











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
Permalink
INTRODUCTION
Hydrogen peroxide and carbamide peroxide are the agents most often used in tooth bleaching techniques. Hydrogen peroxide is generally used for in-office whitening procedures at concentrations of 35 to 40%, while carbamide peroxide is used in techniques with trays, under a dentist’s supervision, and at lower concentrations of10 to 22% 1-3 . However, these concentrations are higher than recommended by some international control agencies, such as the American Dental Association 4 and the Scientific Committee on Consumer Products 5 of the European Union, which indicate a maximum percentage of 6% hydrogen peroxide in bleaching agents, to guard against possible pulpal damage.
Bleaching can promote some adverse effects, mainly sensitivity and gingival irritation1-3,6,7, with sensitivity being the main and most common symptom, reported by approximately 15-78% of people undergoing this procedure, with intensities ranging from mild to moderate 8 , 9 . The intensity of sensitivity is directly related to the concentration used (the higher the concentration, the greater the sensitivity), and the application time (the longer the time, the greater the sensitivity) 8-11 .
The peroxides used in bleaching techniques release free radicals, which, in turn, release cellular metabolic products (such as ATP and prostaglandins) that excite or sensitize the nociceptors in the pulp 12 . The resulting depolarization followed by repolarization of the sensitive dentinal nerves stimulates pain 12 . It has therefore been recommended that the concentration of peroxide in bleaching agents should be reduced 4 , 5 , and that further research should be conducted on bleaching procedures without peroxide, such as those using ozone (O3) 13-20 .
The ozone molecule, and particularly the hydroxyl radical (OH-) - a non-selective oxidant formed by ozone decomposition - play an important role in the oxidation process. Ozone decomposes in aqueous solutions, triggering the formation of both peroxide radicals (HO 2 -) and hydroxyl radicals (OH-) 21 , 22 . Ozone can break down chromophore groups into smaller molecules, resulting in a tooth whitening effect through a binding, substitution or cleavage mechanism 2 . 3
Although some studies have observed that the isolated use of ozone did not promote effective bleaching16,20,24, others have reported that ozone associated with a high concentration of hydrogen peroxide (37.5% 18 and 38% 13-15 ) during in-office bleaching techniques did so. Ozone applied together with carbamide peroxide in the office 19 or by patients on their own18,19,25 has shown significant results in inducing clinically noticeable color change, in addition to reducing patient-reported sensitivity 14 . These differences in the whitening potential reported for ozone therapy in different studies stem from variations in ozone or peroxide dosages or low concentrations, low sample size, older ozone generation devices, and ozone circulation capacity in the application tray 15 , 19 . Among the protocols used, Ferreira et al. 19 applied office treatments with ozone and carbamide peroxide associated to ozone therapy for 1 hour every 3 days (total 3 applications or 3 hours). These treatments promoted clinically noticeable, acceptable and comparable chromatic changes when 10% carbamide peroxide was applied in a tray for 8 hours daily for 7 days (totaling 56 hours of application). However, the benefits of each whitening treatment should be considered separately, as well as the direct effects of these treatments on tooth structure.
Regarding these effects, ozone gas therapy for tooth bleaching was found to promote a significant reduction in enamel microhardness. Moreover, some bleaching agents with low pH can cause a change in mineral content 18 . Ferreira et al. 19 showed that the pH remains neutral when a carbamide peroxide bleaching agent is associated with ozone for 60 minutes, but they also observed a slight decrease in microhardness values, possibly associated with the release of free radicals. This slight reduction could lead to changes not only in the mineral content of the enamel, but also in the roughness and micromorphology of the enamel, characterized by porosity and erosion.
It is therefore important to evaluate the enamel surface properties after application of ozone therapy for bleaching, to ensure that the bleaching effect provides adequate conditions for sound dental substrate. The aim of this study was to evaluate the effects of a bleaching treatment with 10% carbamide peroxide associated with ozone therapy for in-office use on microhardness, roughness and micromorphology of the enamel surface. The null hypothesis was that there would be no difference in microhardness, roughness and micromorphology of enamel whitened by ozone therapy, carbamide peroxide associated to ozone therapy for in-office use, or 10% carbamide peroxide for use in trays.
