











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
Permalink
INTRODUCTION
One of the main aims of endodontics is to provide obturations with three-dimensional sealing of the root canals as a basis for successful treatment 1-2 . However, three-dimensional sealing is not always easy to achieve. Surgical shaping cannot always adapt to the wide range of existing tooth anatomies 3-8 , and chemical preparation does not always eliminate 100% of the contents of the main, lateral, accessory and recurrent canals or apical deltas 9-12 . Successful treatment requires extensive knowledge of materials and different techniques to achieve proper obturation of the entire volume of the root canal system.
For years, obturation techniques used cold-laterally compacted gutta percha cones as the main component, sealed with cements, usually of acid-base composition. Later, techniques were developed for gutta percha mechanical plasticization or direct injection into the system. These changes in canal-sealing techniques were mainly motivated by the need to ensure a 3D seal, i.e., an obturation mass without voids, with gutta percha and/or sealer filling any lateral and/or accessory canals 13-15 .
When 3D sealing is not successful, voids form. Voids are either closed, when they are within the obturation mass, or open, when in contact with the dentin wall. Open voids may connect to the periodontal space through the dentinal tubules. The presence of voids reduces the quality of the final obturation, promoting an environment in which microorganisms can survive, and connection between the periodontal space and the interior of the root canal system. This is why it is so important to ensure a three-dimensional seal, without voids or spaces in which bacteria may develop 16 .
Currently, with the advent of bioceramic sealers, the concept of obturation has changed. Gutta percha has ceased to be the main component, having been replaced by the sealer itself, which has excellent mechanical and biological properties 17-18 .
These new techniques usually use single, more tapered gutta percha cones that almost exactly fit the root canal that was prepared and shaped using rotary and/or oscillatory instruments 19 .
In 2018, Kim proposed an obturation technique based on the use of a bioceramic material with a single gutta percha cone, to which vibration was applied. The vibration transfers ultrasound mechanical energy through a cotton plier that is holding the gutta percha cone inside the root canal, thereby transferring the energy to the bioceramic sealer. This eliminates voids or bubbles, and enhances sealer fluidity, enabling it to penetrate canals that are difficult to access. This technique provides three-dimensional sealing thanks to the sealer rather than the gutta percha 20 .
X-ray micro-CT scanning is an imaging technique based on X-ray absorption by different types of tissues or materials. It can be used to observe and analyze ex vivo samples on a very small scale without causing deterioration 21 . Specimens are positioned in the micro-CT scanner with a holder. Scanning settings (voltage, amperage, rotation, filter, pixel size, grey-scale density, image format, among others) are established, and multiple 2D images are taken while the sample rotates 180° or 360° on its own axis, as programmed. Software is used to recognize the images and convert them into a three-dimensional volume. The volumes thus obtained enable observation, measurement and calculation of many specimen properties, such as volume, surface area, density, presence or absence of voids, etc 22-33 . Identifying the presence, size, type and location of voids in an endodontic obturation is of great clinical importance because it enables evaluation of the three-dimensionality of the sealing techniques, which can be related to the likelihood of healing periradicular lesions. Micro-CT scanning is the only technique that provides images in which the above parameters can be measured without destroying or cutting the specimens. It is important to avoid cutting specimens because doing so may smear the obturation material, preventing proper evaluation 22 . The possibility of observing voids as small as 7 pm enables different sealers and sealing techniques to be studied and compared with the aim of improving obturation three-dimensionality.
The aim of this study was to analyze by micro-CT the presence of voids in the root canal obturation of lower single-rooted premolars prepared using the single cone and ultrasound vibration technique.
MATERIALS AND METHOD
Specimen preparation
This study used 20 single-rooted lower premolars extracted for orthodontic and/or periodontal reasons, straight, with mature apices and caries-free root portion. Retroalveolar X-rays were taken of all specimens in the direction of proximal faces and free faces to verify that they had only one root canal.
Any specimens with more than one root canal were excluded from the sample.
Included specimens were opened at the level of the clinical crown using appropriately sized stone and round bur. Following root canal exposure, catheterization was performed with #10 K-file (Dentsply Maillefer, Switzerland), and opening rectification with EndoZ bur (Dentsply Maillefer, Switzerland) to eliminate any retentive angles. Accesses were prepared with the Sx instrument of the Protaper Gold system (Denstply Maillefer, Switzerland), accessing the cervical and middle thirds of each sample. Next, working length was established by inserting a #15 K-file (Dentsply Maillefer, Switzerland) into the canal until the tip of the file could be seen to emerge from the apical end of the root. That length was measured, and 0.5 mm subtracted from it. The resulting value was recorded in a table as working length (WL).
Surgical preparation was performed with Protaper Gold System instruments S1, S2, F1 and F2, all at working length. Chemical preparation was performed by irrigating with 2.5% sodium hypochlorite between instruments, and final irrigation with 17% EDTA and again 2.5% sodium hypochlorite, alternating rinses with distilled water between the two solutions. Root canals were dried with sterile paper points.
Obturation was performed with size 25/04 gutta percha cones and bioceramic endodontic sealer BIOC Sealer (Angelus), using the single cone technique. The cones were selected and tested prior to obturation, to confirm that they reached the working length. In both groups, the bioceramic sealer was injected through its applicator tip, from the apical end towards the crown portion. As it filled the root volume, the tip was moved backwards towards the crown end up to the cervical third, where it was removed, and the previously selected gutta percha cone was inserted. In Group 1 (without vibration), the gutta percha cone was cut with a hot-tipped instrument and immediately compacted vertically. The pulp chamber toilette was performed and temporary obturation (Cavit 3) applied. In Group 2 (with vibration), ultrasound vibration was applied by holding the gutta percha cone that had been inserted in the root canal with a cotton plier that was made to vibrate with ultrasound for 3 periods of 3 seconds each. Then, the cone was cut with a hot-tipped instrument and immediately compacted vertically. The pulp chamber toilette was performed and temporary obturation (Cavit 3) applied.
The specimens were sent to the Department of Diagnostic Imaging, Micro-CT scan Service, Facultad de Odontología, Universidad de Buenos Aires, for scanning and analysis.
Acquisition and reconstruction
A SkyScan 1272 micro-CT scanner (Bruker-microCT, Kontich, Belgium) was used for image acquisition. The specimens were positioned with their major axis in vertical direction. Due to the size of the teeth, two or three scans were performed and then automatically combined during reconstruction. The following parameters were used for image acquisition: 90 kV, 100 pA, pixel size 12 pm, grey-scale density 0.5, rotation 180, filter Al 0.5 + Cu 0.038, TIFF format.
The images were reconstructed using Nrecon software version 1.7.3.1, adjusting the parameters to show the specimens as clearly as possible.
