











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
PermalinkINTRODUCTION
Paget’s disease of bone (PDB) is a chronic disease characterized by abnormal bone turnover affecting one or more bones of the skeleton 1-3 . It was first described in 1877 by Sir James Paget who named it osteoitis deformans 4 . It occurs in patients over the age of 55 years and is more prevalent in men (M:F ratio: 2:1) 5 , 6 .
PDB has an unusual geographic distribution, with an increased incidence in the United Kingdom, Germany, France, New Zealand, and Australia 6 , 7 , and being less common in China, Japan, India, Southeast Asia and America 8-13 . The incidence and severity of Paget’s disease has decreased over the last 35 years 14-17 .
Although the etiology of the disease remains unclear, association with different underlying conditions has been suggested. The familial occurrence of PDB has prompted genetic studies, which have reported a mutation in the gene SQSTM1 18 , 19 . In turn, the decrease in the incidence of the disease has brought about the search for environmental factors 14, 18-21 . A possible viral etiology has also been suggested based on evidence of measles virus nucleocapsid protein in pagetic osteoclasts 22 , 23 .
Paget’s disease is asymptomatic in the early stages of the disease, in which osteoclastic activity predominates, subsequently causing an increase in osteoblastic activity that leads to sclerosis and bone deformity. Signs and symptoms vary with progression of the disease according to the affected skeletal site. The most common presenting features are pain, deafness, bone deformities, osteoarthritis, pathological fracture, and, though very rarely, malignant transformation6,24-28.
When the disease involves the jaws, it occurs predominantly in the maxilla, which undergoes progressive enlargement causing displacement of the teeth and malocclusion 29 , 30 . With time, the disproportion in the size between the maxilla and the mandible gives rise to the inverted triangle type of facial contour 3 , 30 . Regardless of the affected skeletal site, the microscopic features of PDB vary throughout the course of the disease. In the early phase, active bone resorption predominates, showing abnormally large osteoclasts containing multiple nuclei. The haversian canals enlarge and coalesce, and the bone marrow shows highly vascularized loose fibrous tissue 6 , 30 . The intermediate stages of the disease are characterized by dysregulated bone remodeling in which active osteoblastic activity coexists with osteoclastic activity, leading to apposition of new bone on the surfaces of the previously resorbed trabeculae. Uncoordinated bone resorption and apposition results an anarchic trabecular structure and altered mechanical properties. Finally, the last phase of Paget’s disease is characterized by sclerotic lamellar bone trabeculae with multiple compartments separated by irregularly arranged incremental and reversal lines, resulting in the characteristic microscopic appearance of PDB with the typical mosaic or jigsaw puzzle pattern 2 , 6 31 .
In addition to the histologic characteristics described above, Paget’s disease of the jaws shows specific features. In the osteolytic phase, varying degrees of tooth mobility and ultimately tooth loss may occur 3, 29-31 . In the intermediate phase, hypercementosis with ankylosis of teeth to the adj acent bone and the presence of spherical structures similar to psammoma bodies can be observed. In the later stages of the disease, these spherical structures fuse and a fibrillar structure can be seen on their surface 29-31 .
Radiographic features vary widely with the stage of the disease and osteoclastic/osteoblastic activity. A radiodense image with a cotton wool appearance is typically seen in the intermediate and late phases 29,31, 32-36 .
Diagnosis is mainly based on radiographic studies, bone scintigraphy, and evaluation of serum bone turnover markers. A biopsy is nevertheless necessary not only to confirm diagnosis, especially in controversial cases where differential diagnosis from other diseases must be established, but also for a better understanding of the biological behavior of the disease.
The main differential diagnoses of Paget’s disease of the jaws include cemento-osseous dysplasia 31 , 32 , chronic sclerosing osteomyelitis 31 and medication-related osteonecrosis of the jaws 36 . In view of the increasing incidence of the latter, a complex and emerging pathological condition, it is highly relevant to gain further knowledge about pathological entities with similar morphologic characteristics, as is the case of Paget’s disease of the jaws 37 , 38 .
