (5.86). Internal consistency was confirmed by Cronbach’s alpha 0.84. Test-retest reliability revealed excellent reproducibility (ICC = 0.96). Construct validity was good, demonstrating statistically significant associations between total FIS score and global ratings of oral health (p=0.007) and overall wellbeing (p=0.002), as well as for the subscale scores (p<0.05) with exception of the financial burden subscale. The FIS was also able to discriminate between children with and without dental caries experience and malocclusions (p<0.05). Satisfactory psychometric results for the Peruvian Spanish FIS confirm it as a reliable, valid instrument for assessing the impact on the family caused by children’s oral conditions.
Key words: Oral health; Quality of life; Family.
RESUMEN
Escala de impacto familiar (FIS): adaptación transcultural y propiedades psicométricas al idioma Español de Perú
La falta de la Escala de Impacto Familiar (FIS) en el idioma espanol limita su uso como indicador en paises hispanohablantes, asi como impide las comparaciones con diferentes grupos culturales y etnicos. Por lo tanto, el objetivo de este estudio fue adaptar transculturalmente el FIS al idioma espanol de Peru y evaluar su validad y confiabilidad. Para traducir y adaptar transculturalmente el FIS, 60 padres respondieron al instrumento en dos pruebas piloto. Posteriormente, el FIS fue probado en 200 padres de ninos de 11 a 14 anos de edad, quienes fueron clinicamente evaluados para la experiencia de caries dental y maloclusiones. La consistencia interna fue evaluada por el coeficiente alfa de Cronbach, mientras que la re-aplicacion del FIS en los mismos 200 padres permitio la evaluacion de la confiabilidad testretest por medio del coeficiente de correlacion intraclase (CCI). La validez de constructo y discriminante se basaron en las asociaciones del FIS con las puntuaciones globales de salud bucal y grupos clinicos, respectivamente. La media (desviacion estandar) de la puntuacion total del FIS fue 5,20 (5,86). La consistencia interna fue confirmada por el alfa de Cronbach de 0,84. La confiabilidad test-retest revelo una excelente reproducibilidad (CCI=0,96). La validez de constructo fue buena, demostrando una asociacion estadisticamente significativa entre la puntuacion total del FIS y las puntuaciones globales de salud bucal (p=0,007), bienestar (p=0,002), asi como para las puntuaciones de las sub-escalas (p<0,05), con excepcion de la sub-escala de carga financiera. El FIS fue capaz de discriminar ninos con y sin caries dental y maloclusiones (p<0,05). Los resultados psicometricos satisfactorios de la version peruana del FIS confirman que es un instrumento valido y confiable para evaluar el impacto en la familia causado por las condiciones bucales de los ninos.
Palabras clave: Salud bucal; Calidad de vida; Familia.
INTRODUCTION
Oral diseases and disorders are common during childhood and have a negative impact on children’s oral health-related quality of life (OHRQoL)1,2. The American Academy of Pediatrics defines child health as ‘the social, physical and emotional functioning of the child and, when indicated, his or her family… therefore, measurement of health-related quality of life must be from the perspective of the child and the family’3. However, there are few instruments that evaluate the impact of a child’s oral condition on the family’s quality of life (QoL). The only instrument available for this purpose is the Family Impact Scale (FIS)4.
To date, the validity and reliability of the FIS have been demonstrated in English-speaking parents in Canada5, United Kingdom6, China7 and Brazil8. Nevertheless, although it has been validated in some languages, to the best of our knowledge, it has not been cross-culturally adapted and validated in Spanish. The lack of the FIS in Spanish language limits its use in Spanish-speaking countries, such as Peru, and precludes comparisons with data from other cultural and ethnic groups9. In addition, the FIS has a potential role considering that a parent’s reports of the child’s oral health or OHRQoL may be influenced by the degree to which the parent is physically or psychological affected by the child’s condition5,10. Therefore, the aim of the present study was to carry out the cross-cultural adaptation of the FIS to the Peruvian Spanish language and to test its reliability and validity.