Image analysis
Images were analyzed using CTAN v1.17 software (Bruker, Kontich, Belgium). Coronal and apical limits were established on each specimen to mark the extent of the area to be studied, and three thirds were established: apical, middle and cervical, all with the same number of slices. The protocol followed was previously published by our working group(34). Presence of voids in the whole tooth (global) was determined, after which the global volume of open and closed voids was analyzed in each tooth and each third.
Statistical analysis
Numerical datasets were described by the following measures: mínimum (min), maximum (Max), mean (Me), median (Md), standard deviation (SD), first quartile (Q1) and third quartile (Q3). To compare quantitative data between two groups, Student’s t-test for grouped data (parametric) or Mann-Whitney’s U-test (non-parametric) were applied, as appropriate. Quantitative data were compared between groups using the Kruskal-Wallis test (non-parametric), followed by post-hoc comparisons with the Conover method. Non-parametric tests were used when the conditions of normality or homoscedasticity were not met. To evaluate the assumption of normality, the D’Agostino-Pearson test was used. Homoscedasticity was analyzed by F or Levene tests when two or three groups were compared, respectively. A p-value lower than 0.05 was considered significant. MedCalc software versión 20.215 (MedCalc Software Ltd., 2023) was used.
RESULTS
Micro-CT scans showed presence of closed and open voids in both groups ( Fig. 1A-B ).
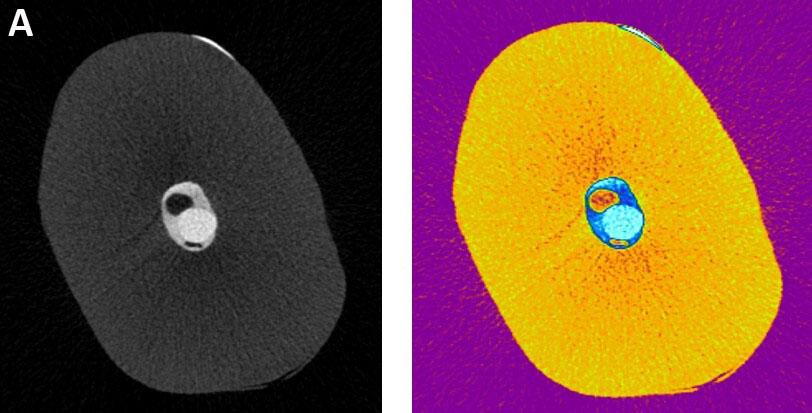
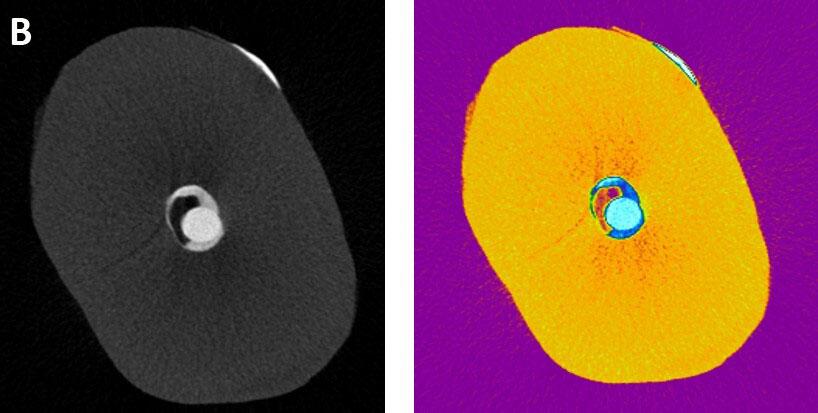
Fig. 1 Micro-CT images, with original colors and contrast, show presence of voids in the endodontic obturation. A) closed voids and B) open voids.
Volume of closed voids
Comparison of the global volume of closed voids between groups showed no significant difference; Group 1 without vibration: 0.003 (0.0069) / Group 2 with vibration: 0.004 (0.006). Values expressed as mean (SD) ( Fig. 2 ).
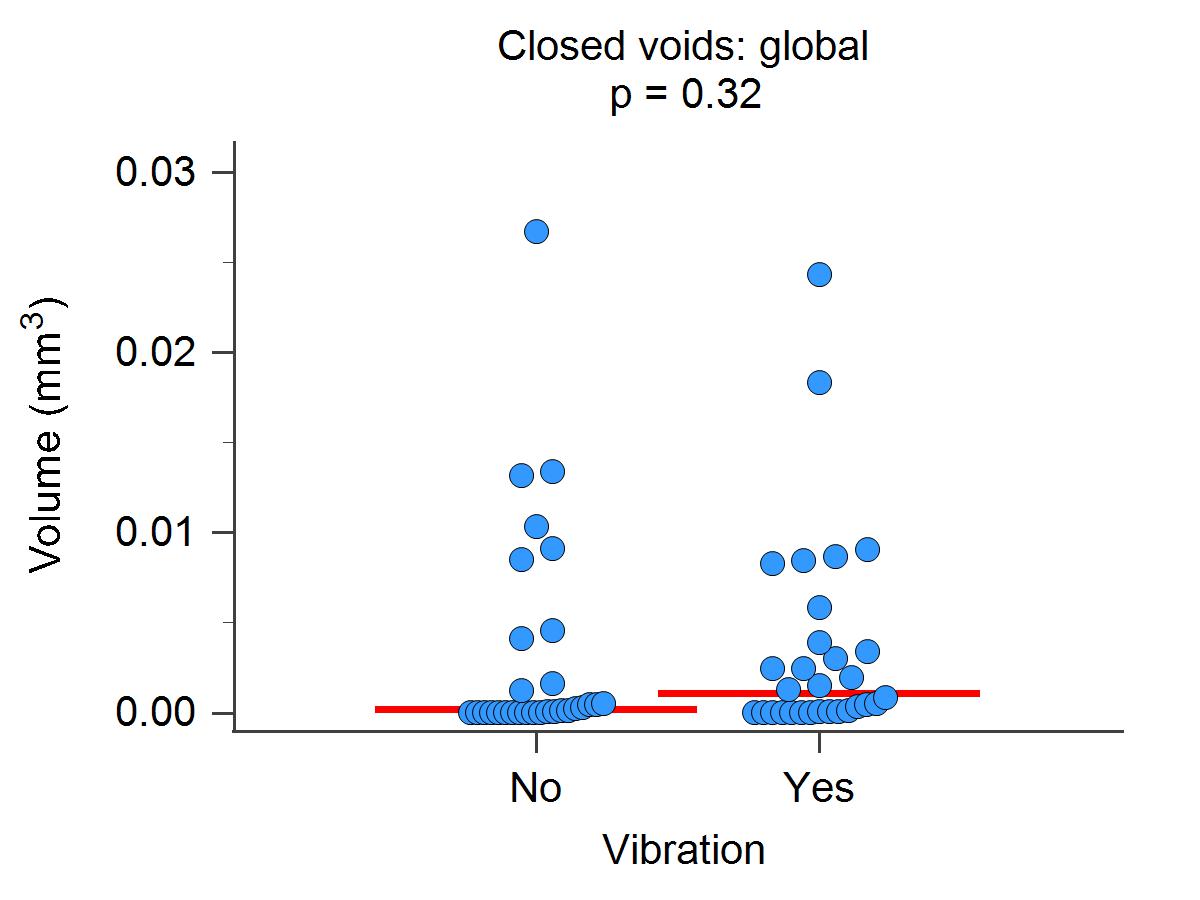
Fig. 2 Global volume of closed voids. Scatter diagram. Horizontal red line: median. p: Mann-Whitney’s U-test.
