











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
PermalinkINTRODUCTION
Bone regeneration in the human body has been studied over the past century with a wide variety of purposes, approaches and surgical materials1. Bone grafts are indicated in medical and dental practice for restoring compromised function and aesthetics due to bone defects2. In oral surgery, bone grafts contribute to the treatment of small to moderate bone defects resulting from periodontal or endodontic disease, dental socket filling after extraction, maxillary sinus lifting or rehabilitation of bone atrophy prior to implants, and even large bone defects caused by traumas, congenital deformities, pathologies and infections involving the maxillofacial complex3.
The choice of a bone substitute should be guided by its physicochemical, mechanical and biological characteristics, including architecture, porosity, resistance, biocompatibility, biodegradability, osteoconduction, osteoinduction and/or osteogenesis, in order to mimic the bone tissue to be repaired4. Biomaterials can be classified according to their origin (autogenous, allogeneic, xenogeneic or alloplastic), composition (metals and alloys, ceramics and bio-glass, polymers or composites) or interaction with the biological environment (bioinert, bioabsorbable or bioactive)5.
There are advantages and limitations in the use of bone grafts. Higher success rates have been achieved with autogenous bone, despite its limited supply and higher morbidity5,6. Donated allografts are more readily available, having been reported over the last sixty years and used increasingly Europe. However, difficulties in processing the biomaterial and risk of an immunogenic inflammatory response may reflect delay or decrease in osteogenesis6. Xenografts have been popular since the 1960s, especially bovine bone, despite the controversies with relation to the risk of transmission of xenozoonoses, which, in fact, have never been documented in dental practice7. Currently, animal byproducts could subsidize the generation of natural materials and contribute to the consolidation of a sustainable industry8. Alloplastic materials are satisfactory alternatives to natural materials, but face the challenge of controlling the great variability of results depending on their composition, associated with resorption and inflammatory or repair responses9. In view of this evidence, there is still no ultimate or single biomaterial for bone reconstruction, which motivates the biotechnological development of the sector10.
The growth of the industry and the consumer market for bone substitute materials for dental use converges with the higher life expectancy of the population and the increase in purchasing power in developing countries11. This market is markedly significant in North America, followed by Europe, Asia, Latin America, Oceania and Africa12. A worldwide increase of 4.4%13 to 9.5%12 is estimated for the period from 2018 to 2026 in guided bone regeneration procedures involving bone grafts and membranes, which may be associated with greater clinical demand from both professionals and patients seeking better results13. In the United States and Europe, more than half a million people annually receive treatment for bone defect repair, and the international bone graft market moved USD 493 million in 2018 and expects to generate USD 931 million by 202514. In Latin America, this market was valued at USD 116.8 million in 201815. In Brazil, the political and economic crisis in the country and the bureaucracy involved in opening new companies are expected to delay the growth of this sector13. In a price-sensitive market, the costs and benefits of bone graft procedures should be considered for clinical choice16.
In this broad market scenario, there is a lack of evidence in the literature about the permeability to bone grafts in dental practice in medium and small cities. The city of Sobral, located in the interior of the State of Ceara, northeastern Brazil (3°41'42.0"S 40°20'28.3"W) is located 232 km from the state capital, Fortaleza. It has an estimated population of 208,935, being the fifth-largest city in this Brazilian state, with a rate of 24.6% of professional occupation, average of 2 minimum monthly wages, gross domestic product per capita of R$ 20,258.09 or USD 4,771.08, municipal human development index of 0.714, 88.35% of urban population, 67.83% in the 15- to 64-year age group and Gini index 0.5617. There are 39 outpatient units with dental care, 1 emergency facility with maxillofacial surgery17, 44 oral health teams in primary care, 2 dental specialty centers (1 municipal and 1 regional) in secondary care18 and 2 schools of dentistry (1 public and 1 privative) with dental care for the population. In the Sobral Campus of the Federal University of Ceara, it was estimated that in 2019, about 4,000 procedures involving oral surgery, periodontics or implantology were performed at the dental clinic.
Thus, the aim of this study was to assess the general profile of use of bone grafts in the perception of dentists in the Brazilian inland.