MATERIAL AND METHODS
The study was approved by the Human Research Ethics Committee of the Cientifica del Sur University, Peru. The participants’ legal guardians signed an informed consent form.
Description of the Family Impact Scale (FIS)
The FIS consists of 14 items divided into three subscales5: parental ⁄ family activity (PA), parental emotions (PE), family conflict (FC) and financial burden (FB). The items refer only to the frequency of events in the previous 3 months. The items have five Likert response options: ‘never = 0’, ‘once or twice = 1’, ‘sometimes = 2’, ‘often = 3’, and ‘every day or almost every day = 4’. The number of ‘don’t know’ responses was counted, but excluded from the total FIS score for each patient.
Total FIS scores and scores for individual subscales are calculated as a simple sum of the response codes. Since there are 14 items, the final score can range from 0 to 56, where a higher score denotes greater impact of a child’s oral condition on family QoL. Following the validation process of the original FIS, answers were obtained to two questions asking the parents for global ratings of their children’s oral health and the extent to which their oral health affected their overall well-being5. These global ratings had a five-point response format. The responses were scored as follows: “excellent”=0, “very good”=1, “good”=2, “average”=3, “poor”=4 for oral health, and not at all=0, very little=1, somewhat=2, a lot=3 and very much=4 for general wellbeing.
Translation and Adaptation of the FIS
The original FIS was translated and adapted to Spanish for Peru following standard guidelines11-13. Based on these guidelines, two initial translations into Spanish were made independently by two native Spanish translators. Both translations were reviewed in a consensus meeting in Peru. The Review Panel for this meeting consisted of four postgraduate professors, fluent in both Spanish and English, who knew the objectives of the study and had experience in OHRQoL studies13. The Review Panel evaluated the translations and determined the conceptual and item equivalence in order to retain content similarity in the different cultures. A consensus-translated version of the FIS was developed as a result of this process and then pilottested on a convenience sample of 40 parents of children aged 11–14 years old. Modifications were made according to parents’ suggestions, in order to clarify the content of the instrument. The panel developed a first Peruvian version of the FIS, which was translated back into English by two native English-speaking translators. The back-translated English consensus version was compared to the original English version to determine semantic equivalence.
Finally, the draft of the first version of the FIS was pilot-tested for a second time on a different convenience sample of twenty parents of 11-to-14- year-old children. There was no change in terms of new suggestions or difficulties in comprehension, and the Review Panel wrote the final Peruvian version of the FIS. The Peruvian version of the FIS during pilot tests and assessment of psychometric properties was administered in face-to-face independent interviews. Structures, instructions, mode of administration and measurement methods of the instrument were similar to the original English version of the FIS5.
Assessment of validity and reliability
Validity is usually assessed on a sample size of 50 to 200 people in a cross-sectional design, while testretest reliability is assessed on a sub-sample (of about 10% or 30 people)11-13. In line with this requirement, the Peruvian version of the FIS was administered in face-to-face independent interviews with 200 parents of 11- to 14-year-olds from four schools – two public schools in a deprived area and two private schools in a wealthy area. All schools were located in the city of Lima, capital of Peru. Children were randomly selected from official school registries. All parents were invited to participate in the study according to the following inclusion criteria: parents who have children with no systemic and ⁄ or neurological diseases, with children who could be examined intra-orally and who had not received dental treatment during the study. Interviews were carried out before the clinical oral examinations by three trained interviewers who were blind to the oral screening examination findings. The interviewers were trained in the administration and intonation of each item of the Peruvian FIS. They were also clearly instructed to avoid suggesting responses or showing the answer options while reading them.
The children’s oral examinations looked at dental caries and malocclusions and were carried out by a single specialist in pediatric dentistry who was previously trained and calibrated (Kappa intraagreement = 0.92 and 0.89 for dental caries and malocclusions, respectively). Dental caries experience was assessed as number of decayed, missed and filled teeth (DMFT)14. Then, children were divided into two clinical groups15: those with no dental caries experience (DMFT=0) vs. those with dental caries experience in one or more teeth (DMFT 31). Malocclusions were classified using the Dental Aesthetic Index (DAI)16, and the children were divided into two clinical groups: children with malocclusions and without malocclusions.