In both groups, the volume of closed voids differed significantly between thirds (p < 0.05), with the cervical third having the highest volume of voids ( Fig. 3 A and B ).
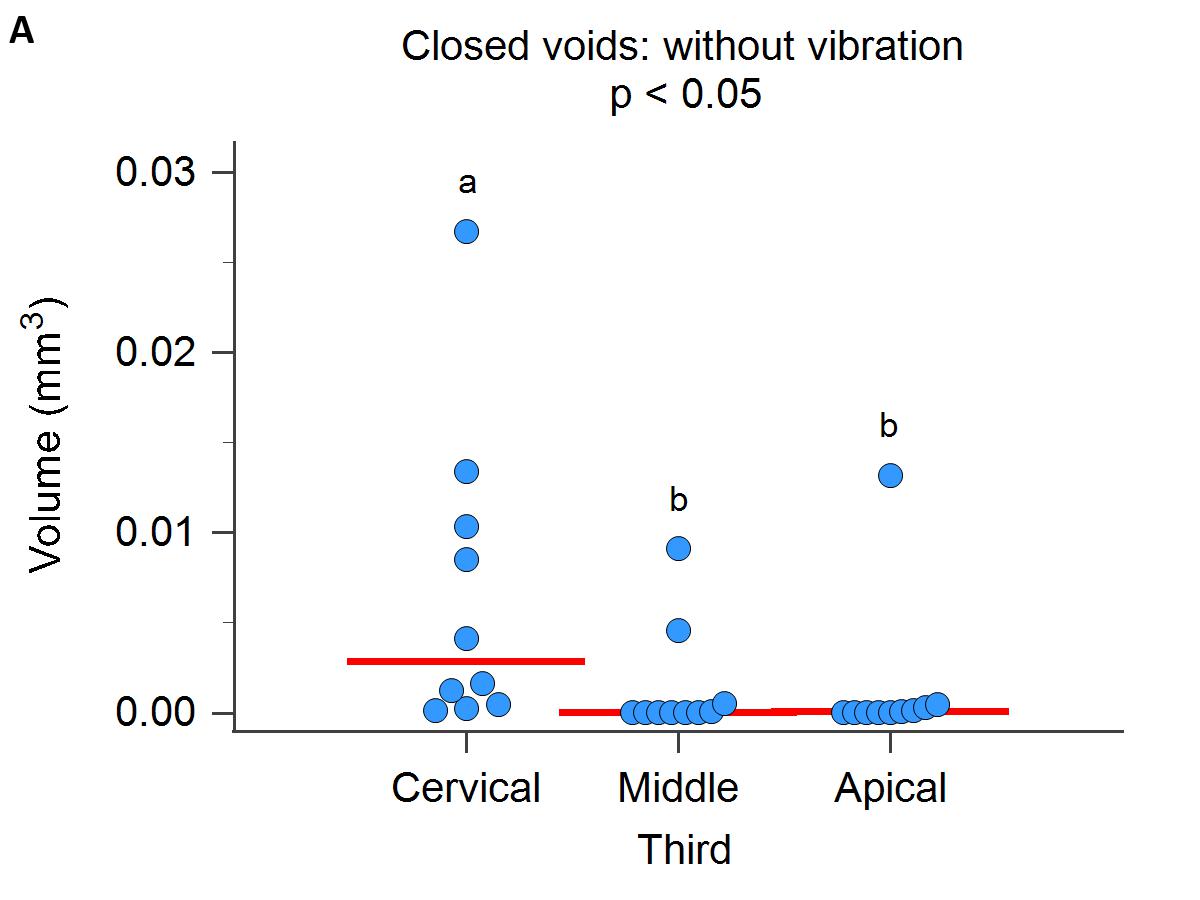
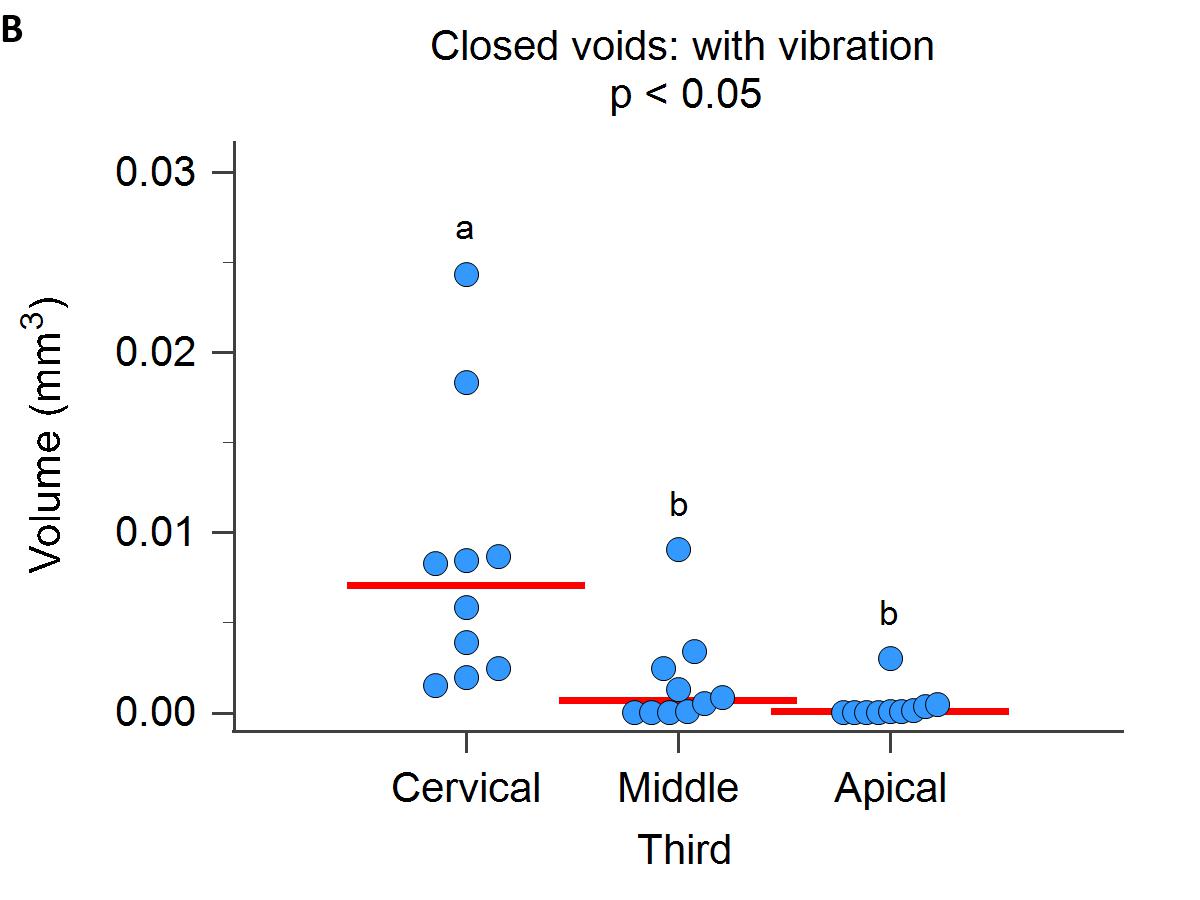
Fig. 3 Volume of closed voids according to third. A) Group 1, Without Vibration, and B) Group 2, With Vibration. Scatter diagram. Horizontal red line: median. p: Kruskal-Wallis test. Different letters indicate significant differences in post-hoc comparisons (Conover).