MATERIALS AND METHOD
Bleaching Protocols
The bleaching protocols evaluated are shown in Table 1. The ozone concentration in the ozone gas therapy followed protocols adapted from Tessier et al. 25 , Santana et al. 18 , and Ferreira et al. 19 . The pH values for the 10% carbamide peroxide bleaching agent and the ozonized 10% carbamide peroxide were measured in triplicate, at different application times (baseline, 30, and 60 minutes), using a pH meter (MS Tecnopon Equipamentos Especiais, Piracicaba, SP, Brazil).
Table 1 Bleaching protocols used, materials and manufacturers
| Bleaching treatment/Abbreviation | Bleaching protocols | Trade name and manufacturer (city, state, country) |
| Bleaching with 10% carbamide peroxide using a tray/CP | 1 hour a day for 14 days | Opalescence PF 10% - Ultradent (Indaiatuba, SP, Brazil) |
| Bleaching with ozone gas/O | 1 hour every 3 days, for a total of 3 applications | Medplus V Philozon® (Balneário Camboriú, SC, Brazil) |
| Tray bleaching with 10% ozonized carbamide peroxide/OCP | 1 hour every 3 days, for a total of 3 applications | Opalescence PF 10% - Ultradent (Indaiatuba, SP, Brazil) and Medplus V Philozon® (Balneário Camboriú, SC, Brazil) |
Tooth selection
Sixty clean, extracted bovine incisors obtained from a slaughterhouse were stored in a freezer at -18°C no longer than two months before commencing the experimental stage. The teeth were thawed at room temperature, and the roots were removed from the crown with a double-sided diamond disc (KG Sorensen, Barueri, SP, Brazil). The crowns were sectioned to obtain enamel blocks (5.0 mm x 5.0 mm x 3.0 mm). The blocks were embedded in polyester resin (Maxi Rubber, Campinas, SP, Brazil), and polished in a pneumatic electric polisher (Ecomet 250 grinder, Buehler, Lake Bluff, IL, USA) with 600- and 1200-grit sandpaper (Buehler, Lake Bluff, IL, USA), alumina suspension at 0.3 pm (Alfa Micropolish, Buehler, Lake Bluff, IL, USA) and a felt cloth (Buehler, Lake Bluff, IL, USA). The enamel specimens were cleaned in an ultrasonic cleaner with deionized water for 10 minutes to remove any residue from the polishing procedure. Sixty enamel blocks obtained at the end of this stage were selected according to microhardness and surface roughness values. The blocks were then immersed in artificial saliva solution (7 mL for each tooth) (1.5 mMol/L Ca; 50 mMol/L KCl; 0.9mMol/L PO4; 20 mMol/L Tris buffer; pH=7.0), as recommended by Featherstone et al. 26 and modified by Serra & Cury 27 , for 7 days at 37°C in a bacteriological incubator.
Microhardness evaluation
Three Knoop microhardness indentations were made at 150 pm intervals on the upper surface of each enamel sample before applying the treatments, using a microhardness tester (HVS-1000, Panambra, Sao Paulo, SP, Brazil), under a load of 25 g, applied for 5 seconds. The values were tabulated, and enamel blocks with average Knoop microhardness between 350 and 400 kgf/mm2 were selected.
Roughness evaluation
Initial surface roughness was measured with a roughness tester (Suftest SJ-210, Mitutoyo, Suzano, SP, Brazil) on the surface of the samples. The roughness measurement (Ra) was made with a static load of 5 N at a speed of 0.5 mm/s. The cut-off value was 0.25 pm in sequential mode. Three measurements were performed on each sample at different locations, and the arithmetic mean was calculated. The values were tabulated, and enamel blocks with a mean roughness of 0.04 pm ± 0.01 pm were selected.
At the end of this stage, 33 enamel blocks were selected for the experiment (30 for the microhardness and roughness tests, and 3 for the initial micromorphology evaluations).