Data analysis
The SPSS software program (version 17.0 SPSS Inc., Chicago, IL, USA) was used for data analysis. Descriptive analyses were performed initially to assess the prevalence of oral impacts and measures of central tendency (means and standard deviations) of total and individual domain scores of the Peruvian FIS. Internal consistency of the FIS was assessed using Cronbach’s alpha, inter-item and item-total correlation coefficients. The test-retest reliability was assessed by calculating the Intraclass Correlation Coefficient (ICC) for the FIS score using the data from the same 200 parents who were interviewed for a second time, 7–14 days after the first interview, by the same interviewers. To test construct validity, correlations between the scores of each subscale, total scale and global ratings were analyzed using Spearman’s correlation coefficient. Discriminant validity was tested by comparing the mean FIS scores between children with caries experience/malocclusions and those without. As the FIS scores were not normally distributed, the nonparametric Mann-Whitney test was used to evaluate the difference in mean scores between clinical groups. The level of significance was set at 0.05.
RESULTS
A total 243 parents were invited to participate in the validation study, of whom 43 were not included because they did not conform to the study criteria. All 200 eligible parents provided signed parental informed consent, resulting in a response rate of 82.3%. Of the 200 parents interviewed, 85.0% were mothers and 15.0% fathers. The mean (standard deviation) age of children was 12.5 (1.12), of whom 95 (47.5%) attended public schools and 105 (52.5%) attended private schools. Of these, 54.0% were girls and 46.0% boys, and a total 108 (54.0%) and 148 (74.0%) had dental caries experience and presence of malocclusions, respectively.
All questionnaires were completed. The scores for the total scale in the study population ranged from 0 to 28, with a mean (standard deviation) of 5.20 (5.86). Overall, 64.5% of parents reported oral impact (total FIS scores >0). Of these, 121 parents (60.5%) reported experiencing impact on parental/ family activity; 110 (55.0%) reported impact on parental emotions; 98 (49.0%) reported impact on family conflict and 46 (23.0%) reported financial burden impacts.
Reliability
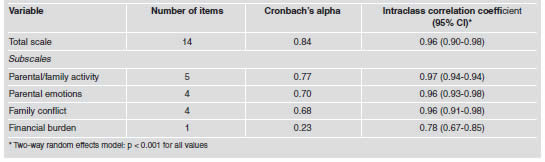
Cronbach’s alpha coefficient was 0.84 for the total scale and ranged from 0.23 for financial burden subscale to 0.77 for parental/family activity subscale (Table 1). Test-retest reliability was assessed using the ICC, which was 0.96 for the total scale ranging from 0.78 for financial burden subscale to 0.97 for parental/family activity subscale (Table 1).
Table 1: Reliability statistics for total FIS scale and subscales (n = 200).
Construct validity
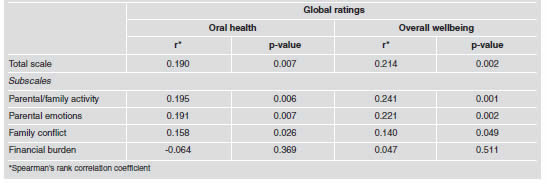
The correlations between global ratings (oral health and overall well-being) and the full scale (r= 0.190 and r= 0.214), parental/family activity subscale (r= 0.195 and r= 0.241) and family conflict subscale (r= 0.158 and r= 0.140) were not strong but statistically significant (Table 2). The financial burden subscale was not significantly associated to global ratings.
Table 2: Construct validity: rank correlations between total FIS scale and subscale scores, and global rating of oral health and overall wellbeing (n = 200).
Discriminant validity
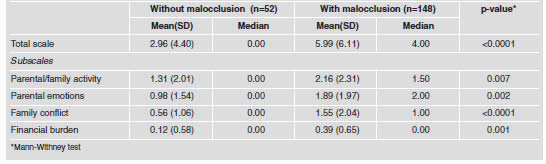
There was a significant difference in total scale and subscales scores of the FIS between children without dental caries experience and those with dental caries experience in one or more teeth (Table 3). This result was similar for malocclusion groups (Table 4).