The volumes of closed voids per group, global and per third, are set forth in Table 1 .
Table 1 Volume of closed voids in treatments without and with vibration, in each third and global
| Volume of closed voids (mm3) | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Third | Vibration | p* | |||||||||||||
| No | Yes | ||||||||||||||
| N | min | Max | Me | Md | SD | Q1 - Q 3 | N | min | Max | Me | Md | SD | Q1 - Q 3 | ||
| Cervical | 10 | 0.000 | 0.027 | 0.007 | 0.003 | 0.008 | 0.000 - 0.010 | 10 | 0.002 | 0.024 | 0.008 | 0.007 | 0.007 | 0.002 - 0.009 | 0.39 |
| Middle | 10 | 0.000 | 0.009 | 0.001 | 0.000 | 0.003 | 0.000 - 0.001 | 10 | 0.000 | 0.009 | 0.002 | 0.001 | 0.003 | 0.000 - 0.002 | 0.35 |
| Apical | 10 | 0.000 | 0.013 | 0.001 | 0.000 | 0.004 | 0.000 - 0.000 | 10 | 0.000 | 0.003 | 0.000 | 0.000 | 0.001 | 0.000 - 0.000 | 0.69 |
| Global | 30 | 0.000 | 0.027 | 0.003 | 0.000 | 0.006 | 0.000 - 0.004 | 30 | 0.000 | 0.024 | 0.004 | 0.001 | 0.006 | 0.000 - 0.004 | 0.32 |
The volumes of open voids per group, global and per third, are set forth in Table 2 .
Table 2 Volume of open voids in treatments without and with vibration, in each third and global
| Volume of closed voids (mm3) | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Third | Vibration | p* | |||||||||||||
| No | Yes | ||||||||||||||
| N | min | Max | Me | Md | SD | Q1 - Q 3 | N | min | Max | Me | Md | SD | Q1 - Q 3 | ||
| Cervical | 10 | 4.339 | 13.062 | 8.378 | 7.502 | 3.139 | 5.459 - 10.717 | 10 | 6.069 | 10.916 | 8.565 | 8.652 | 1.822 | 6.493 - 10.465 | 0.87# |
| Middle | 10 | 2.102 | 5.858 | 3.459 | 3.155 | 1.210 | 2.531 - 4.327 | 10 | 2.584 | 5.974 | 3.784 | 3.313 | 1.165 | 3.083 - 4.054 | 0.55# |
| Apical | 10 | 1.204 | 3.274 | 1.706 | 1.521 | 0.613 | 1.340 - 1.837 | 10 | 1.004 | 2.142 | 1.555 | 1.496 | 0.356 | 1.440 - 1.758 | ≈1 |
| Global | 30 | 1.204 | 13.062 | 4.514 | 3.489 | 3.447 | 1.837 - 5.858 | 30 | 1.004 | 10.916 | 4.635 | 3.313 | 3.215 | 1.758 - 6.493 | 0.80* |
Global volume of open voids was 4.514 (3.447) in Group 1, and 4.635 (3.215) in Group 2; values expressed as mean (SD); without significant differences. ( Fig. 4 ).
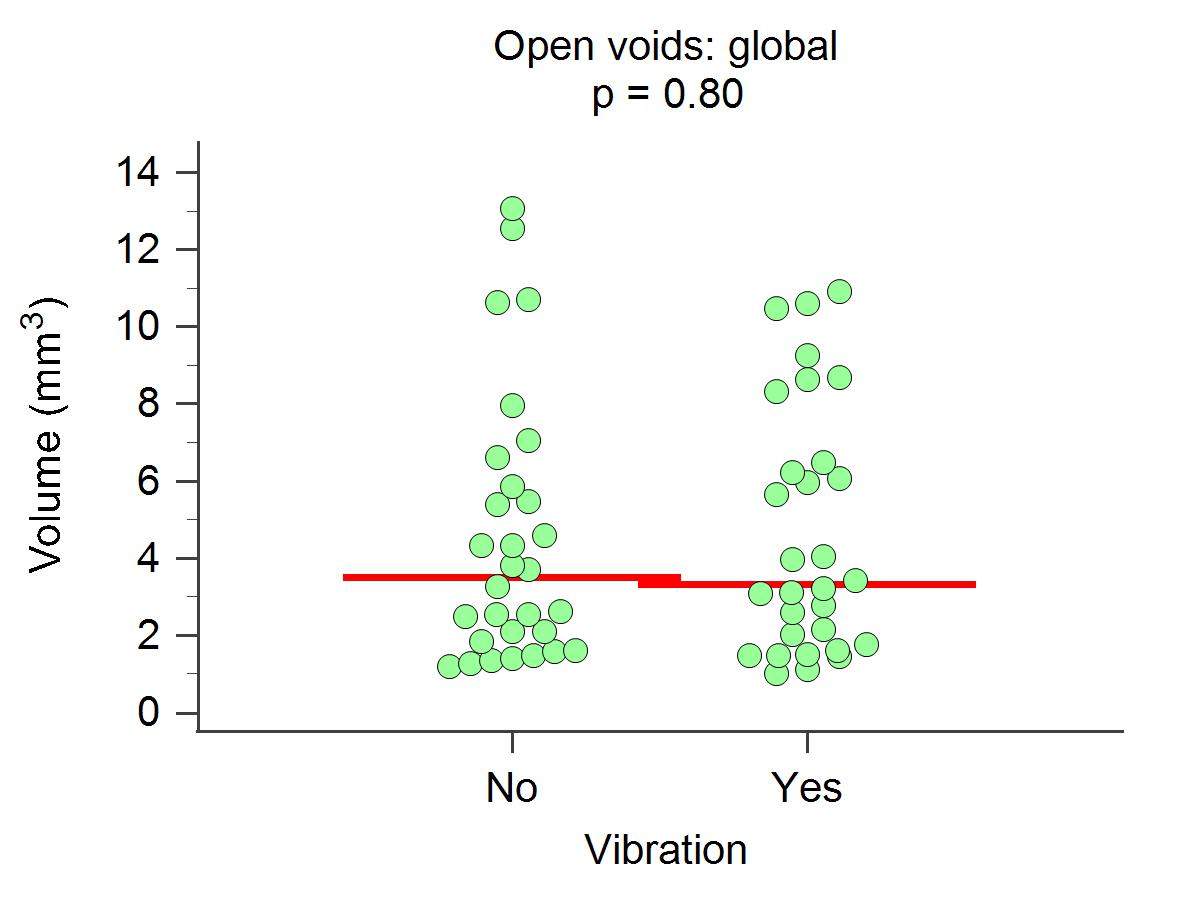
Fig. 4 Volume of open voids according to treatment. Scatter diagram. Horizontal red line: median. p Mann-Whitney’s U-test.