Tray construction and enamel block positioning
Anatomical molding of the upper arch of a dental mannequin (Prodens, Pronew, Sao Gonzalo, RJ, Brazil) was performed with alginate (Hydrogum, Zhermack, Meier, RJ, Brazil) using a metal mold without the artificial teeth. The alveoli were obliterated with utility wax. Soon after, the mold was cast with microgranulated special type IV plaster (Durone, Dentsply Sirona, Sao Paulo, SP, Brazil). This special plaster model was used to perform the whitening procedures.
The trays were made by positioning replicas of the enamel blocks (made with composite resin 5.0 mm x 5.0 mm x 3.0 mm) on the empty alveoli using sticky wax, with one enamel block positioned in each dental element of the arch (from tooth 35 to 45). A new mold was made with alginate, and cast with stone plaster to make three silicone trays (Cristal PVC, Bioart, Sao Carlos, SP, Brazil) (3.0 mm thick), one tray for each bleaching agent under study. The tray for the group to receive the 10% carbamide peroxide treatment (CP group) was cut at the limit corresponding to the division between the free and inserted gingiva of the mannequin.
In the experimental groups O and OCP (those using 10% carbamide peroxide associated to ozone gas therapy), both the external and internal faces of the plaster model were ground with a number 6 spherical bur coupled to a micromotor in the region at the end of the vestibule bottom. Dense condensation silicone paste (Speedex, Coltene, Rio de Janeiro, RJ, Brazil) was applied with a thickness of 0.5 mm above the dental block replicas, in order to provide space for the circulation of ozone inside the tray. Afterwards, two silicone trays (Cristal PVC, Bioart, Sao Carlos, SP, Brazil) were made in a vacuum plasticizer (P7, Bio-art, Sao Carlos, SP, Brazil), by cutting the tray at the site of the wear in the region at the end of the vestibule. Then, four holes were drilled on the buccal surface and two on the lingual surface of the respective trays, through which to install plastic cannulas (Macrogotas Descarpack Luer Slip, Sao Paulo, SP, Brazil) to allow the ozone to enter through the buccal surface and exit through the lingual surface of the trays. After making the trays on the previously prepared special plaster models, the enamel blocks were removed from the polyester resin, so that the resin could be fixed on a plaster model, thus reproducing the dental arch to be used in performing the whitening techniques (Fig. 1).

Bleaching treatment with 10% carbamide peroxide - CP
A disposable syringe (Biotecmed, Sao Paulo, SP, Brazil) was used to apply 0.02 mL of 10% carbamide peroxide on the surface of the enamel blocks. The
bleaching agent was kept on the enamel surface for 1 hour per day, according to the manufacturer’s recommendations. After this time, the gel was removed from the enamel surface with deionized water for 10 s and dried with gauze. Then, the model was immersed in artificial saliva solution and kept in a humid environment in a bacteriological incubator at 37°C. This cycle was repeated for 14 days. After finishing the applications, the enamel surface was washed with distilled water, and again stored in artificial saliva solution for 24 hours in a 37°C bacteriological incubator, until the final microhardness and roughness evaluations were performed.
Bleaching treatment with ozone - O
An ozone therapy generator (Medplus V Philozon, Camboriú, SC, Brazil) connected to an oxygen cylinder by a standard flow meter (Nogales et al., 2008) was used to perform the experiment. The dose applied was adjusted according to the concentration of the oxygen/ozone gas mixture (mcg/mL), and the action time (min). The ozone concentration was 60 mcg/mL, at an oxygen flow rate of 1 L/ min, according to the manufacturer’s guidelines. The application time was 1 hour every 3 days, for a total 3 applications. The gas was introduced by adapting one end of the cannula to the four holes of the tray in the vestibular region, and the other end of the cannula to the ozone generator equipment. The gas was released from the tray by adapting one end of the cannulas to the tray in the lingual area (Fig. 2), and the other end to the device itself,

which has an integrated vacuum pump for gases. The specimens were kept in artificial saliva solution in a bacteriological incubator at 37°C between the bleaching sessions. After the last session, the blocks were washed with distilled water and again stored in artificial saliva solution for 24 hours in a 37°C bacteriological incubator, until the final microhardness and roughness evaluations were performed.