MATERIALS AND METHODS
Ethical and legal aspects
This research adopted the ethical principles of respect for people, non-maleficence, beneficence and justice described in the Belmont Report (1978) and the Brazilian guidelines of the Resolution of the National Health Council No. 466 (2012), which establishes the basic requirements for research involving human beings in the country. This research was assessed and approved by the local Ethics Committee of the Universidade Estadual Vale do Acarau via Plataforma Brasil (register CAAE #04644918.4.0000.5053 and approval protocol #3.145.268), before data collection started. Participants' consent was registered through a Free and Informed Consent Form (FICF), which provided information in appropriate language about the purpose of the research, as well as ensuring the confidentiality of identities.
Type of study
This was an exploratory, descriptive, crosssectional study by intensive direct observation with a quantitative, structured approach. The target population consisted of dentists working in the city of Sobral.
Sample
In a previous consultation with the Federal Council of Dentistry, which is a professional-class entity responsible for managing all enrollments and the legality of dental practice in Brazil, it was informed that there are 233 registered practitioners in the city of Sobral. Considering a population of 233 dentists in the city of Sobral and calculating a representative sample with 99% confidence interval and 5% margin of error, we idealized a sample of 173 dentists.
To achieve significant, homogeneous sampling, a random field study was conducted from February to September 2019, restricted to the Sobral municipality, using the snowball technique to access these professionals.
Inclusion criteria were dentists working in the city of Sobral, in private practice or public assistance in primary, secondary or tertiary care of the Brazilian Unified Health System, duly registered with the
Federal Council of Dentistry, of legal age (over 18 years old), of either sex, with no limitation regarding year of graduation, and who accepted to participate voluntarily in this study. Professionals who did not sign the FICF or cases of error in filling out forms were excluded.
Data collection
For the standardization of data collection and analysis, an anonymous, self-reported, face-to-face form was used, applied in individual voluntary interviews in a dental office or health unit.
The variables considered in this study were based on the methodology developed by Castro-Silva and Coutinho (2012)19. The form consisted of closed objective or semi-open questions, grouped into five basic categories (professional data, subject knowledge, specific use, cost-effectiveness and biosafety).
Data analysis
After the generation of an electronic bank with data collected in the Excel for Windows software (Office 2010™, Microsoft Corporation, USA), the quantitative variables were described in terms of absolute and relative values, being presented in the form of a table. Intergroup inferential statistical analysis of frequencies was performed using the Statistical Package for the Social Sciences software version 20 (IBM™, USA) applying the chi-square test and Fisher's exact post-test for nonparametric data, considering significant differences if P<0.05.
RESULTS
Among the 233 dentists in the city of Sobral, a total 183 volunteers comprised the sample, equivalent to 78.54% of the city's professionals. Remarkably, the sample used in this study was greater than the size determined using statistical parameters as mentioned above. The representative sample of dentists in this study increases the level of confidence in the results found for the city of Sobral.
The prevalence of females (117 participants) was almost double that of males (66 participants) (Fig. 1A). Mean age±standard deviation was 35.37±10.21 years and there was prevalence of three quarters of the sample in the age group up to 40 years (Fig. 1B). The vast majority of the sample did not have any specialization or expertise in Orthodontics (Fig. 1C). Table 1 shows respondents' general knowledge about bone grafts. Most respondents sample had graduated up to 10 years previously and demonstrated significant familiarity with the subject. They had acquired such knowledge mainly at undergraduate level, in comparison to postgraduate studies and dental conferences. Among the natural or synthetic compositions mentioned, ceramics were the most prevalent, followed by composites, while there was little mention of polymers and glasses. Bovine mineral bone was the material most frequently cited by all participants.