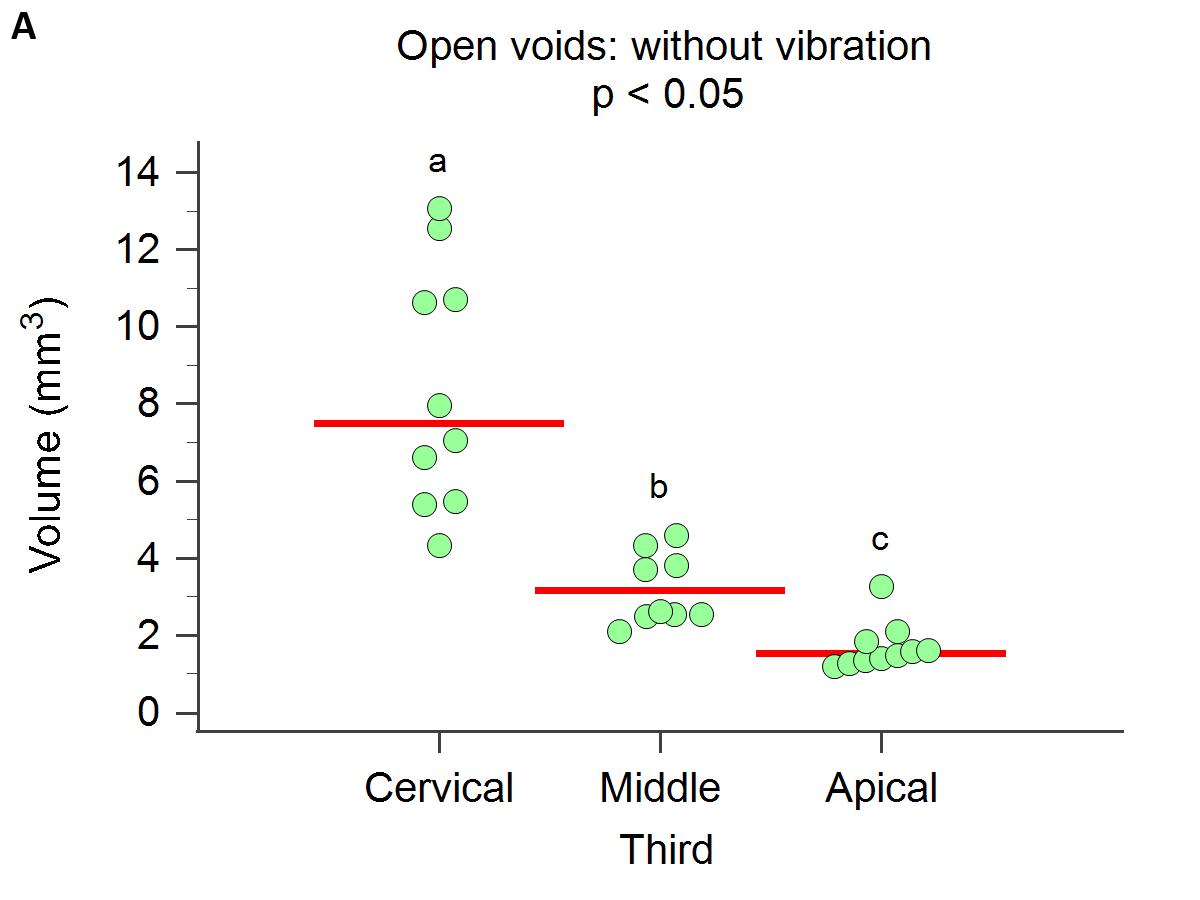
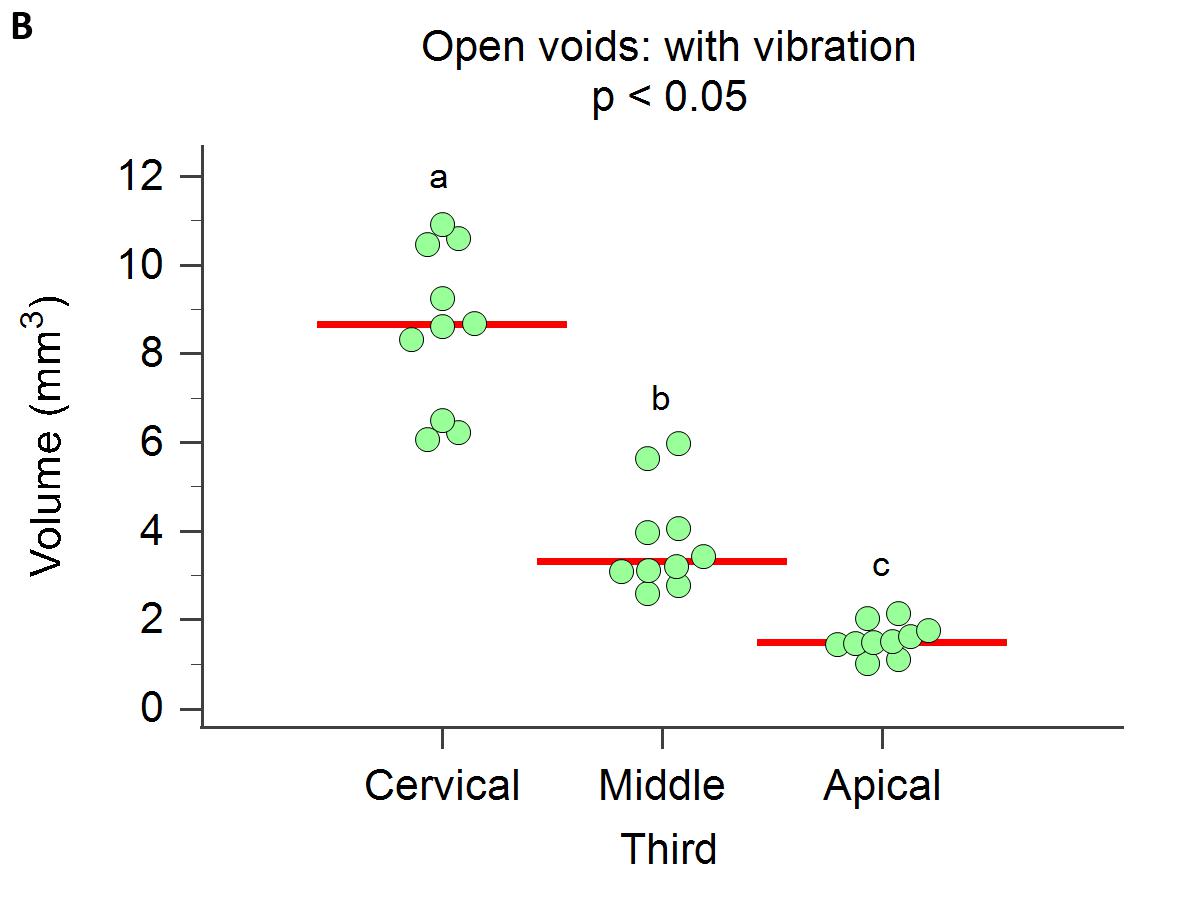
The volume of open voids differed significantly between thirds (p < 0.05), both in the group without vibration ( Fig. 5 ) and in the group with vibration ( Fig. 5 ). In both cases, the cervical third had the highest volume of voids and the apical third had the lowest.
Total volume of voids
In Group 1, global volume of voids ranged from 1.204 to 13.076 mm3, with a median (Q1-Q3) of 3.489 (1.850 - 5.867) and a mean (SD) of 4.517 (3.449). In