Bleaching treatment with 10% ozonized carbamide peroxide - OCP
A disposable syringe (Biotecmed, Sao Paulo, SP, Brazil) was used to apply 0.02 ml of 10% carbamide peroxide whitening agent on the buccal enamel surface of the teeth, and cannulas were used to position the previously prepared tray. The tray, together with the plastic cannulas, was connected to the ozone generator, as mentioned above. The 10% carbamide peroxide, together with the designated O protocol, was left on the specimens for 1 hour. This application was repeated every 3 days, for a total three applications. The specimens were kept in artificial saliva solution, in a bacteriological incubator at 37°C between the bleaching sessions. After the last session, the blocks were washed with distilled water, and again stored in an artificial saliva solution for 24 hours in a 37°C bacteriological incubator, until the final microhardness and roughness evaluations were performed.
After the bleaching treatments were completed, the enamel blocks were submitted to final microhardness and roughness analysis, and the enamel micromorphology was evaluated.
Analysis of enamel surface micromorphology
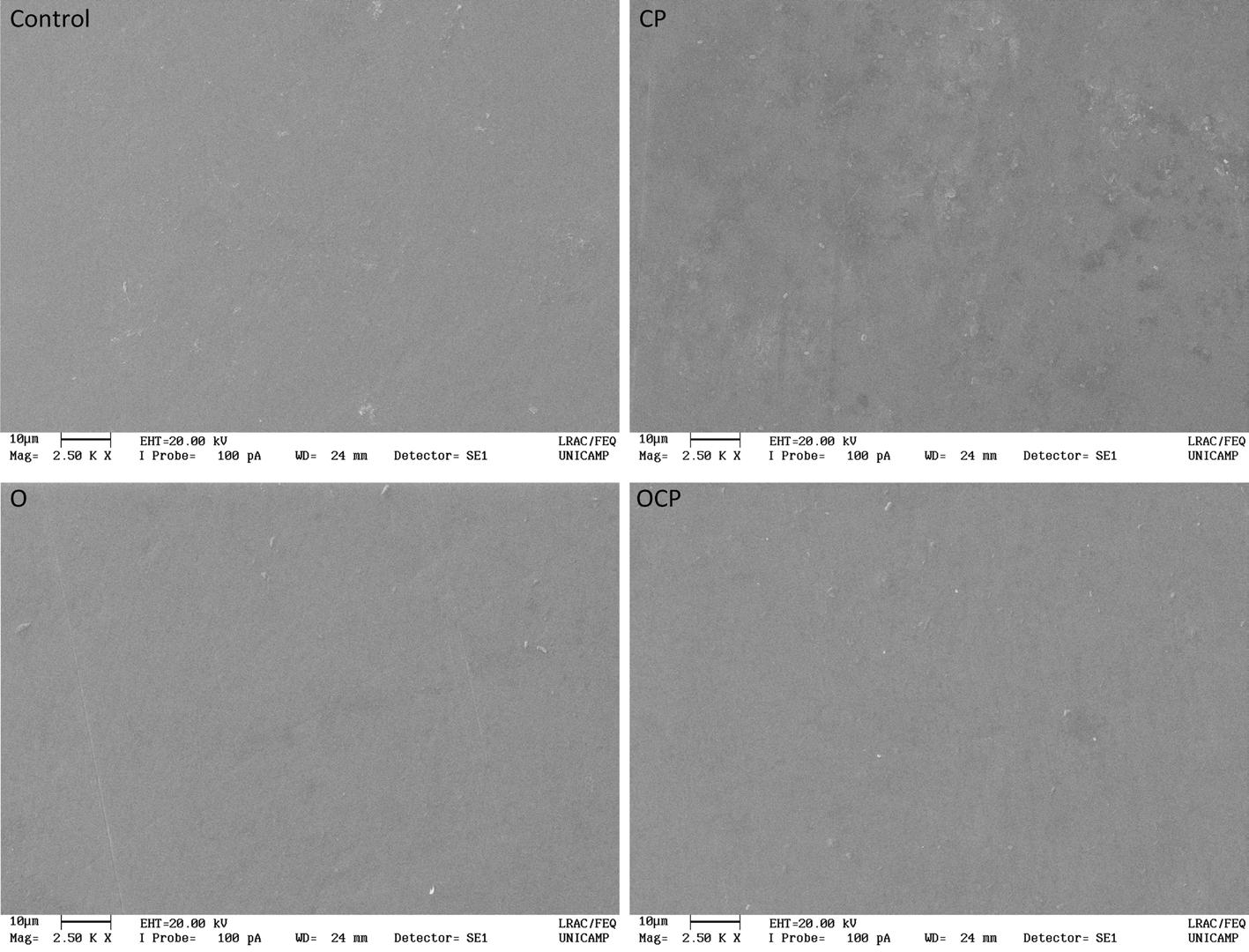
The dental enamel surface of three enamel blocks from each group were analyzed by scanning electron microscopy (LEO Electron Microscopy/ Oxford, Cambridge, England) before and after each whitening treatment. The specimens were subjected to a gold metallization process. Images were obtained at a magnification of 5000x. A single operator evaluated the enamel surface for erosions, irregularities and depressions.