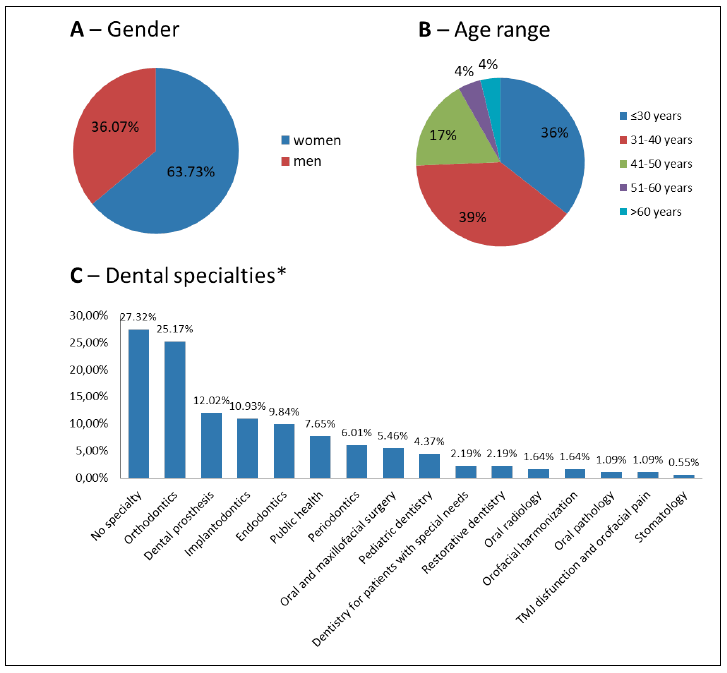
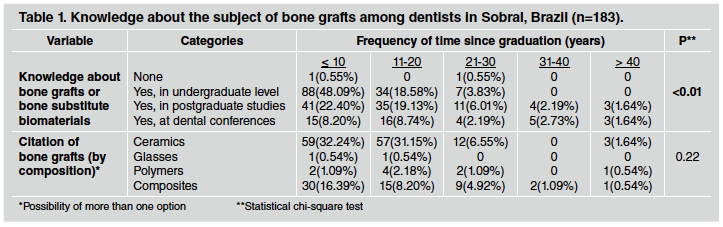
Table 2) shows that only a quarter of the respondents (45 or 24.59%) had performed bone grafts. Regardless of the intensity of use (from <10 to >100 cases), the most frequent bone graft applications were simultaneously with a dental implant, fresh dental sockets and maxillary sinus lifting, while the least frequent were periodontal use, paraendodontic use and extensive bone reconstruction. Autogenous and xenogeneic grafts were more often used than alloplastic and allogeneic grafts. Ceramics were the most frequently used composition of bone grafts and their association with membrane was more frequent than bone graft alone or associated with autologous fibrin.
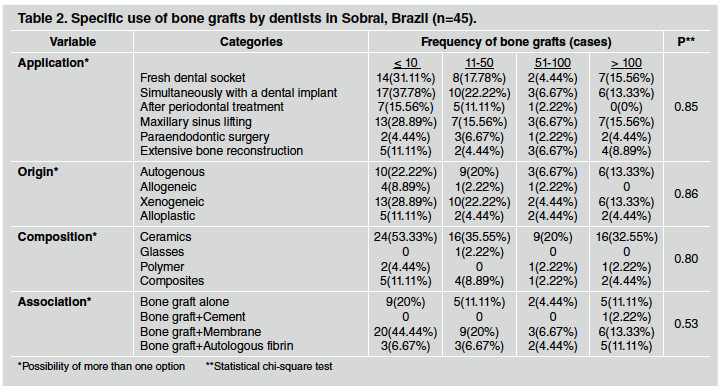
Table 3) shows the high satisfaction of professionals and patients with bone grafts, with material or technical costs being considered moderate.

However, the fact that professionals never or rarely include the patient in the choice of this form of treatment is remarkable. The reported country of origin of the bone graft used differed significantly according to how many bone grafts the respondent had performed: most of those who had performed up to 10 cases did not know country of origin or had used imported material, while respondents who had performed over 50 cases reported using imported or imported+national materials. Use of bone grafts was higher in the private service than in the public for most of the analyzed ranges.
Table 4) shows that professionals always follow datasheets and recommendations for the use of bone grafts. Respondents who had performed up to 50 cases did not overall report having patients with inflammatory or infectious complications after bone grafts, while the profile is significantly reversed for respondents who had performed more than 50 cases, although they reported feeling safe regarding the origin of the materials. In general, both the opinion of the professionals and their perception of the belief of their patients were more favorable to the use of bone grafts from animals than from humans. Within all three dental specialties, the low number of professionals registered in the Brazilian Transplant System for use of bone tissue banks confirms the low level of acceptance among professionals of allografts, with only 2 registered dentists in the specialties of Oral and Maxillofacial surgery or Implantodontics.