Group 2, it ranged from 1.007 to 10.919 mm3, with a median (Q1- Q3) of 3.313 (1.758 - 6.499) and a mean (SD) of 4.638 (3.218) ( Fig. 6 ). There was no significant difference between the groups without and with vibration ( Table 3 ), either within the thirds studied: cervical (p = 0.87), middle (p = 0.55) and apical (p ~ 1), or global (p = 0.80).
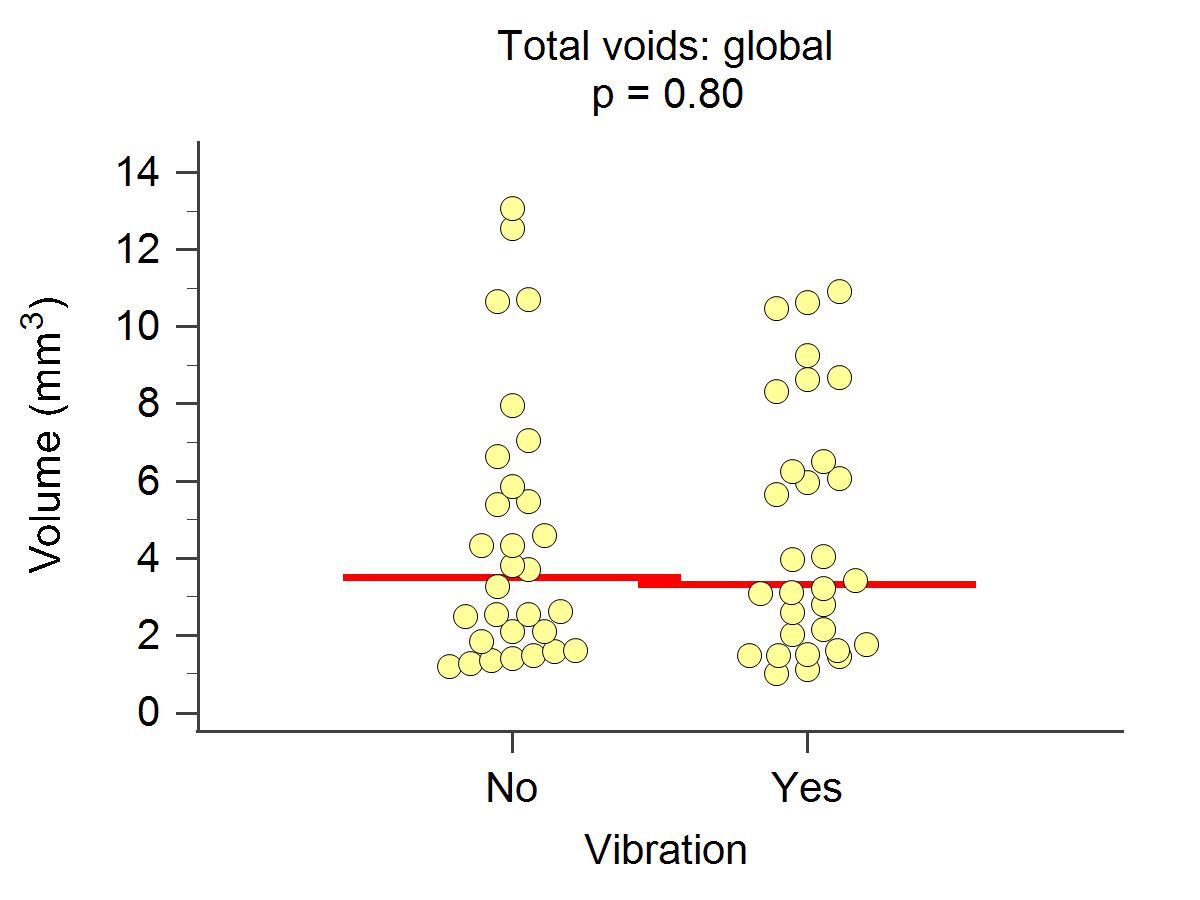
Fig. 6 Total volume of voids according to treatment. Scatter diagram. Horizontal red line: median. p: Mann-Whitney’s U-test.