Table 3: Discriminant validity: total FIS scale and subscales scores for children without and with caries experience.
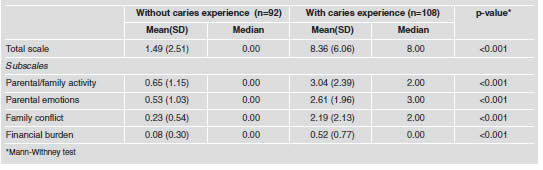
Table 4: Discriminant validity: total FIS scale and subscale scores for children without malocclusion and with malocclusion.
DISCUSSION
This study adapted and validated the FIS cross-culturally for use among Peruvian parents. To the best of our knowledge, this is the first study that has adapted and evaluated the psychometric properties of this measure in a Latin American language such as Spanish after its original validation in English.
When a QoL instrument is translated for use in a context and country different from those it was created in, the cross-cultural adaptation should be evaluated, considering that it will be influenced by the wider social context including family environment, friends, schools and cultural customs in different countries17. By adapting the QoL instrument, its validity and reliability will be similar to those in the original version18. Our study meticulously applies standard guidelines for the translation and cross-cultural adaptation of QoL measures11-13 and conducts pilot tests to identify any potential problems in its content, such as misunderstandings of the intended meaning of the items, clarity and cultural relevance. The results showed semantic equivalence between the English and Peruvian Spanish language versions of the FIS. The Peruvian version of the FIS for the Spanish language also exhibited good psychometric properties and provided acceptable support for its validity and reliability. Test-retest reliability was confirmed by the ICC, which showed excellent correlations between the first and second total FIS scale and subscales scores. Cronbach’s alpha coefficient for the full scale and subscales indicates good internal consistency, as values of 0.5 or above are considered acceptable19. Similar results were obtained in the Canadian, Chinese and Brazilian validation studies5,7,8.
Concerning construct validity, our findings on the associations of the full FIS scale and subscale scores with global ratings on oral health and overall well-being proved the validity of the measure, except between the financial burden (FB) subscale and global ratings. In agreement with our study, the Brazilian FIS version also found that the FB subscale did not correlate with global ratings8. In contrast, in the Chinese version, the FB subscale was only associated with the overall wellbeing rating7. In Canada, the FB subscale was associated with both global indicators5. This may be because the FB subscale comprises a single item and addresses economic rather than psychosocial or behavioral impact5,7. It has therefore been recommended that the full scale score be used as a primary outcome, as there is stronger support for its validity than for the subscales alone7,8.
The ability of the Peruvian FIS to discriminate significantly between different clinical groups according to caries experience and presence of malocclusions was also demonstrated. Similar results were found in the Chinese validation7. However, the Canadian and Brazilian FIS versions did not find significant differences between clinical groups in total scores5,8. Considering the mean values found for both clinical groups in our study, children with dental caries experience achieved higher scores on the total scale and subscales than the malocclusion group, indicating that dental caries could have higher negative impact than malocclusion at this sample age. This may be because dental caries commonly causes toothache and discomfort, demanding more parental attention and concern than malocclusions, which do not usually produce oral symptoms. Parents may thus choose to treat malocclusions or not, sometimes also resulting in higher treatment costs. Since the FIS is a short instrument, it can be used in epidemiological surveys and also as an indicator for purposes such as political, research, public health and clinical actions4.
CONCLUSION
The Peruvian Spanish version of the FIS proved to be valid and reliable for assessing the impact of a child’s oral condition on the family’s quality of life.
ACKNOWLEDGMENTS
This study was financially supported by Fundacao de Amparo a Pesquisa do Estado de Minas Gerais – FAPEMIG.