DISCUSSION
The local register of 233 dentists for a population of 208,935 inhabitants in Sobral17 shows the ratio of 1 professional to 896 individuals, which is a lower rate than the Brazilian average of 1 dental professional to 668 inhabitants20. Even in the face of favorable demand, the low number of experts would explain the generalist profile of dentists in the city and may explain the low use of bone grafts in the sample. Inorganic bioceramics were bone substitute materials most frequently cited and used by respondents, in agreement with most studies on the subject9,21,22. This preference is supported by osteoconductive action, ability to carry osteogenic cells9,21 or osteoinductive growth factors23, versatility of concentrations, formats and particle sizes22 as well as the possible association of apatites with collagen or other polymers with the aim of achieving biological synergism15,21,24. Thus, the basic understanding of the properties of biomaterials for bone regeneration and their appropriate applications is very important in making a good clinical choice19.
The most frequent clinical applications were simultaneous use with a dental implant, fresh dental sockets and maxillary sinus lifting, in agreement with the two most prevalent surgical beds in the dental literature19,24,25. The present study found a higher frequency of bone graft in association with membranes or autologous fibrin than in isolated form, disagreeing with another Brazilian study19 and international reports, which state that dentists make less use of membranes next to the bone graft because it represents an additional cost to the patient16,26. The adjunct use of autologous fibrin has been promising, as it has a high concentration of angiogenic and osteogenic growth factors, evidencing the evolution of bone regeneration techniques27.
The prevalence of use of autogenous and xenogeneic grafts compared to alloplastic and allogeneic, associated with a more favorable perception of the use of bone grafts from animals than from humans, agrees with other studies on the topic19,28. Autografts are a gold standard for the treatment ofbone defects28, but the preference of professionals for xenografts and alloplastic grafts has increased gradually in Latin America15 and Brazil26 for medical and dental applications3,22. The advantages of xenografts and alloplastic grafts are biomimicry of human bone tissue24 and absence of patient's donor bed, which explains their wide range of clinical uses9,19,22. Stigmatization of the cadaverous source, lack of disclosure29 and ethical, moral or religious values of users could explain low choice of allografts30,31. Satisfaction with bone grafts in this study was high, confirming an Indian study with 59% of utilization31. Refusal rates to bone grafts has been more often associated to the geopopulational context than to age, gender, education and religion, ranging from 2% for alloplastic grafts to 20% for allografts in Chilean study30 or from 11% for autografts to 67% for xenografts in Saudi Arabia29.
The present study confirmed the existing knowledge on use ofmaterials ofimported12,13 or national origin24. Multinational companies, predominantly US, currently dominate the global market for dental bone grafts12,13. Brazilian industry gains representation among companies already consolidated in the market, with 3 out of 5 institutions responsible for 65% of dental bone grafts in the country26.
Costs were considered moderate by the respondents, predominantly from private practice in Sobral, a finding similar to those from a large city in southeastern Brazil19. However, the country suffers from chronic underfunding in public health32, where the costs of procedures can be substantial limitations13,33 and only a small percentage of its population has undergone bone reconstruction procedures16,34. In private practice, costs are associated to the loyalty of dentists to the use of bone grafts33.
Dentists may select therapeutic options that involve high cost, based on their perception of the patient's profile and oral condition or on the patient's feedback regarding motivation or being able to afford the cost of the treatment35. The current study highlighted the low level of patient participation in the choice of material to be grafted, in contrast to most international studies29-31,35. This emphasizes the need to improve professional interaction with patients in order to make successful joint decisions regarding the use of bone graft.
High occurrence of inflammation or infection in grafted patients was proportional to high density of surgical care performed by the respondents. The rigid biosafety involved in processing, sterility and standardized validation tests of grafting12,36 reduces fears regarding the transmission of animal or human diseases30,31 and increases the safety perceived by dentists regarding their use37. Nevertheless, grafting procedure failure can range from 5 to 10% as a result of infections or inappropriate graft stabilization15. Factors such as filling large bone defects with bone block, mixed grafts (autogenous + synthetic) and diabetes mellitus may also be associated with infections38. To reduce potential out-of-office complications with bone grafting, it can be helpful to apply antibiotic therapy used sparingly39 and intensification of care with oral hygiene habits34. Although there is still little dental use of bone grafts in Sobral, their cost-effectiveness and biosafety are generally satisfactory and in accordance with the literature. This study confirms good acceptance by dentists and their knowledge of the subject of bone grafts in Sobral, a medium-sized city in the Brazilian inland, which constitutes a promising scenario for the development of the sector.