The total volume of voids differed significantly ( Fig. 7B ). In both cases, the cervical third had the between thirds (p < 0.05), both in Group 1 Without highest volume of voids, and the apical third had the Vibration ( Fig. 7A ) and in Group 2 With Vibration lowest.
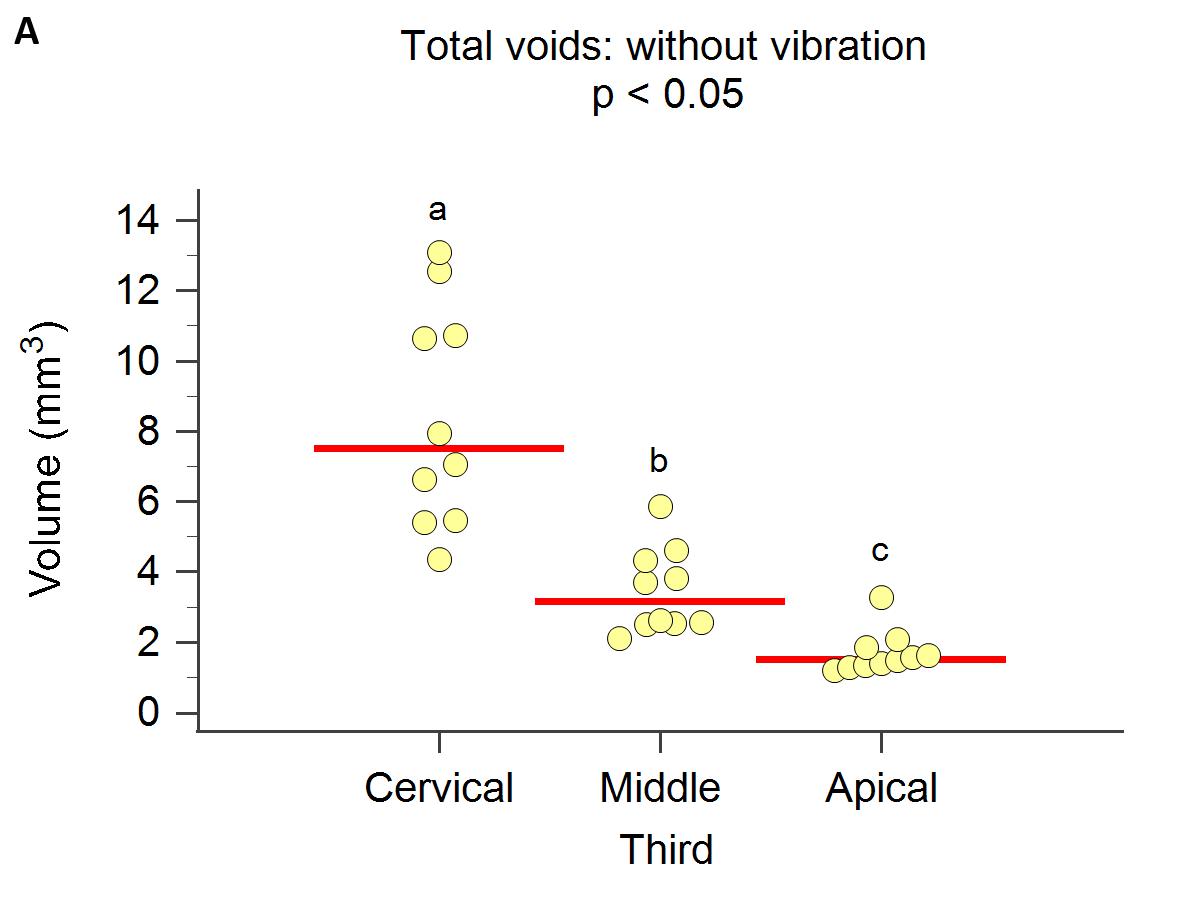
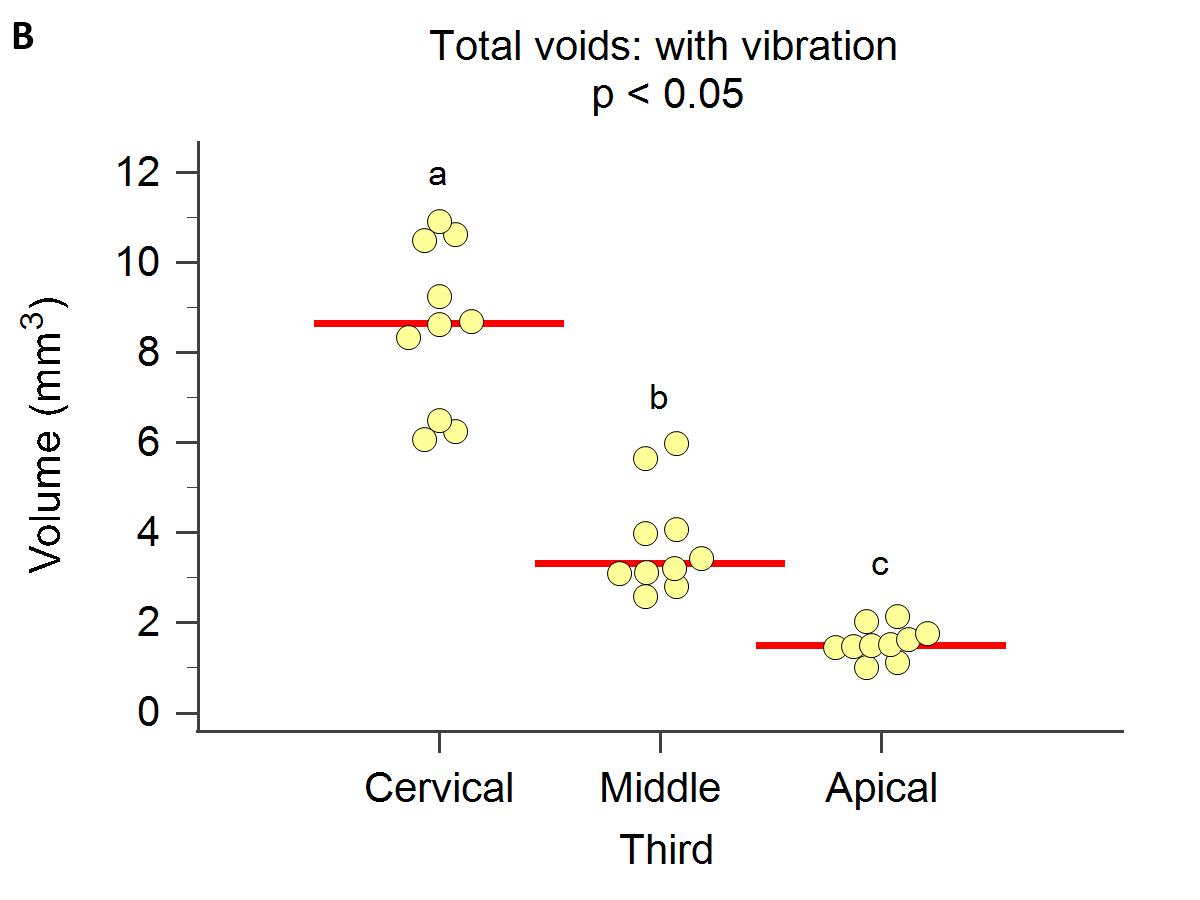
Fig. 7 Total volume of voids according to thirds. A) Group Without Vibration and B) Group With Vibration. Scatter diagram. Horizontal red line: median. p Kruskal-Wallis test. Different letters indícate significant differences in post-hoc comparisons (Conover).