The aim of the present study was to perform a detailed analysis of the histopathological features of Paget’s disease of the jaws observed in a series comprising 31 cases. To our knowledge, this is the largest series of Paget’s disease of the jaws reported to date.
MATERIALS AND METHODS
The study projet was approved by the Ethics Committee of the School of Dentistry of the University of Buenos Aires (# 200201702003 08BA). The study comprised all cases of Paget’s disease of the jaws (n=31) filed in the archives of the Surgical Pathology Laboratory of the Oral Pathology Department, School of Dentistry, University of Buenos Aires, between 1960 and 2018. The microscopic features of the hematoxylin-eosin-stained histological sections were analyzed and recorded, and the clinical and radiographic data available on the filed records were examined.
RESULTS
The 31 retrieved cases of Paget’s disease of the jaws accounted for 0.05% of all oral-maxillofacial pathologies diagnosed at our laboratory in the studied period (58 years).
Mean age was 61 years, age range 44 to 85 years, and frequency peaked in the sixth decade of life. Nineteen cases (61%) were women. The most frequently affected site was the maxilla (13 cases). No information regarding mandibular or maxillary location was available in seven cases, and the disease involved other skeletal bones (polyostotic form) in five cases.
Microscopically, all cases showed the typical trabecular structure: lamellar trabeculae with a mosaic pattern containing multiple compartments. The observed compartments were mostly demarcated by resorption lines (Fig. 1A). Trabeculae were markedly thicker in 24 cases (77%). Twenty cases (64%) showed osteoblastic and osteoclastic activity (Fig. 1B) and 11 cases (35%) showed no cellular activity (Fig.1C). All cases exhibited areas of necrosis evidenced by the absence of osteocytes inside lacunae. The medullary spaces were occupied by fibrous tissue, which was mostly loose and well vascularized. The observed microscopic features were consistent with Paget’s disease of bone. The occurrence of cemento-osseous trabeculae in 15 cases (48%) was a remarkable finding. The latter trabeculae were mineralized structures arranged in the typical mosaic pattern but had rounded and scalloped surfaces with less cellularity, resembling cementum. Some sectors of the surface