1. Abanto J, Carvalho TS, Mendes FM, Wanderley MT, Bonecker M, Raggio DP. Impact of oral diseases and disorders on oral health-related quality of life of preschool children. Community Dent Oral Epidemiol 2011; 39: 105-114. [ Links ]
2. Abanto J, Tsakos G, Paiva SM, Carvalho TS, Raggio DP, Bonecker M. Impact of dental caries and trauma on quality of life among 5- to 6-year-old children: perceptions of parents and children. Community Dent Oral Epidemiol 2014; 42:385-394. [ Links ]
3. Fink R. Issues and problems in measuring children’s health status in community health research. Soc Sci Med 1989; 29:715-719.
4. Abanto J, Paiva SM, Raggio DP, Celiberti P, Aldrigui JM, Bonecker M. The impact of dental caries and trauma in children on family quality of life. Community Dent Oral Epidemiol 2012; 40:323-331. [ Links ]
5. Locker D, Jokovic A, Stephens M, Kenny D, Tompson B, Guyatt G. Family impact of child oral and orofacial conditions. Community Dent Oral Epidemiol 2002; 30: 438-448. [ Links ]
6. Marshman Z, Rodd H, Stem M, Mitchell C, Robinson PG. Evaluation of the Parental Perceptions Questionnaire, a component of the COHQoL, for use in the UK. Community Dent Health 2007; 24:198-204. [ Links ]
7. McGrath C, Pang HN, Lo EC, King NM, Hagg U, Samman N. Translation and evaluation of a Chinese version of the Child Oral Health-related Quality of Life measure. Int J Paediatr Dent 2008; 18:267-274. [ Links ]
8. Goursand D, Paiva SM, Zarzar PM, Pordeus IA, Allison PJ. Family Impact Scale (FIS): psychometric properties of the Brazilian Portuguese language version. Eur J Paediatr Dent 2009; 10:141-146. [ Links ]
9. Abanto J, Albites U, Bonecker M, Martins-Paiva S, Castillo JL, Aguilar-Galvez D. Cross-cultural adaptation and psychometric properties of the Child Perceptions Questionnaire 11-14 (CPQ11-14) for the Peruvian Spanish language. Med Oral Patol Oral Cir Bucal 2013; 18: e832-e838. [ Links ]
10. Rothman ML, Hendrick SC, Blucroft KA, Hickman DH, Rubenstein LZ. The validity of proxy generated scores as measures of patient health status. Med Care 1991; 29: 115-124. [ Links ]
11. Guillermin F, Bombardier C, Beaton D. Cross-cultural adaptation of health-related quality of life measures: literature review and proposed guidelines. J Clin Epidemiol 1993; 46:1417-1432. [ Links ]
12. Herdman M, Fox-Rushby J, Badia X. A model of equivalence in the cultural adaptation of HRQoL instruments: the universalist approach. Qual Life Res 1998; 7:323-335. [ Links ]
13. Van Widenfelt BMV, Treffers PDA, Beurs E, Siebelink BM, Koudijs E. Translation and cross-cultural adaptation of assessment instruments used in psychological research with children and families. Clin Child Fam Psychol Rev 2005; 8:135-147. [ Links ]
14. WHO. WHOQOL – measuring quality of life. The World Health Organization quality of life instruments. World Health Organization, Geneva. 1997.
15. Knutson JW. An index of the prevalence of dental caries in school children. Public Health Rep 1944; 59: 253-263. [ Links ]
16. Cons NC, Jenny J, Kohout FJ: DAI: the Dental Aesthetic Index. Iowa, USA: College of Dentistry, University of Iowa, 1986. [ Links ]
17. Cox MJ, Paley B. Families as systems. Annu Rev Psychol 1997; 48:243-267. [ Links ]
18. Albites U, Abanto J, Bonecker M, Paiva SM, Aguilar- Galvez D, Castillo JL. Parental-caregiver perceptions of child oral health-related quality of life (P-CPQ): Psychometric properties for the Peruvian Spanish language. Med Oral Patol Oral Cir Bucal 2014; 19:e220-e224. [ Links ]
19. Cronbach LJ. Coefficient alpha and the internal structure of tests. Psychometrika 1951; 16:297-334. [ Links ]