Statistical Analyses
The analyses were performed with the R programming resources 28 at a significance level of 5%. Descriptive and exploratory analyses of the data were made. The exploratory analysis indicated an “outlier” (discrepant value) in the microhardness of the 10% ozonized carbamide peroxide group at baseline (microhardness=395 Kgf/mm2), so this value was excluded from the analyses. Next, a linear mixed model for repeated measures in time (ANOVA for repeated measures in time) and the Tukey-Kramer test were applied. The roughness data did not meet the assumptions of a general linear model (ANOVA), thus calling for an analysis of generalized linear mixed models for repeated measures over time. The percentage increase (in positive values) or decrease (in negative values) of microhardness and roughness between the time periods was also calculated.
RESULTS
The triplicate means of the pH values recorded for the bleaching treatments showed that they remained unchanged throughout the OCP application time, and decreased slightly during the CP application time (Table 2). Although the pH for both treatments was acidic, the OCP treatment was found to be slightly more acidic.
Table 2 pH valúes for 10% carbamide peroxide and 10% ozonized carbamide peroxide according to time
| Treatment | Time | ||
|---|---|---|---|
| Baseline | 30 minutes | 60 minutes | |
| CP | 6.32 | 6.12 | 6.06 |
| OCP | 5.52 | 5.55 | 5.54 |
There was significant interaction between the factors “treatment” and “evaluation time” for the microhardness response variable (p<0.0001). There was no significant difference between the enamel microhardness values for the O and OCP treatments at baseline versus final times (p>0.05), whereas CP promoted decreased microhardness at the end of treatment (p=0.0087), with a mean percentage of 9.94% (Table 3). Treatment with O produced higher enamel microhardness values than the other groups by the end of the treatment (p=0.0169).
Table 3 Mean (standard deviation) microhardness (in Kg/mm2) according to treatment and time
| Treatment | Time | Average percentage (in %) | |
|---|---|---|---|
| Baseline | Final | ||
| CP | 359.40 (19.22) Aa | 323.67 (22.87) Bb | -9.94 |
| O | 356.70 (16.67) Aa | 376.03 (33.87) Aa | 5.41 |
| OCP | 360.04 (12.86) Aa | 338.33 (18.29) Ab | -6.02 |
There was significant interaction between the factors “treatment” and “evaluation time” for the roughness response variable (p<0.0003). In addition, there was a significant increase in surface roughness for CP at the end of the bleaching treatment (percentage increase of 66.66%), as well as greater enamel roughness for this group at the end of the treatment, compared to OCP and O (p=0.0003) (Table 4). The surface micromorphology images showed that CP caused slight irregularities in the enamel micromorphology after the bleaching treatment (Fig. 3).