exhibited fibrillar structures as those described by Cooke 30 (Fig. 1D). Cementicles were observed in 13 cases (42%). The involved tooth was submitted for histopathological examination in two cases, and both submitted teeth were found to exhibit cementum apposition resulting in hypercementosis and ankylosis with the typical mosaic pattern (Fig. 1E). Osteomyelitis was observed in 11 cases (35%), which were clinically and radiographically diagnosed as osteomyelitis associated with Paget’s disease of the jaws. All the cases exhibited thick cemento-osseous trabeculae with multiple compartments and necrosis. An acute/chronic inflammatory process and microbial colonies were observed in the bone marrow (Fig.1F).
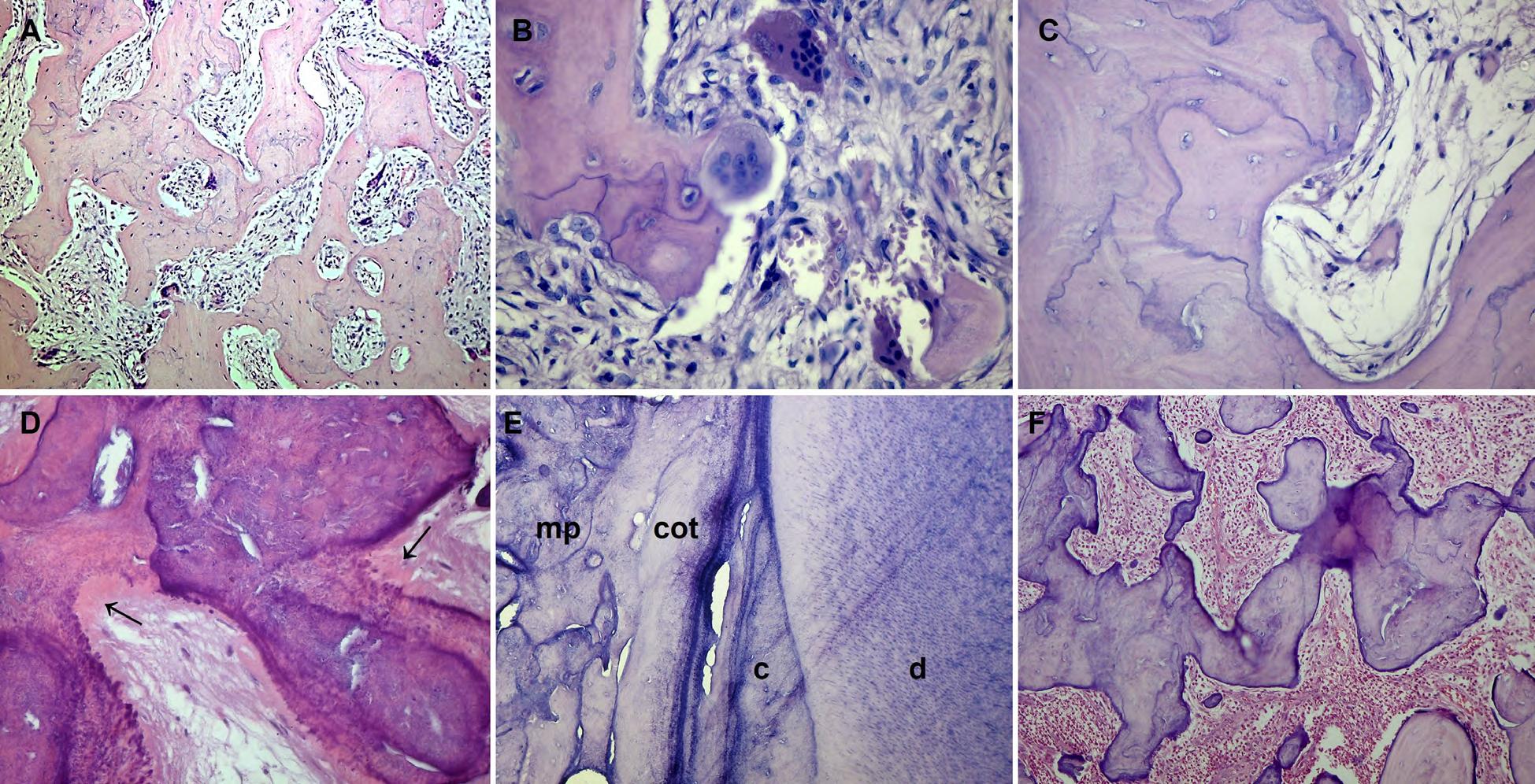
Fig. 1 Photomicrographs of Paget’s disease of the jaws. A. Lamellar bone trabeculae showing a mosaic pattern, and fibrous bone marrow. H-E Orig. Mag. X100. B. Osteoblasts and osteoclasts on the surface of the bone trabecula. H-E Orig. Mag. X400. C. Absence of cells on the surface of the trabecula. H-E Orig. Mag. X400. D. Cemento-osseous trabeculae with a fibrillar surface (j). H-E Orig. Mag. X400. E. Tooth root exhibiting hypercementosis and ankylosis. d: dentine ; c: cement; cot: cemento-osseous trabecula; mp: Mosaic pattern. H-E Orig. Mag. X400. F. Necrotic cemento-osseous trabeculae with multiple compartments and medullary spaces occupied by an inflammatory process. H-E Orig. Mag. X100.
DISCUSSION
Few case series of Paget’s disease of the jaws have been reported in the literature to date; all comprised a small number of cases and were mostly published in the 80’s 29, 33-35 . In 2012, Werner de Castro et al. published a series of 134 cases of Paget’s disease of bone, which included only five cases located in the jaws 36 .
There is no available information on the incidence and frequency of Paget’s disease of the jaws in Argentina. We herein report 31 cases of Paget’s disease of the jaws diagnosed at a single referral center within a period of 58 years, and that accounted for 0.05% of all oral maxillofacial pathologies filed in the laboratory archives. To our knowledge, this is the largest series of cases of this disease reported to date. Sixty-five of the cases in this series were diagnosed before 1980, confirming the decreasing trend in the incidence of the disease worldwide.