Table 3 Total volume of voids in treatments without and with vibration, in each third and global
| Volume of closed voids (mm3) | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Third | Vibration | p* | |||||||||||||
| No | Yes | ||||||||||||||
| N | min | Max | Me | Md | SD | Q1 - Q 3 | N | min | Max | Me | Md | SD | Q1 - Q 3 | ||
| Cervical | 10 | 4.340 | 13.076 | 8.384 | 7.508 | 3.139 | 5.463 - 10.717 | 10 | 6.077 | 10.919 | 8.573 | 8.655 | 1.820 | 6.499 - 10.483 | 0.87# |
| Middle | 10 | 2.102 | 5.867 | 3.461 | 3.155 | 1.212 | 2.531 - 4.332 | 10 | 2.584 | 5.974 | 3.786 | 3.313 | 1.166 | 3.083 - 4.056 | 0.55# |
| Apical | 10 | 1.204 | 3.274 | 1.707 | 1.521 | 0.614 | 1.340 - 1.850 | 10 | 1.007 | 2.143 | 1.555 | 1.496 | 0.355 | 1.440 -1.758 | ≈1* |
| Global | 30 | 1.204 | 13.076 | 4.517 | 3.489 | 3.449 | 1.850 - 5.867 | 30 | 1.007 | 10.919 | 4.638 | 3.313 | 3.218 | 1.758 - 6.499 | 0.80* |
DISCUSSION
Many different obturation techniques are currently in use, all of which seek to achieve a three-dimensional seal that will increase the likelihood of successful endodontic treatment, free from recontamination. One of the most popular techniques in recent years
uses a bioceramic as the main material, along with a more tapered gutta-percha cone that matches the last instrument used. In 2018, Kim introduced a variation of this technique by adding the use of ultrasound to make the gutta percha cone vibrate, which transmits the waves to the sealer, thereby improving its flow towards the more irregular parts of the root canal 20 . The present study used micro-CT scans to evaluate 20 teeth obturated with bioceramic sealer and single, more tapered cone. Ultrasound was used to apply vibration to half the specimens. Statistical data showed no significant difference in sealing capacity between techniques. There were, however, differences between the thirds evaluated. As expected, the cervical third had the most voids, regardless of the obturation technique, because it contains more sealer due to the anatomical change in the canal, and the gutta percha cone has poorer fit. The data recorded in the current study are consistent with the report published by Kim et al. in 2018 20 , which found no significant difference between groups with and without vibration, although many sealer-free spaces (voids) were observed, mainly in the cervical third, also in agreement with the current study. Iglecias et al. 28 also reported similar results to the current study. They performed single-cone obturations and continuous wave obturations. Micro-CT analysis showed no difference between groups regarding the presence of voids, except in the cervical third.
Ho et al . 32 conducted a study observing endodontically treated samples obturated using different techniques (cold lateral condensation, hot vertical condensation and thermoplasticization by ultrasound). The amount of gutta percha present in each sample was evaluated. The results showed that vertical compaction and ultrasound thermoplasticization achieved comparable obturation qualities with gutta percha in the canal system, with significantly higher density than the samples obturated using cold lateral condensation. This demonstrates better results with the use of ultrasound applied on the gutta percha, reducing voids in the mass, but the article does not specify results on the evaluation of the presence of voids in the endodontic sealer.
The data reported by Somma et al. 35 in 2011 on the evaluation of three different sealing methods also agree with the current study. They analyzed two thermoplasticization techniques (Thermafill and System B) and the single cone technique, by means of 19.1 pm pixel size micro-CT scan. All measurements found similar values for the quantity and distribution of voids and the percentage of occupation of the endodontic space, regardless of the technique.
In 2014, though without using ultrasound, Kele§ 36 et al. measured the volumes of filling and voids in oval root canals by means of 12.5 pm micro-CT. They found that in the apical third, there was no difference between cold lateral compaction and hot vertical compaction techniques, but in the other two thirds, there was a difference in favor of hot compaction.
In 2021, Pérez-Alfayate et al. 30 analyzed the obturation of 200 lower molars with curved roots, using six sealers (AH Plus Thermafil, GuttaCore, GuttaFusion, Cold Side Compaction, AH Plus and EndoSequence BC sealer). Half of the samples from each group were activated with an Endoactivator sonic system tip size 25/06. Three sections were cut from each molar, representing the cervical, medium and apical thirds. Images taken with confocal laser microscope and operative microscope showed no statistically significant differences between sealers, techniques or thirds. It was concluded that the use of sonic activation was unrelated to the three-dimensional seal of the obturation, at least according to the data recorded under fluorescent laser and operative optical microscopes. These results are consistent with the present study.
Ba§er Can et al. 29 also used micro-CT to evaluate 30 single-rooted teeth obturated with EndoREZ, Activ GP or AHplus with gutta-percha. The images were acquired at 13.68 pm and showed significantly more voids in the apical third with Activ GP than with the other two techniques (EndoREZ or AHplus and gutta percha). As in the current study, micro-CT scans enabled determination of whether there were significant differences between different obturation methods.
Celikten et al. 19 evaluated and compared the presence of voids in endodontic obturation with different sealers (EndoSequence BC Sealer, Smartpaste bio, Activ GP and AH Plus) by means of 13.47 pm pixel size micro-CT scans. A large quantity of voids was found in the samples obturated with bioceramics, but there was no statistical difference between them, or compared to the other sealers. This paper suggests that micro-TC scanning is essential for evaluating this type of parameters.
Huang et al. 27 evaluated two endodontic sealers (EndoSequence BC sealer and AH Plus) for obturation of lower premolars. Although the SEM study showed that both sealer were better adapted at crown level, micro-CT scans showed the presence of closed voids within the sealer mass, with no difference between them. Moreover, the number of voids in the cervical third was significantly higher than in the other two thirds, in direct relation to the oval anatomy of root canals in these thirds. These results support the current study.
All of the above demonstrates the importance of using technology that enables parameters to be assessed at very high resolutions.