Table 4 Mean (standard deviation) roughness (in pm) according to treatment and time
| Treatment | Time | Average percentage (in %) | |
|---|---|---|---|
| Baseline | Final | ||
| CP | 0.039 (0.015) Ba | 0.065 (0.025) Aa | 66.66 |
| O | 0.055 (0.012) Aa | 0.037 (0.012) Bb | -32.72 |
| OCP | 0.046 (0.017) Aa | 0.051 (0.022) Aab | 10.86 |
DISCUSSION
Although it has been reported that ozone gas therapy is capable of bleaching by binding, substitution or cleavage mechanisms 21-23 , there is still no consensus regarding the best bleaching protocol to apply ozone therapy for tooth whitening 17 . Moreover, there can be variations in the dosages or concentrations of ozone or peroxide in the ozone generation devices, and in the ozone circulation capacity of the application tray 15 , 19 . The protocol used by Ferreira et al. 19 promoted noticeable, acceptable and perceptible bleaching effects of CP (8 hours daily for 7 days). However, O and OCP treatments were shorter (both applied for 1 hour in the sessions), thus enabling a reduction of 53 hours in the bleaching treatment compared to CP. However, changes may occur in the enamel microhardness, roughness and micromorphology using this protocol, calling for evaluation of these effects. Differences were observed in these enamel surface properties when different treatments were used. We therefore reject the null hypothesis of this study.
The bleaching treatment with CP significantly reduced microhardness, possibly related to the pH of the bleaching agent and the treatment time, even considering that this protocol was adapted from Ferreira et al. 19 . In the present study, CP application time was shorter (1 hour daily for 14 days) than in the study by Ferreira et al. 19 , so we conclude that a shorter application time can promote effective color change 10 , 29 in addition to lowering tooth sensitivity to CP 10 . However, it should be noted that the pH of this bleaching agent is slightly acidic, thereby promoting solubility of the calcium and phosphate present in dental enamel 30 . Furthermore, the change in mineral content can also lead to changes in the enamel surface micromorphology 18 , 31 and increase enamel roughness 32 , as observed in the present study. Treatment with O and OCP did not alter the enamel microhardness. Although OCP was more acidic than CP, the contact between bleaching agent and enamel surface did not promote significant changes, possibly due to the shorter application time (3 hours altogether for OCP versus 14 hours for CP). Thus, the protocol and treatment time may influence enamel properties, considering that all the samples remained immersed in artificial saliva during the time between applications, thus allowing a balance to be maintained between the enamel demineralization-remineralization processes 18 .
However, by the end of the treatment, microhardness was higher in the enamel treated with O than with the other protocols. Ozone decomposes in aqueous solution, releasing free radicals as a result of its high oxidation capacity, and these free radicals can act in the cleavage of organic or inorganic components 18 . Tahmassebi et al. 33 observed that the oxidation of organic compounds present in enamel can lead to increased permeability of the substrate, thereby facilitating the process of remineralization and deposition of calcium and phosphate, of which compounds were present in the artificial saliva used. This mechanism of action may also explain the decrease in O roughness values at the end oftreatment (by 32.72%), contrary to what occurred with the CP and OCP groups. Specifically in relation to CP, the reduction in microhardness at the end of treatment, related to mineral loss, explains the increase in roughness (by 66.66%), confirmed by changes (irregularities) in surface micromorphology, as corroborated by other studies 34 , 35 . These irregularities may be related to byproducts resulting from the oxidizing reaction of the bleaching agent, mainly urea and oxygen. Urea can denature proteins present in organic portions of the tooth structure 36 , 37 , and has the potential to penetrate the enamel, affecting not only the surface but also the interprismatic portion of the enamel. Urea penetration may thus contribute to higher enamel permeability and microstructural changes 34 . As for OCP, although it was associated to the ozone application, its contact with the enamel surface may have led to increased roughness (by 10.86%); however, micromorphological changes were not observed, possibly due to the use of ozone therapy.
Ozone therapy for in-office bleaching did not cause changes in enamel microhardness or surface micromorphology. It led to greater surface smoothness, with a shorter treatment time, compared to the conventional bleaching procedure using tray-delivered carbamide peroxide. This makes it safer in terms of changes in enamel surface properties. However, ozone application requires greater control and the use of a specific tray to prevent inhalation. Further studies are therefore needed to ensure a protocol that is safe, effective, and more convenient for both patient and professional.
It can be concluded that treatment with 10% carbamide peroxide for use in trays changed enamel surface properties more than treatments with ozone or with 10% ozonized carbamide peroxide for use in the office. Gaseous ozone therapy for bleaching treatment, with or without carbamide peroxide, maintained the mechanical and physical properties of microhardness and micromorphology of the enamel surface, and either maintained or reduced surface roughness, compared to the conventional tray-delivered carbamide peroxide whitening treatment.