In addition to the typical histopathological characteristics of Paget’s disease involving other bones of the skeleton, Paget’s disease of the jaws shows formation of cemento-osseous trabeculae and cementicles. The latter histopathological feature could be misleading, and diagnosis can be confused with other dysplastic and neoplastic diseases affecting the jaws, such as cemento-osseous dysplasia, cementoblastoma, and ossifying cemento-fibroma. These pathologies affect the jaws exclusively; the former is dysplastic, the latter two are tumor lesions of odontogenic origin, and all threes show formation of cemento-osseous trabeculae with a paget-like pattern.
Paget’s disease of bone is infrequent in the jaws. Most studies on this pathological entity reported the clinical and radiographic features, but few analyzed the specific histopathology and possible etiopathogenesis of the disease in this location 29-31 . Rushton (1938) was the first author to report hypercementosis of the teeth in Paget’s disease of the jaws 29 . Lucas (1955) pointed out that the observed hypercementosis could be differentiated from hypercementosis related with other causes by the absence of periodontal ligament and lamina dura; the author also found that hypercementosis becomes evident in the later stages of the disease 30 . Cook (1956) analyzed five teeth with root hypercementosis from patients with Paget’s disease of the jaws, and observed marked cellularity in the newly-formed cementum, which in turn showed signs of remodeling in a mosaic pattern similar to that described in bone tissue. The author also observed nodules of bone fused together by woven bone that had a fibrillar structure on its surface, at right angles to the central nodules 29 .
In our case series, 15 cases (48%) exhibited cemento-osseous trabeculae with marked signs of remodeling in a mosaic pattern, and in line with the aforementioned authors, showed a fibrillar pattern on the surface of the trabeculae. Thirteen cases (42%) showed cementicles, and the two cases submitted with the involved teeth for histopathological evaluation exhibited hypercementosis with tooth ankylosis and the typical mosaic pattern.
It is known that formation of Paget-like trabeculae increases risk of infection. Eleven cases of Paget’s disease of the jaws in our series (36%) showed osteomyelitis, and their microscopic features were similar to those reported in bisphosphonate-related osteonecrosis of the jaws. Our research group found the Paget-like trabecular structure containing multiple compartments to be a distinctive microscopic feature of bisphosphonate-related osteonecrosis 37-38 . Based on this observation, we have posited the existence of an etiopathogenic mechanism that might also explain the necrosis and inflammation seen in Paget’s disease of the jaws. Bisphosphonates induce new bone formation and are therefore used in oncological treatment to limit metastasis-related bone destruction and to treat different bone metabolism alterations. Similarly, a mechanism that remains unknown to date would cause the chaotic bone architecture found in Paget’s disease, favoring necrosis and the subsequent inflammation and invasión of oral microorganisms into the bone.
Of note, we observed a subtle difference between the mosaic pattern of trabeculae in Paget’s disease of the jaws and the Paget-like structure of trabeculae in bisphosphonate-related osteonecrosis of the jaws: in the latter condition the cement lines are regular and linear, following the laminar arrangement of trabeculae, whereas in Paget’s disease of the jaws, they show a scalloped appearance indicating reabsorption. Although diagnosis of both pathological entities is defined based on clinical and biochemical data, in-depth analysis of their microscopic features could contribute to differential diagnosis and provide a better understanding of the biological behavior and pathogenesis of these complex diseases.
All the cases of Paget’s disease ofthe jaws presenting osteomyelitis showed cemento-osseous trabeculae, which were thicker and contained multiple compartments. Formation of cemento-osseous trabeculae is likely reactive to inflammation, and these trabeculae probably have little or no repair capacity.
It must be pointed out that when bone pathologies are in the jaws, they usually have distinct characteristics that are different from those observed when they are located in other bones of the skeleton. This is especially evident, for example, in osteosarcoma of the jaws and medication-related osteonecrosis of the jaws, as well as in Paget’s disease of the jaws. These differences could be attributed to the greater remodeling activity of the jaws due to stimuli of the masticatory forces and to the persistence of and/or coexistence with tissues that have the potential to form cementum-like and dentin-like structures.

